Instagram-able
Sickle Me This (and then some)
Anemias
Intravascular or Extravascular
Everything everywhere all at once
Hypercellular
100
26yoF who was in her usual state of health up until 1 week ago comes in with a terrible headache and somnolence for the last 2 days. She is hemodynamically stable and has normal renal function. On CBC she has a Hb of 9.2g/dL and a platelet count of 45,000/uL. The rest of her labs have not resulted yet. You see this on peripheral smear. You are concerned she may have this.
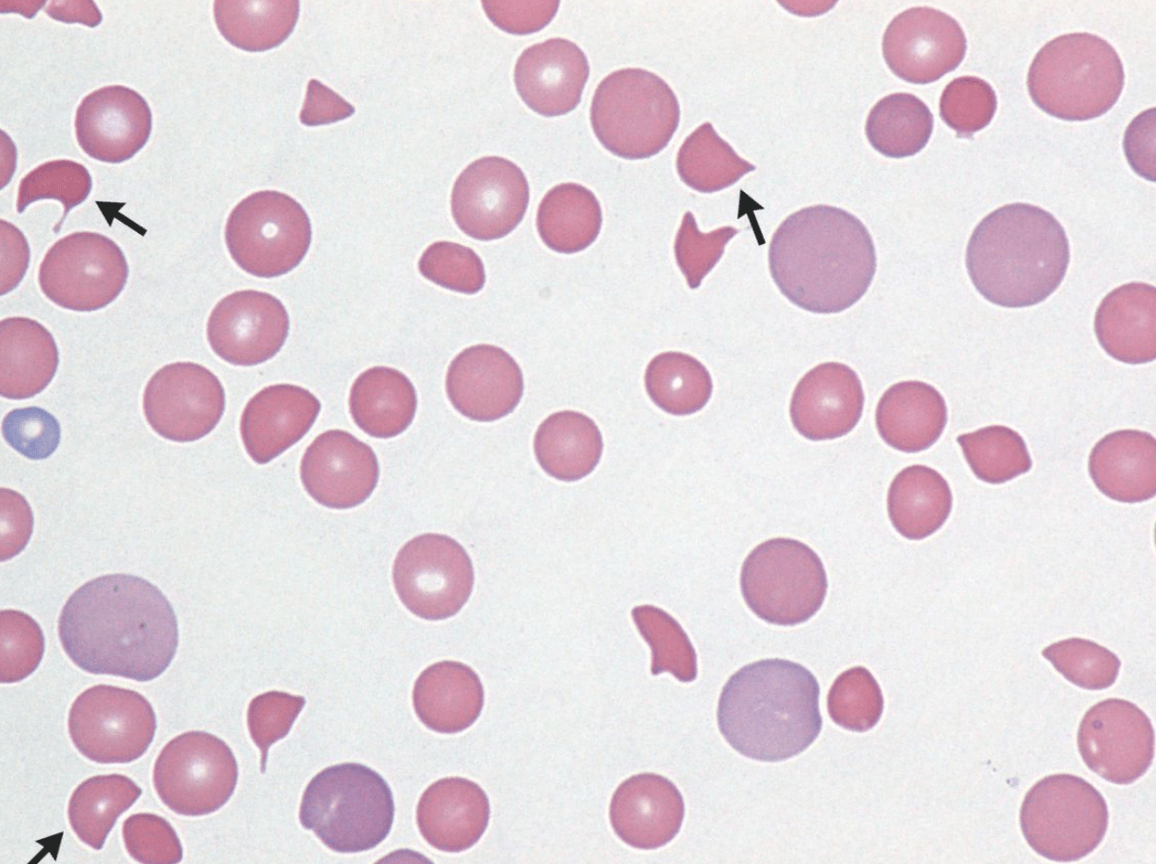
What is TTP.
Since PT and PTT are not given, DIC is also on the differential.
