Drop The Beat
Bone Dance
Is It A Pheo?
Better Safe Than Sorry
Pimple Poppin'
100
62y M presents to clinic after ED visit for cellulitis. His infection is resolved. He asks about his abnormal EKG results found in the ED. Denies chest pain, dyspnea, presyncope/syncope.
BP 118/77 HR 78 O2 98%
Name the diagnosis and next step for management.
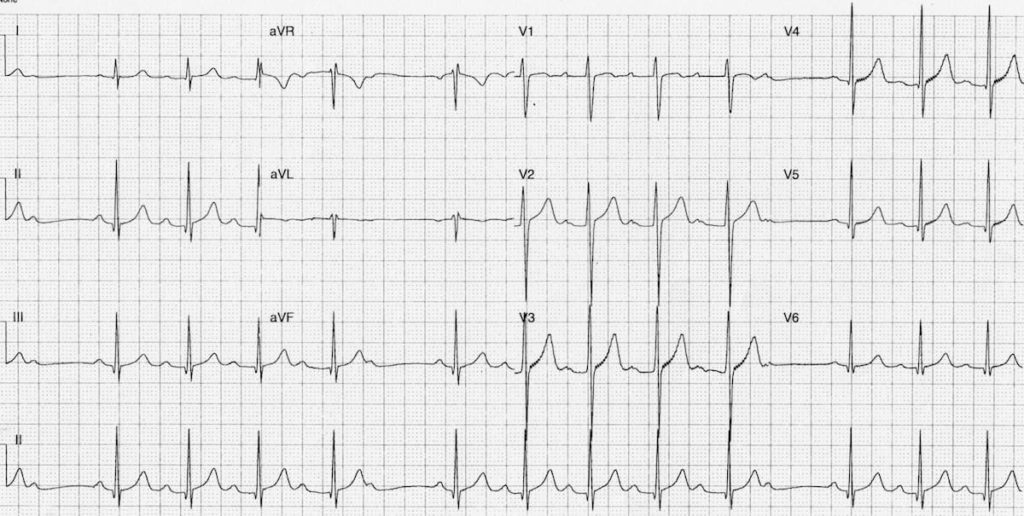
2nd Degree Mobitz I - Wenckebach
No pacemaker required. Evaluate for reversible causes.
Beta blockers, calcium channel blockers, digoxin, adenosine, antiarrhythmic drugs
Cardiac Surgery
Electrolyte Abnormalities
Ischemia, Cardiomyopathy
100
30y M presents to clinic for knee pain that has progressed during his marathon training. Worse with sitting, squatting, and stairs. XR negative. Most likely Diagnosis:

Patellofemoral Pain Syndrome
100
A 38 yo F with PMH of anxiety and depression presents to clinic with 3 months of intermittent palpitations, increased appetite, "hot flashes", and 10 pound weight loss. She has a family history of lupus and RA. Physical exam is notable for mild bilateral tremors in upper extremities and a palpable nodule in the L lobe of the thyroid. TSH is 0.019 and Free T4 is elevated. What is the most appropriate next step in diagnosis?
A) Radioactive iodine scan
B) Thyroid US
C) TSH receptor antibody
D) Fine needle aspiration/biopsy
E) Refer to endocrinology
Radioactive iodine scan
100
63y F presents to clinic for a routine office visit. She takes a multi-vitamin and has no other medical problems. She asks when and how she should be checked for osteoporosis:
65y Female, DEXA
100
A 58 yo F presents with several noduloulcerative lesions on her forearm that first appeared about 1 month ago starting on the dorsal surface of her R hand. She thinks they appeared after she was doing some yard work in the bushes around her house.
What is the most likely causative organism?
Sporothrix schenkii
200
67y M admitted for pneumonia develops chest pain and dyspnea on the floor.
HR 139 BP 142/89 O2 93% RA
EKG reveals _____. What is your next step?
