What's your phenotype?
paper trail
Troubleshooting
ECHO STAT
scenarios
100
MAP 58, CI 1.6, CVP 14, PCWP 28, SvO2 46%, Lactic 5.1
levo @ 20, dobutamine @ 5
what is your issue? (ex: LV, RV, BIV, etc)
LV failure
100
DanGer was this type of trial.
Randomized control trial
100
When suction alarms occur, these 3 things could be causing it.
poor positioning, inadequate volume, or right heart failure
100
What is the distance between the aortic valve annulus and the inlet of the impella catheter supposed to be for the impella CP?
3.5 cm
100
What is the ACT goal for the left sided devices in the ICU?
160-180
200
Impella CP at P-7, getting suction alarms.
MAP 64, CI 1.8, CVP 20, PAP 50/28, PCWP 12, SvO2 48%, Lactic 1.2
what is your issue? (ex: LV, RV, BIV, etc)
RV FAILURE
200
"In selected patients with STEMI and severe or refractory cardiogenic shock, insertion of a microaxial intravascular flow pump is reasonable to reduce death" Refers to this class.
class 2a
200
You have bright red urine, you suspect hemolysis, what things would you check/do related to the pump to troubleshoot?
-adequate preload
-appropriate afterload (MAP<80)
-positioning ( under pap muscle?, outlet too close to aortic valve?)
-turn down p-level if patient can tolerate
-escalate to bigger pump ( 5.5 )
200
What is the distance between the aortic valve annulus and the inlet of the impella catheter supposed to be for the impella 5.5?
5.0 cm
200
Impella CP is less likely to hemolyze than the impella 5.5 due to its larger motor size and less RPM needed to generate flow. true or false?
False
300
Impella CP @ P-8
MAP 55, CI 1.5, CVP 22, PAP 60/35, PCWP 25, SVR 1800, SvO2 42%, Lactic 6.2
Norepi @ 25, dobutamine @ 7.5, vaso @ 0.02
what is your issue? (ex: LV, RV, BIV, etc)
Biventricular failure
300
Routine use of Impella reduces ALL-CAUSE mortality at 180 days by this amount in patients in CGS due to AMI.
12.7%
300
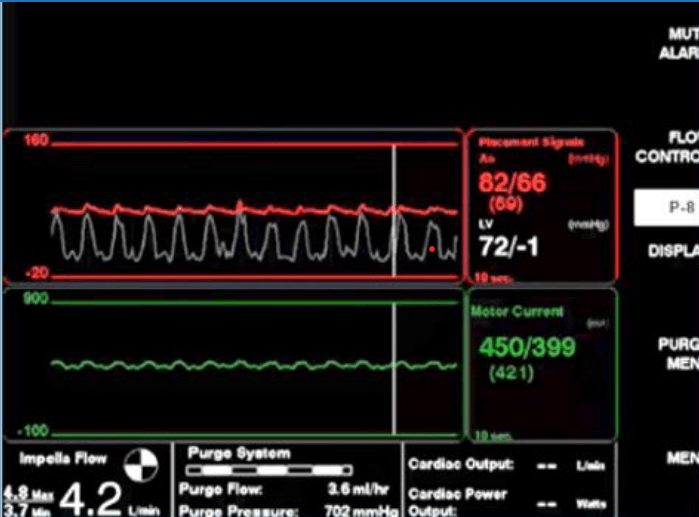
What do you think is the cause of this alarm?
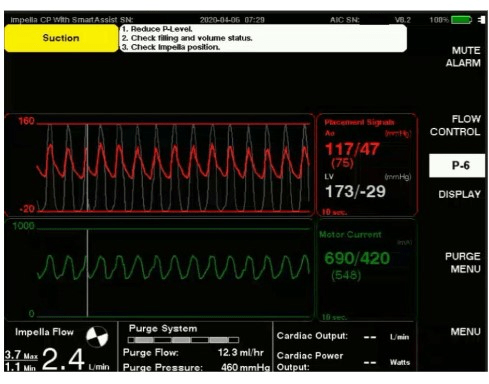
diastolic suction/volume related suction.
why?
negative diastolic LV number, lower than expected diastolic flows
treatment?
300
is this a properly positioned CP?