100
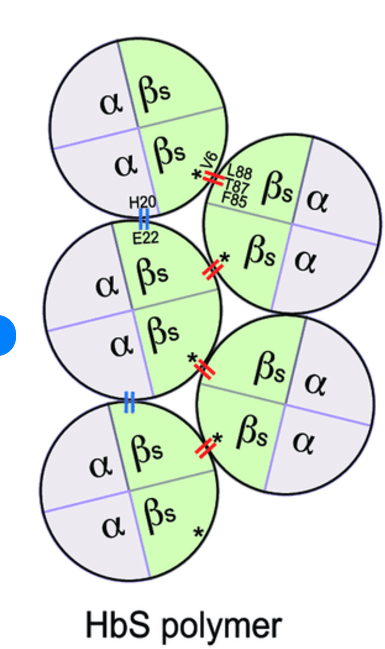
Hb S is made up of these globin chains
2 alpha chains and 2 beta chains with a mutation in the beta chain that results in glutamine changing to valine.
100
You think of this diagnosis as you see a 23 year old female who comes to see you for fatigue. Her periods are frequent, heavy and irregular. She tells you this as she shakes her big-gulp sized cup full of ice chips that she intermittently crunches on.
What is iron deficiency?
What would you expect her Iron studies to look like?
100
What immunoglobulin is involved in warm autoimmune hemolytic anemia?
IgG
100
The other day you were playing trust with a friend. As you closed your eyes and got ready to fall, you noticed yourself start to sway and almost lose balance before purposely falling into their arms. As a discerning medical student who just completed hematology you decide to tell your doctor to check which vitamin?
What is a B12 level
(+ romberg sign)
Romberg's test, Romberg's sign, or the Romberg maneuver is a test used in an exam of neurological function for balance. The exam is based on the premise that a person requires at least two of the three following senses to maintain balance while standing: proprioception; vestibular function; and vision. Diseases affecting the dorsal columns of the spinal cord will show a positive sign.
100
A 36 year old man is in a motor vehicle accident and undergoes surgery for a femur fracture. Post operatively, 1 day after the accident, his WBC is 25k/uL (4.8-10.8), his Hb is 11/dL ( nl 13-15) and his plt is 524k/uL. Labs 4 months ago show a WBC of 8.3k/uL, Hb of 15.2 and a platelet count of 263k/uL. % neutrophils=90. 6%lymphs, 3% monos. 2% eos. 1% basos.
Peripheral smear is shown:
What do you think is going on?
Inflammatory. Reactive neutrophilia.
200
These broken down or smudged cells are often seen on the peripheral smear of which mature lymphoid malignancy?
What is CLL?
200
Hydroxyurea increases this type of Hb in patients with sickle cell disease
Bonus: how else does Hydroxyurea work?
What is Hb F
200
40 yo M not taking any medications comes to doctors office because he has been feeling fatigued lately. Cbc shows a Hb of 6g/dL (12-15), WBC of 1.2x109/L (nl 4.5-10.5) and neutrophil count of 0.2x109/L, platelets of 11,000/uL (nl150-400). HE is sent emergently to the hospital. All viral studies and other infectious work up is negative. B12 and folic acid are normal. CT scan shows no Lymphadenopathy. Bone marrow biopsy shows a hypocellular marrow with increased fat. No blasts or malignant cells are found. What is the diagnosis?
What is Aplastic Anemia

200
A 65 year old man with a history of Hypertension develops chest pain and shortness of breath that has started and worsened over the last 24 hours and presents to the ED. Work up for acute coronary syndrome is underway when his CBC comes back and his Hb is 4.5g/dL, Plt is 179,000/uL and WBC is 5.4x109/L. and absolute reticulocyte count is 125,000 (H). Liver tests result soon after and show a total bili of 5.5 and a direct of 1.4. In order to confirm (or refute) your suspicion that he may have an autoimmune hemolytic anemia, you decide to send this test.
What is the coombs test?