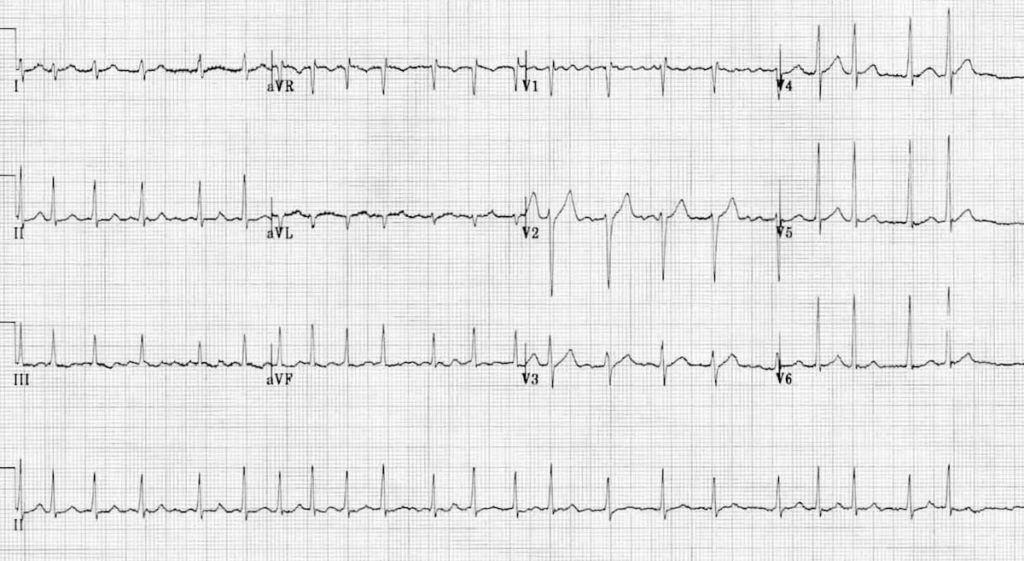
Atrial Fibrillation with RVR
IV Metoprolol
IV Diltiazem
200
14y F presents to clinic due to knee pain. She has swelling over the tibial tuberosity. Her pain worsens during evening track practice, but improves by 8am the next day. XR obtained below. Patient's mother asks about return to sports:

Continue sports as long as pain resolves within 24 hours
Conservative management, ICE, NSAIDs, PT
200
68y F has a DEXA T-score of −2.8 at the femoral neck. She has no history of fracture. What is the diagnosis, and what is first-line pharmacologic treatment?
Osteoporosis
Bisphosphonates are first line treatment. Counsel patients to take on empty stomach, full glass of water, and remain upright for 30min.
200
A 39 year old previous healthy male presents to clinic to establish care. He reports that his father was diagnosed with stage 3 colon cancer at age 52 and wants to know at what age he needs to start screening.
40 years
Per AAFP guidelines, screening in patient's with first degree relatives who were diagnosed with advanced colon cancer before 60 should start screening at 40 or at 10 years before age of diagnosis, whichever is EARLIER.
200
A 68 yo M with T2DM and peripheral neuropathy presents to clinic for discoloration and thickening of his toenails. Over the counter topical agents have had no effect. He has noticed that the nails are now brittle and easily lift off the nail bed. What is the next best step for management?

Oral terbinafine daily for 12 weeks
(If not fully treated, pause treatment for 12 weeks then resume daily for 4 weeks)
300
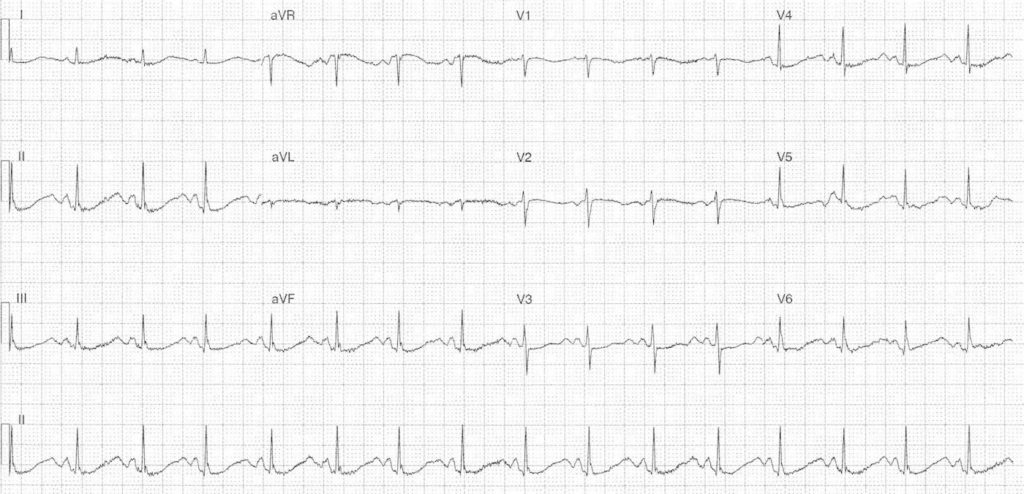
47y F presents with acute onset chest pain and dyspnea. HR 104, BP 152/92, O2 89% RA.
This diagnosis should remain high on your DDx based on presentation and EKG findings followed by the next best step.