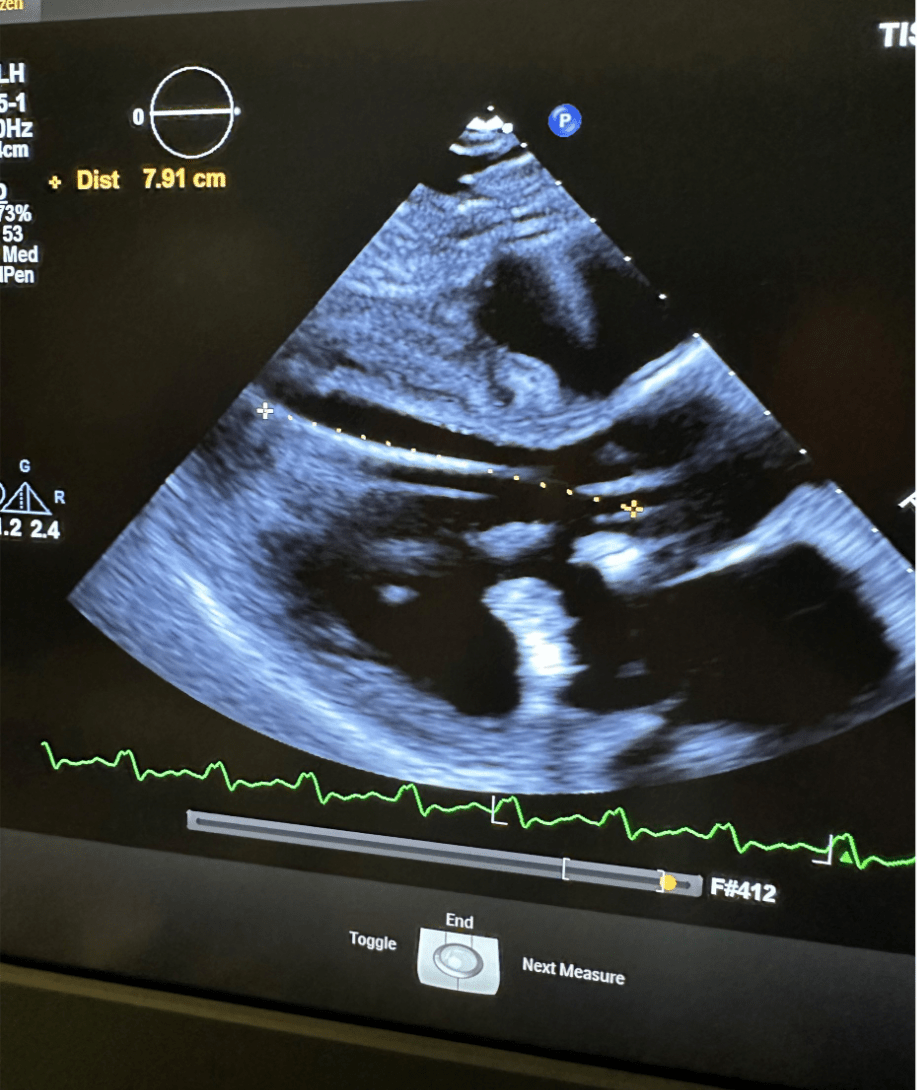
no. bonus:
what is wrong with it?
300
A patient will experience a 1% increase in their mortality for every _____ they spend in shock.
1 hour
400
impella CP @ P-7, MAP 60, CI 1.8, CVP 2, PCWP 4, PAP 22/8, SvO2 55%, Lactic 2.6
levophed gtt @ 8
what is your issue? (ex: LV, RV, BIV, etc)
hypovolemia
400
"In patients with cardiogenic shock, it is recommended to initiate tMCS before the onset of severe organ dysfunction" is what class in the EACTS/STS/AATS Guidelines?
Class 1
400
what is causing this suction alarm?
continuous suction. lower than expected flows in systole and diastole. completely decoupled LV and Placement signal.
Positioning.
400
Where would you measure this impella heart pump from? point to the screen
mid inlet to the aortic valve annulus
400
Does this patient appear to be supported?
yes.
No active alarms
MAP and flows appropriate
500
Impella CP @ P-9 3.6L
CO 3.6/CI 1.6, MAP 68, CVP 17, PAP 55/20, PCWP 25, Lactic normal, SvO2 48%, norepi @ 3, dobut @ 2.5
what is the issue? what should you do?
LV failure worsening, escalate and watch RV
500
True or False: "In patients with post-procedural LCOS, tMCS is recommended" this is a class 3 recommendation from the EACTS/STS/AATS Guidelines in LCOS
False.
What class is it?