200
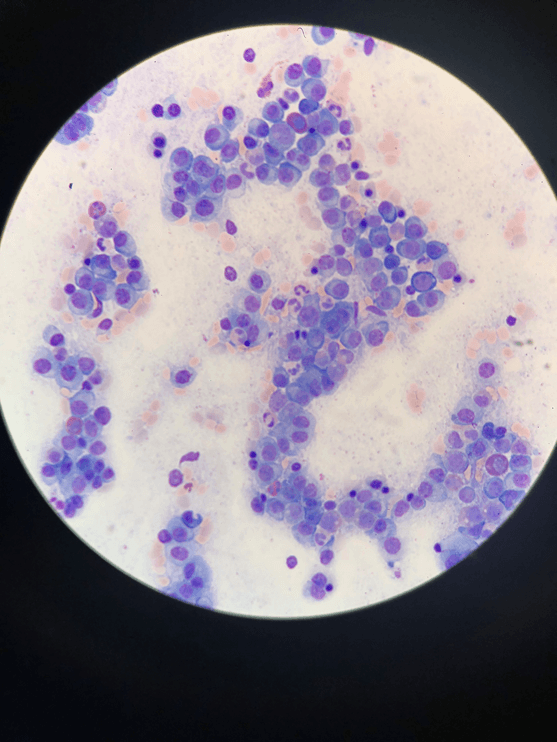
A 22-year-old female presented with 2 weeks of fever, anemia, generalized lymphadenopathy, hepatosplenomegaly, and skin rashes. Her total leukocyte count was 306 × 109/L. Peripheral blood smear showed many atypical lymphocytes with petal-shaped nuclei as seen in the photograph. Peripheral blood immunophenotype noted negative markers for myeloid and B lymphoid lineage (CD10, CD19, CD3, CD5, CD7, cyto-CD3, TCR, CD16, CD56) and strongly positive for CD4 and CD25, and also CD2, which was atypical. Bone marrow aspirate and biopsy revealed involvement by acute leukemia. Serology for HTLV-1 was positive and serum calcium was normal.
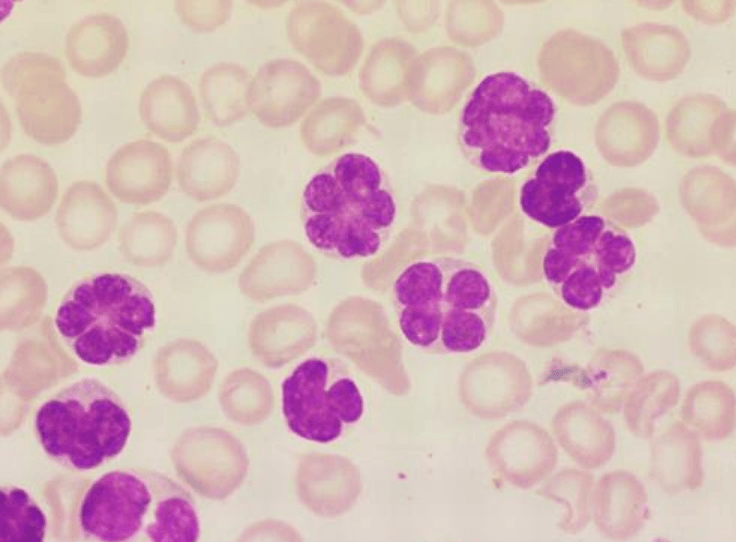
What is Adult T cell Leukemia Lymphoma
200
A 36 year old man comes to the office for yearly check up with his PCP. Upon further questioning he does report that lately he feels hungry, wants to eat, but when he feels like he can't eat more than half of his meals.
Lab work up shows Hb of 15, Wbc of 95k/uL Plt of 513k/L. WBC shows 47% polys, 27% bands, 5% metamyelocytes, 8% myelocytes, 3% blasts. 5% lymps, 3% basos, 2% monos 1%eos.
Smear shows:
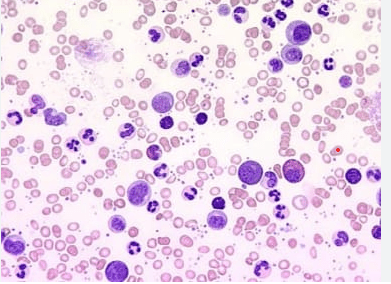
After confirming the diagnosis, what medication (can give class of medication) will you start?