PE, CTA Chest
S1Q3T3 (12-25% of cases)
Sinus Tachycardia (44-73% of cases)
RBBB (18-25% of cases)
300
32y F presents with bilateral hand pain and morning stiffness. Exam shows swellng of MCP and PIP joints with no involvement of DIP. RF is positive. This additional antibody would aid in conclusive diagnosis:

Anti-CCP (Cyclic Citrullinated Peptide) antibodies
300
25y F presents due to concern for irregular menses. On exam, she has evidence of acne and hirsutism. Labs show elevated free testosterone and a normal TSH and prolactin. She does not desire to be pregnant. What is the diagnosis and first line pharmacologic treatment?
PCOS. OCPs
Rotterdam Criteria requires 2/3: Oligovulation, Hyperandrogenism, Polycystic Ovaries on US
300
A 21 yo F completes her first pap smear for cervical cancer screening. Results show low-grade squamous intraepithelial lesion. What is the appropriate next step?
Repeat pap smear in 1 year
LSIL is commonly seen in active HPV. In patients less than 25, repeat testing without colposcopy is considered appropriate as most patients will spontaneously clear HPV.
300
77y M presents due to concern for skin lesion. Diagnosis?

Basal Cell Carcinoma
400
51y F with vomiting and diarrhea presents with weakness and fatigue. This electrolyte abnormality will precipitate the following EKG changes.
Hypokalemia +/- Hypomagnesemia
ST segment depression, ↓ amplitude T wave, ↑ amplitude U waves at the end of the T wave, prolonged QT
400
13-year-old obese boy presents with a limp and left groin pain. He holds the left leg in external rotation. Internal rotation of the hip is limited and painful. Diagnosis?

Slipped capital femoral epiphysis (SCFE)
Risks: Obese, premenarche (F), tanner III (M)
Can have hip, groin, thigh, knee pain
400
62y F presents to ED with N/V, AMS, and polyuria for 3 days. PMH osteoporosis and HTN treated with HCTZ. She has been having worsening heartburn and taking OTC calcium carbonate. Labs reveal:
Serum calcium: 14.8 mg/dL (normal 8.5–10.5)
Creatinine: 2.4 mg/dL (baseline 0.9)
BUN: 38 mg/dL
Bicarbonate: 34 mEq/L (normal 22–28)
Phosphorus: 3.2 mg/dL
PTH: 8 pg/mL (normal 15–65)
PTHrP: negative
25-OH vitamin D: normal
What is the most likely diagnosis?
A) Primary hyperparathyroidism
B) Hypercalcemia of malignancy
C) Milk-alkali syndrome
D) Sarcoidosis
E) Familial hypocalciuric hypercalcemia
C) Milk Alkali Syndrome
hypercalcemia, metabolic alkalosis, and renal insufficiency resulting from excessive ingestion of calcium and absorbable alkali
**Low PTH, negative PTHrP, normal Vit D
400
68y M presents to discuss his AAA screening US. It was discovered that he has a 4.2cm AAA. He denies abdominal pain. When should have have repeat imaging?
Repeat US AAA in 1 year, each year until growth >5.5cm then refer
Encourage smoking cessation, control BP and lipids, encourage exercise
400
55y F presents to the clinic for ear pain that started 2 days ago. She has associated hearing loss. On exam, there are grouped vesicles with erythema noted in her left external canal. Diagnosis?