500
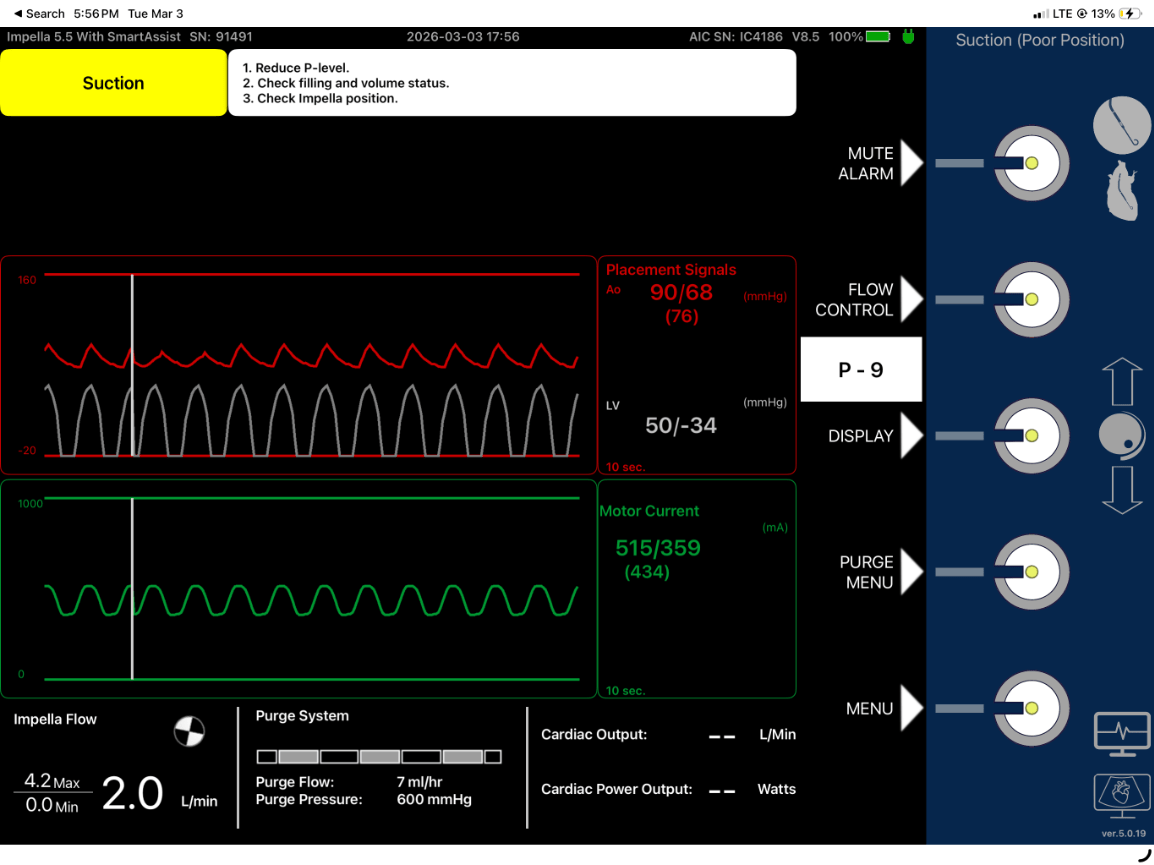
What is the cause of this alarm?
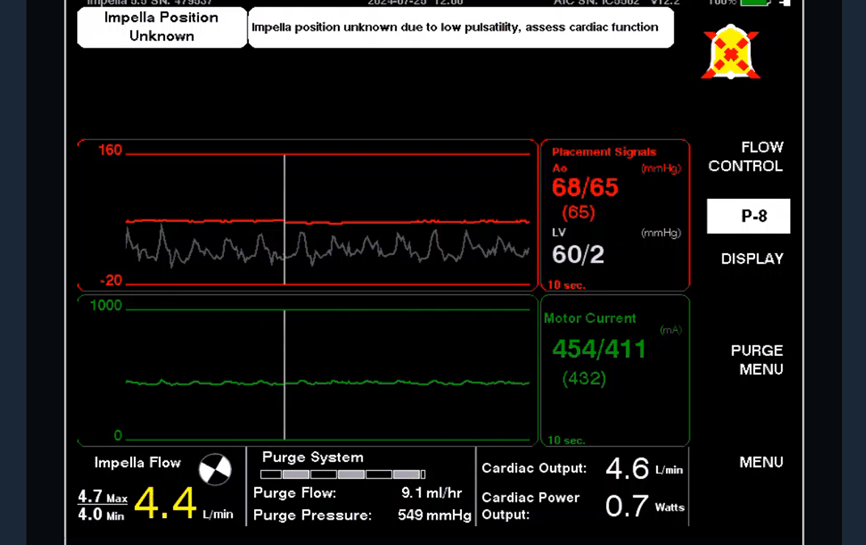
low native heart pulsatility, not generating enough pressure difference across the aortic valve.
bonus: is this patient supported?