Tyrosine Kinase Inhibitor
Imatinib,
Dasatinib
Nilotinib
300
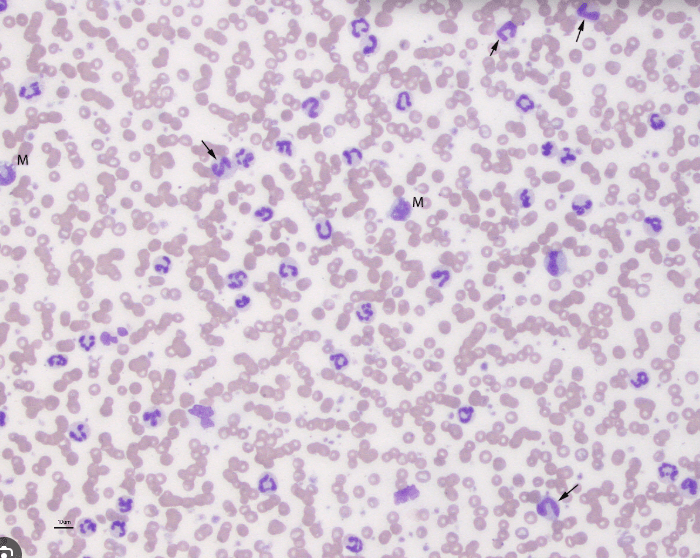
When you saw this finding on PS in a patient on the wards, you checked and found an ESR of 120!
Bonus: name 3 diseases that can give this smear findings.
What is rouleaux formation?
RBCs typically repel eachother becaues they are negatively charged. WHen there is an increase in positively charged proteins, such as immunoglobulins and fibrinogen, we can see a rouleaux and also an elevated ESR.
The stacking of cells (rouleaux formation) facilitates the rate of red cell sedimentation, a phenomenon that may be seen on a peripheral smear.
Seen in Significant paraproteinemias, chronic infections, chronic liver disease, connective tissue diseases.
300
A 23 year old male with HbSS disease comes to the hospital with shortness of breath and chest pain. He has a temperature of 102F. O2 sat is 82% on Room air. With O2 he is at 88%. He looks uncomfortable when breathing. Chest Xray shows bilateral infiltrates at the bases. His Hb is 8g/dL (normal 12-15), his usual baseline is 9g/dL. The MICU is called and they are considering intubation given his respiratory distress. In addition to antibiotics and respiratory management, what is the best management for this patient with sickle cell disease?
He has acute chest syndrome. Best management is exchange transfusion.
300
Anemia of chronic disease is mediated by an increase in this enzyme which blocks the release of iron from macrophages as well as the absorption of iron from the gut.
What is hepcidin.
