Oh Baby!
Oh Baby! Part 2
We're all crusty here
100
2 day old neonate with the following rash. Born at 39 weeks via cesarean delivery. Mom received routine prenatal care. Infant is BF well, had 3 wet diapers and 1 meconium stool. 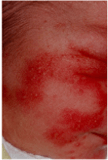
Erythema Toxicum Neonatorum
- 20% of neonates in first 3 days of life
- unknown etiology. self resolving within 5 days
- erythematous macules and papules tha rapidly progress to pustules on erythematous base
100
16 day old brought to your office for rash on eyebrows:

What is the rash and treatment?
Seborrheic Dermatitis
- self limiting erythematous plaques with greasy, yellowish scales
- areas rich in sebaceous glands (scalp, ear, center of face, intertriginous areas)
- Resolves within weeks to months of birth.
- Tx: emollients, shampoo and brush, ketoconazole shampoo, topical steroids x 1 week.
100
45 yo diabetic presents with complaints of chronic red rash, non-pruritic on medial thighs. This has been ongoing for years.

Erythrasma
- chronic superficial infection of intertriginous areas
- Reddish brown, scaly, flat macules. Can be pruritic but not always.
- Caused by Corynebacterium minutissimum
- RFs: T2DM, obesity, warm weather, excessive sweating
- coral red flourescence shows Gram + filamentous rods
- Tx with washing, erythromycin gel or oral azithromycin
200
5 day old male who lives in Florida with parents presents with this rash: 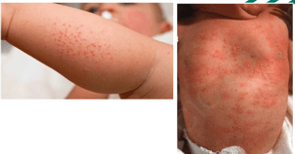
Miliaria aka Heat Rash
- common in newborns in warm climate.
- accumulation of sweat beneath sweat ducts that are obstructed by keratin
- usually first week of life. Resolves when moved to cooler conditions
200
3 day old infant with white bumps in the mouth:

Milia (Epstein's pearls)
- milia is very common and affects >50% of newborns
- usually on nose and cheeks but can be in the mouth (Epstein's pearls)
- No tx needed.
200
33 yo male present c/o several red lesions on his palms, hands, and lips. Has a history of recurrent herpes.

Erythema Multiforme
- active, self limiting and sometimes recurring
- Type IV hypersensitivity reaction. Triggered by infection, meds, various triggers (HSV!)
- Major: involves membranes with systemic signs.
- Minor: Rash only, little to no systemic signs.
- Supportive treatment.
300
Female neonate is born via vaginal delivery at 41 weeks to 26 yo female. uncomplicated pregnancy and delivery. Exam 2 hours after delivery shows the following lesions. No other abnormalities noted. During exam, infant starts to suck vigorously at the involved areas.

congenital sucking blister
careful not to confuse with more serious infection such as herpes, candidiasis, SLE, bullous impetigo. These should be accompanied by other clinical symptoms/signs.
300
6 month old presents with birthmark which is growing with no signs of regression. What is the official name and treatment?

Nevus Flammeus
- congenital low flow vascular malformation in dermal capillaries
- blanchable, usually unilateral, painless, flat
- If periorbital involvement must eval for glaucoma
- can treat with pulsed dye laser for cosmetic purposes
300
60 yo female with T2DM presents with tender facial rash accompanied by fevers, lymphadenopathy. She recently had a sore throat:

Erysipelas
- infection of upper dermis and superficial lymphatics causeed by beta hemolytic streptococcus
- more superficial, raised and demarcated than cellulitis.
- Fiery red, high fevers, indurated, tense, shiny plaque.
- Treatment targeted for strep bacteria!
400
3 week old newborn presents with this rash which consists of inflammatory papules and pustules limited to the face

Neonatal Cephalic Pustulosis
- occurs in up to 20% of infants
- Used to be called "neonatal acne" but that term is not accurate as this is not caused by stimulation of the sebaceous glands
- Usually onsets around 3 weeks. Tx with cleansing soap/water and avoidance of oils and lotions.
- Can use ketoconazole BID or 1% hydrocortisone until clearance.
- not associated with acne later in life.
400
Mom brings her 2 week old for a well check on Jan 15th. Pediatrician notes the follow rash at start of visit, but notes this rash is gone by the end of the visit:

Cutis Marmorata
- vascular disorder affecting newborns
- when exposed to cold. resolves when warmed.
- normal physiologic response for babies!
- No treatment needed. often associated with Downs.
400
20 yo student presents to clinic c/o scaly rash on his trunk. he had mild fever and HA a few weeks prior but states this was minor and self resolving. His rash doesn't itch. He plays tennis and spends time outdoors. Lesions are primarily on his trunk. Sun exposed areas on his arms do not have any lesions.

Pityriasis Rosea
- common, self limiting papulosquamous eruption seen in children and young adults usually following viral URI.
- prodromal URI. No pruritis.
- Herald patch with eruption usually 1-2 weeks in a "christmas tree" pattern.
- rose colored or violet
- cluster in lower abdomen and pubic areas.
- Tx with observation. Resolves within 4-12 weeks.
500
3 day old presents for WCC. Mom is concerned about a pink colored rash on his face. The rash blanches when pressed and is darker when he is upset:

Nevus Simplex (Salmon Patch, stork bite)
- 40-60% of infants
- eyelids, glabella, midline of nape of neck.
- vascular birthmark caused by telangiectasias in dermis layer of skin
- Fades within 1-2 years.
500
Mom brings her newborn in for 2 week well check on Jan 15th. The following rash is noted by the pediatrician throughout the exam and visit:

Cutis Marmorata telangiectasia congenita
- serious, rare condition that does NOT improve with warming.
- associated with several congenital abnormalities (craniofacial, skeletal, neurologic, vascular)
500
25 yo woman on OCPs comes to office with a rash on her hands, forearms, and face. On exam she has oozing ulcers and hyperpigmented skin. Her mom has similar issues.
Porphyria Cutanea Tarda
- familial disorder caused by heme synthetic enzyme uroporphyrinogen decarboxylase (UROD) deficiency which leads to overproduction of porphyrin byproducts.
- fragile skin, erythema, vesicles progressing to blisters, erosions and ulcers.
- Triggers: Sunlight, alcohol, estrogen, viral hepatitis, iron.