500
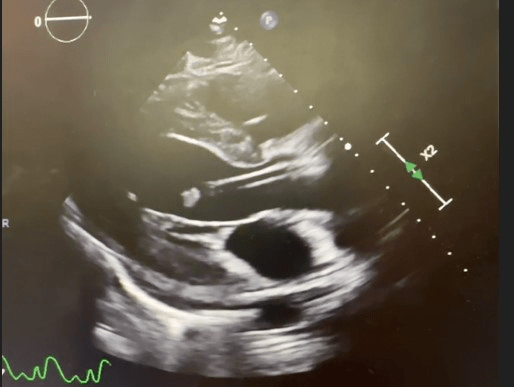
What is going on with the placement of this impella?
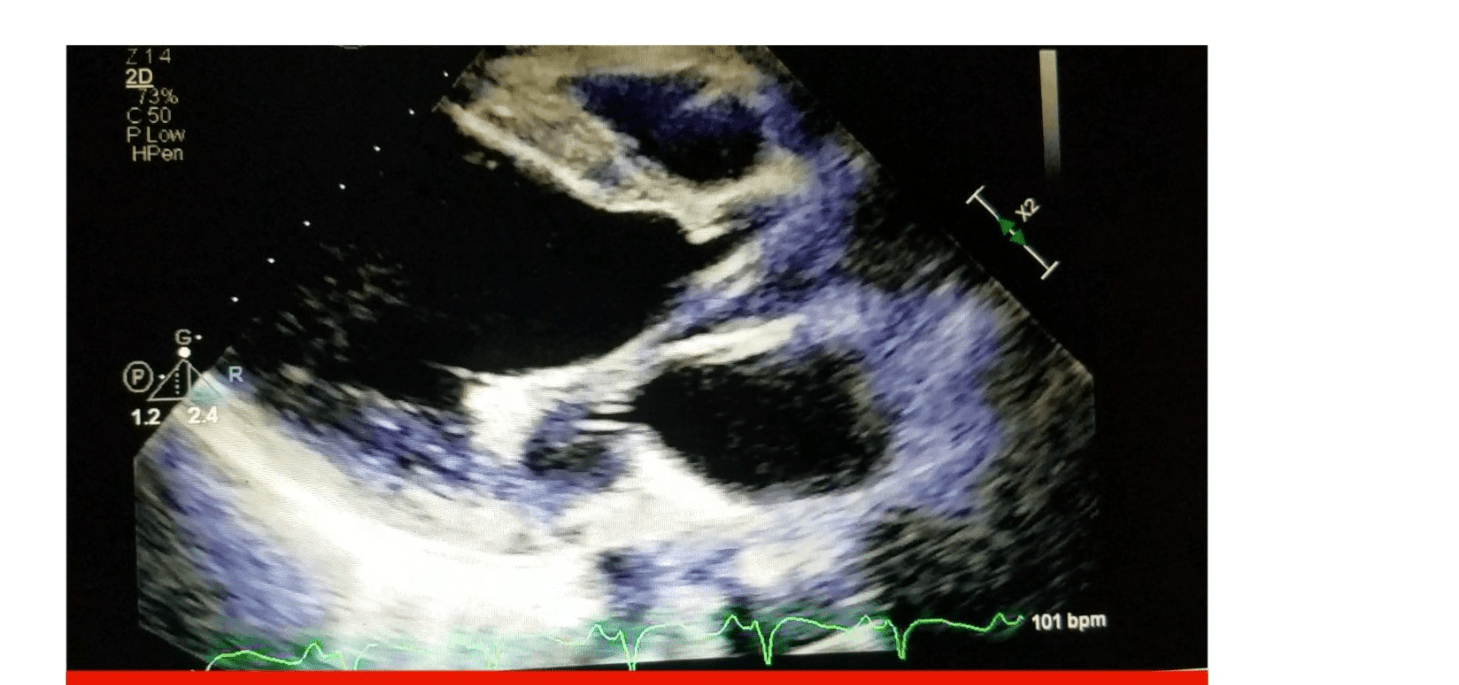
caught in papillary muscle. not properly positioned
500
Impella at P-9 and suction alarms present. What questions are you going to ask to troubleshoot?
what is CVP? What is MAP/CO? Has the patient moved? When was the last echo? drips?
RVF? hypovolemia? Positioning?