AOCD is seen in Chronic infections neoplastic disorders, SLE, RA, ckd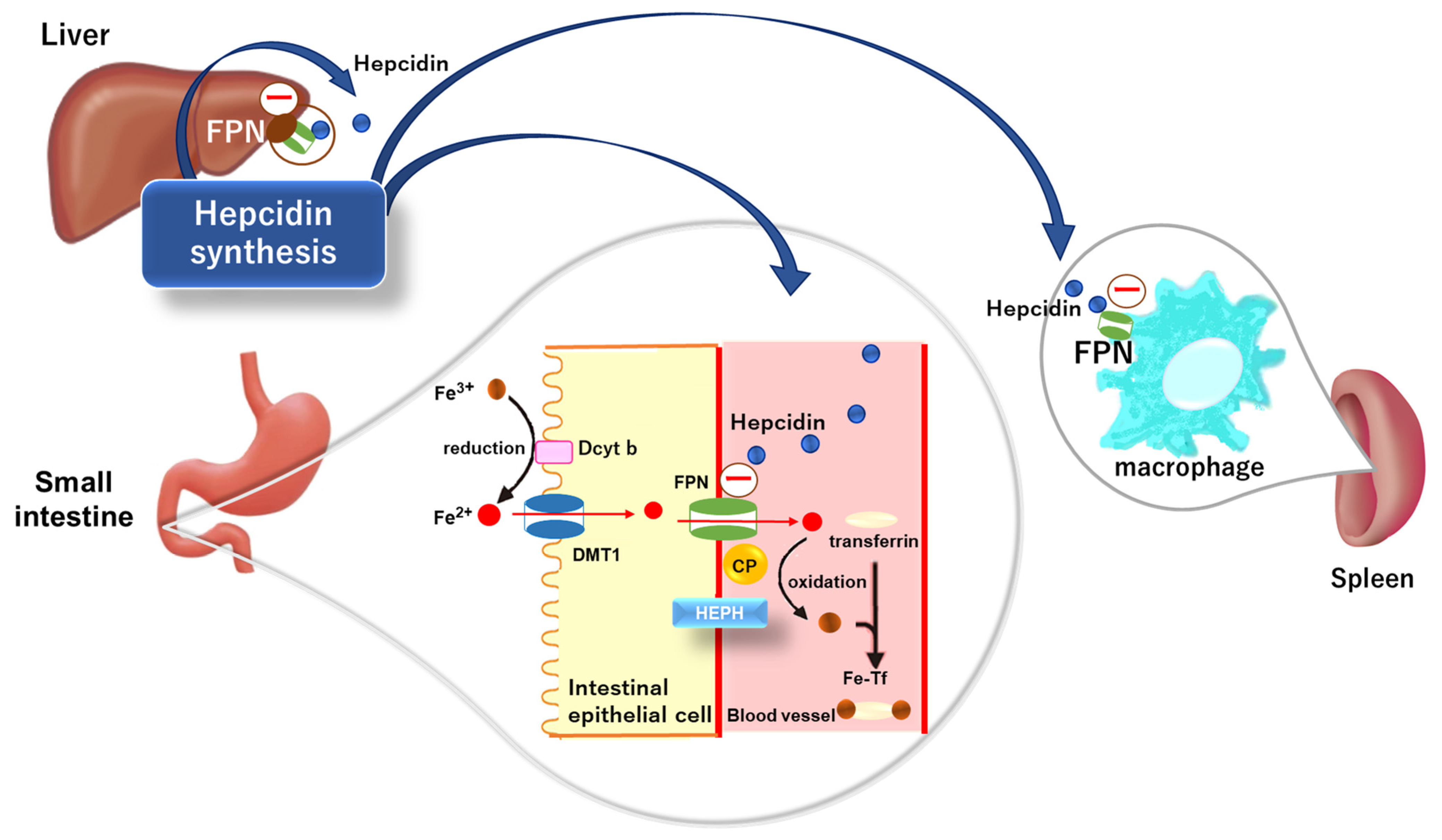
300
Cold Autoimmune Hemolytic anemia can be triggered by an infection from this type of bacteria.
What is mycoplasma pneumoniae
(EBV and CMV can also do it)
Cold Autoimmune Hemolytic Anemia : typically mediated by IgM and Complement which cause agglutination and extravascular hemolysis upon exposure to cold. Can see acrocyanosis: painful / blue fingers and toes.

300
You are seeing a 24 year old female for a history of thrombocytopenia. She states she has had mild thrombocytopenia her entire life. Her current platelet count is 70,000/uL. She reports she has easy bruising. You send for testing: Ristocetin induced platelet aggregation is decreased. Smear is below. What does she have?

What is Bernard-Soulier Syndrome.
(AR inheritance)
Ristocetin-induced platelet aggregation (RIPA) is used as an in vitro test to determine the presence and integrity of the platelet glycoprotein (GP) Ibα-V-IX complex and von Willebrand factor (VWF) interaction
300
A 62 year old man presents to his PCP with progressive fatigue and early satiety over the past 4 months. Physical exam reveals splenomegaly with the spleen palpable 6cm below the L costal margin. Laboratory studies show Hb 9.5g/dL, white blood cell count 13.2k/uL and platelet count 110k/uL
Choose the smear:
A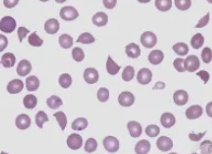
B

C 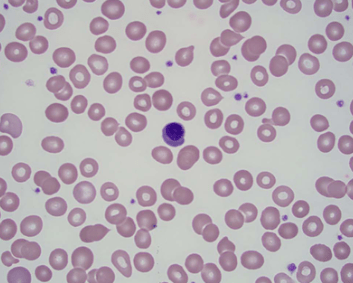
D 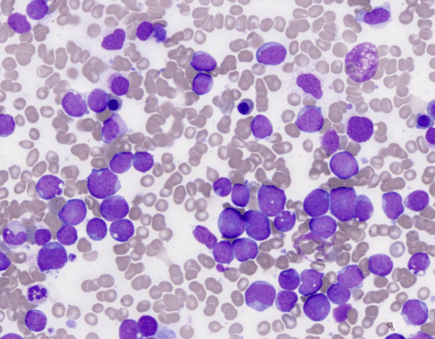
C
400
What organ is this patient missing?