VZV, Ramsay Hunt Syndrome
Tx: Valtrex 1g TID 7 days, Prednisone 1mg/kg 5 days
500
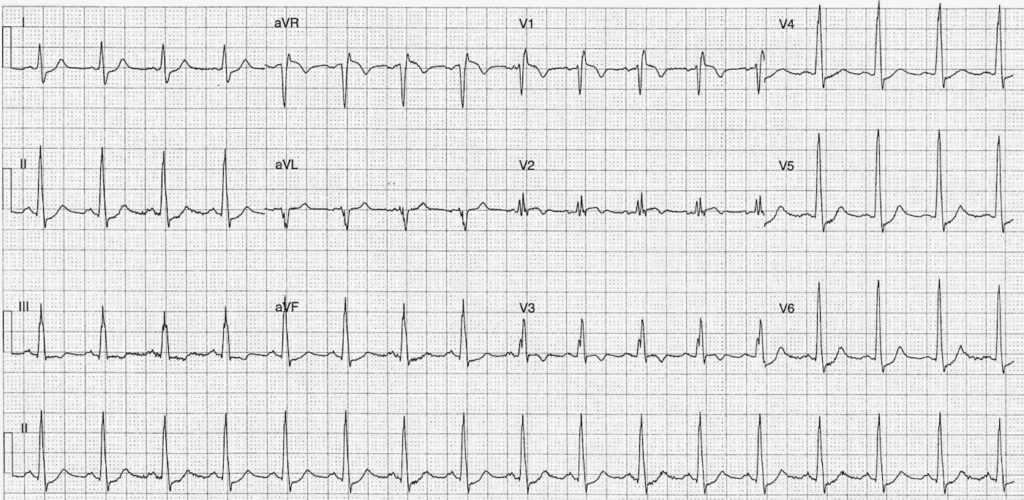
55y M with DM2, HTN, HLD, and 20y smoking history presents for intermittent chest pain. EKG reveals:
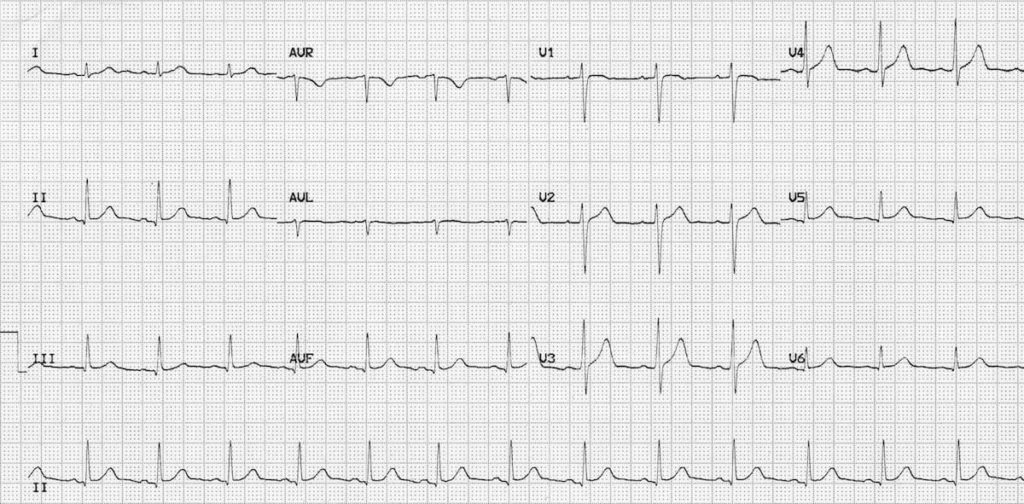
Normal Sinus Rhythm
Next steps: CAC vs Stress Test
500
55y F presents to clinic for right shoulder pain. On exam, she cannot actively abduct her arm past 60° but has full passive ROM. She has weakness during strength testing with her shoulder flexed at 90 degrees and shoulder internal rotation. On MRI, which tendon is most likely to be torn?
Supraspinatus Tendon
Empty can test. Pain with testing is likely tendinopathy, weakness with testing is likely tendon tear
500
A 58-year-old African American man with a 12-year history of type 2 diabetes, hypertension, and obesity (BMI 34) presents for routine follow-up. His current medications are metformin 1000 mg BID, glimepiride 4 mg daily, and lisinopril 20 mg daily. Labs reveal:
HbA1c: 8.4%
Fasting glucose: 198 mg/dL
Creatinine: 1.8 mg/dL, eGFR: 38 mL/min/1.73 m²
Potassium: 4.9 mEq/L
Vitamin B12: 180 pg/mL (low-normal; reference 200–900)
In addition to adding Vit B12, Which medications adjustments should be made?
A) Continue current, add Farxiga 10mg
B) Reduce Metformin 500mg BID, add Farxiga 10mg
C) Continue current, add Sitagliptin 25mg
D) Reduce Metformin 500mg BID, increase glimepiride 8mg
B) Reduce Metformin 500mg BID, add Farxiga 10mg
eGFR 30-45: Metformin 500 BID
CKD3b: SGLT2, may be continued for CKD even if eGFR <25 though glycemic benefit declines eGFR <45
500
18y F presents to clinic for a routine visit. She has never received the HPV vaccine but is interested in reducing her risk of cervical cancer. How many doses of HPV vaccine will she need?
3 dose series over 6 months
If given before age of 15, only requires 2 dose series. May be given as early as 9y and up to 26y
500
A 40 yo F with T2DM and obesity presents with painful, indurated nodules and scarring in both axillae. Some of these nodules appear to be draining scant, foul-smelling fluid.
What other disorders can be associated with this condition?
A) Psoriasis
B) Dermatitis herpetiformis
C) Crohn's Disease
D) Nummular eczema
E) PCOS
C) Crohn's Disease