Spleen
Howell Jolly Bodies
400
A 29 year old female comes to you on ferrous sulfate. She reports her primary doctor has been giving her iron to help her Hb of 9g/dL but it never seems to increase. Ferritin is 150ng/ml. Serum iron is 35ug/dl. TIBC is 290ug/dl. MCV is 66fl. She reports very light periods. Hemoglobin electrophoresis shows a low HbA2 of 1%(HbA2 2.6-3.4%). What do you conclude she has.
She likely has alpha thalassemia mutation.
What if the HbA2 were 4.5%?
HbA2 – 2.6-3.4%
400
A 25 year old man in the hospital has just been diagnosed with an aggressive T cell lymphoma with diffuse lymphadenopathy above and below the diaphragm. He is ill appearing. His Hb is 9g/dL His LDH is 2500(H), His Uric Acid is 10, His Creatinine is 2.3 (baseline 1.1), Calcium is 7.8(L), and his K is 5.3 (high normal). Given concern for tumor lysis, the team treats with aggressive hydration and rasburicase and hours later the patient gets acutely short of breath, Hb drops to 5.1g/dL and haptoglobin (was 150) is now undetectable with bite and blister cells on the peripheral smear. You tell your team this is what caused the acute drop in Hb.
What is G6PD deficiency
Blister cells.
This patient is autolysing.
is X linked recessive.
Still have to worry about it in women, but much more often severe in men.
Need test for g6pd deficiency before giving these agents.
400
42 year old female comes to the hospital reporting tea colored urine after waking up this morning and is found to be anemic. Coombs testing is negative but she has an elevated indirect bilirubin, high lactic dehydrogenase and a low haptoglobin. She also has mild pancytopenia, and is found to have a LLE deep venous thrombosis. Flow cytometry shows CD55 and CD59 negative Red blood cells. What medication will you treat her with?
Complement inhibition.
Eculizumab or Ravalizumab
400
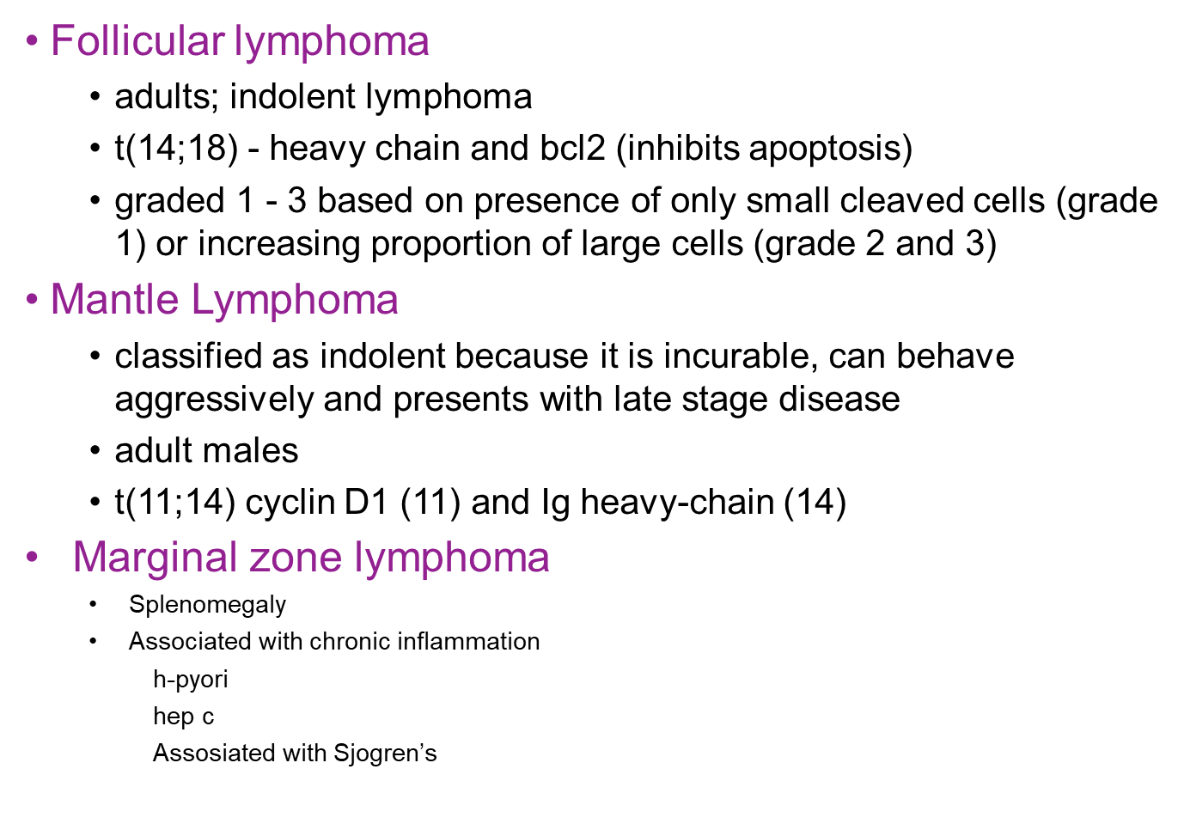
Treatment of H. pylori could result in the eradication of which early stage lymphoma?
Extranodal Marginal Zone Lymphoma in the stomach
MALT lymphoma.
400
A 65 year old 20 pack year smoker man comes to see you for a high Hct. His hb is 18g/dL and his Hct is 54. He recently had a stroke and was discharged from the hospital for follow up with you. In the hospital his Epo was undetectable, he had iron deficiency and he had a +Jak2V617F mutation. What will you do to manage his condition?
Phlebotomy to a Hct less than 45.
500
Sometimes you'll see me in hemolytic anemia or in bone marrow pathology? What am I? 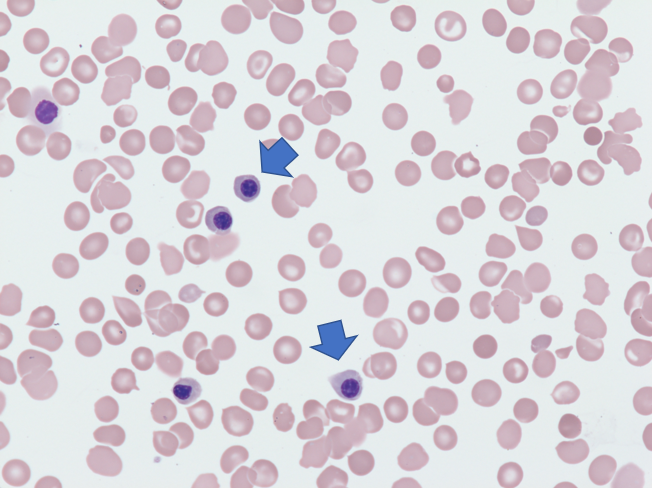
What is a nucleated Red Blood Cell.
(I am Not a plasma cell, see here for comparison both pictures below are plasma cells)
500
A 32 year old female with Sickle Cell disease comes in with acute aplastic crisis. Her Reticulocyte count is very low, along her her Hb which is 4g/dl, lower than her usual of 7.5g/dL (normal 12.5-15). What is the most common culprit causing aplastic crisis?
Parvovirus B19
Management: supportive care. Will slowly recover over 1-2 weeks.
What is the reticulocyte count a measure of?
aplastic crisis different from aplastic anemia.
500
What is the name of these cells? Name 2 diseases they are seen in?
What are ringed sideroblasts.
Accumulation of iron in mitochondria preventing it from being incorporated into Heme.
seen in MDS
or lead poisioning or a congenital sideroblastic anemia.
500
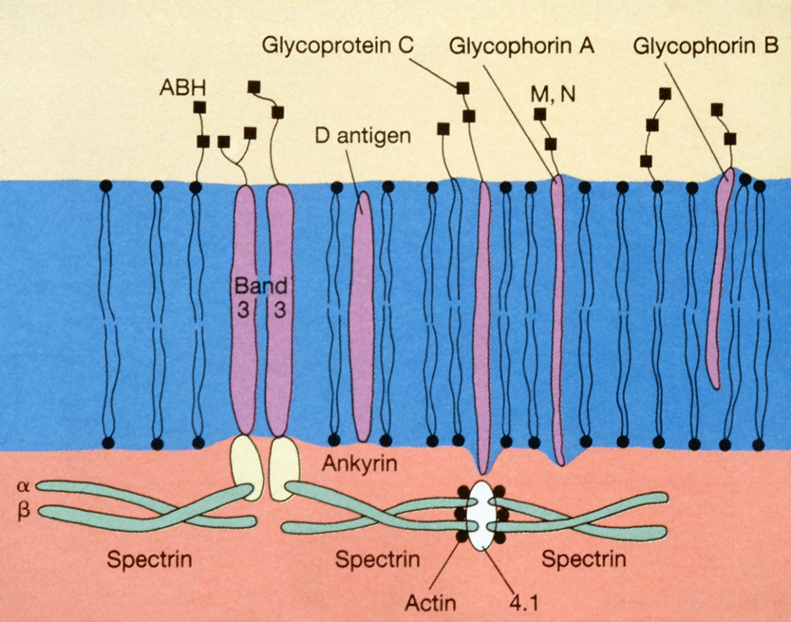
A 46 year old man has a longstanding anemia. He has a history of HTN, surgically had a cholecystectomy in the past. He has a Hb of 9g/dL. Haptoglobin is <10. Total bilirubin is 2.9mg/dl and direct bilirubin is 0.8mg/dl. Looking back he has always had mild anemia and a low haptoglobin. Testing demonstrates increased osmotic fragility.
Name 2 of the proteins that can be mutated or deficient in this disease.
Hereditary spherocytosis.
-deficiency of ankryn – up to 50% of cases
-deficiency of spectrin alpha or beta
-4.2 deficiency
-point mutations of Band 3
500
A 57 year old female presents to the ED with a history of hypothyroidism, reporting that she has had some easy bruising last few weeks but today when she was walking in the house with grocery bags, she noticed significant confluent progressive bruising of both her arms. She has never had a bleeding issue in the past. Labs show a new anemia, Hb is 9g/dl. PLatelet count is normal. PT is 10s, PTT is 55s. Mixing study does not correct. Factor VIII is undetectable. What is your diagnosis?
Bonus: HOw will you manage this?
FActor VIII inhibitor.
500
A 65 year old man nonsmokder with a history of hypertension comes to see you for a high Hct. His hb is 18g/dL and his Hct is 54%. He recently had a stroke and was discharged from the hospital for follow up with you. In the hospital his Epo 300 (normal 5-20) and his Jak2 v617F mutation was negative. What will you do to work him up further?
Bonus: what are other 2 other common clinical scenarious to cause secondary erythrocytosis?
Epo secreting Tumor
High altitude
Obstructive Sleep Apnea
Smoking
Testosterone
600
A 56 year old man comes in to see you for headaches. He also reports he is more short of breath on exertion than he used to be. He also admits to some blurry vision on occasion, this is new over the last few weeks. On exam he has Lymphadenopathy in the neck and axilla. Labs show Hb of 9g/dL, platelets of 90K/uL, WBC of 7k/uL. Chemistry including Calcium and creatinine is normal, except his total protein is 10g/dL. Albumin is 3.3. Serum protein shows 5.7g/dL of IgMkappa. He denies any pain anywhere.
What is your first step in management of this patient?
Waldenstroms presentation.
Admit, Plasmapharesis
600
A 45 yoM is diagnosed with stage IV Diffuse large B cell lymphoma. You treat him with standard of care with curative intent and give him Rituixmab, Cytoxan, Vincristine, Doxorubicin and prednisone. (RCHOP). Interim PET CT shows improvement of disease. Post treatment pet shows NED, but 2 months later he comes back to see you with worsening lymphadenopathy, fevers chills and sweats. What treatment are you going to recommend now?
CART therapy
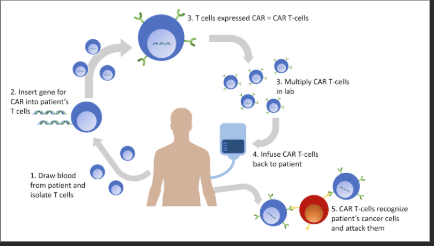
CART is recommended as a second line in refractory disease or in early relapse -within 12 months. If not within 12 months then advised after 2 lines of systemic therapy.