Lumbar's Anatomy
Switchin' Up Positions For Yuh
What's your Pathology?
Anatomy ID
Name the Exam/CR
100
A portion of the lamina located btw the superior and inferior articular processes is called the:
Pars interarticularis
100
What topographic landmark corresponds to the L2-L3 level?
Lower costal margin
100
Lateral curvature of the vertebral column:
8. Scoliosis
100
Name the anatomy: A, B, C
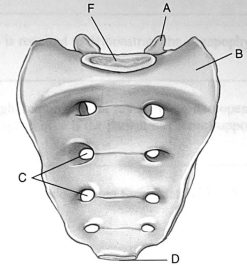
A. (L) Superior articular process
B. (L) Ala of sacrum
C. (R) Sacral foramina btw S2-S4
100

AP/PA Lumbar Spine
Pt: recumbent, knees flexed to reduce lumbar curve, hands out of LF
CR: ⊥ beam, iliac crest (14x17), MSP
IR: 14x17, Portrait
T: 85±5 / 25-80 / 40” SID / ↑Expiration
200
The superior and inferior vertebral notches join together to form the:
Intervertebral foramina
200
T/F: It is possible to shield females for an AP projection of the sacrum or coccyx if the gonadal shields are correctly placed.
False
200
Fx of vertebral body c/b hyperflexion force:
3. Chance fx
200
Name the anatomy: E, F, G, H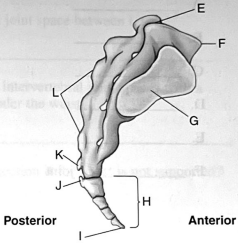
E. Sacral canal
F. Sacral promontory
G. (R) Auricular surface (SI jt)
H. Coccyx
200

AP Axial Sacrum
Pt: Recumbent, knees supported
CR: 15° cephalic, 2” ↑ symph/2” ↓ ASIS, MSP
IR: 8x10, Portrait
T: 85±5 / 6-10 / 37” SID / Suspend respiration
300
The small foramina found in the sacrum are called:
Pelvic (anterior) sacral foramina
300
T/F: The female gonadal dose is approx. equal for either AP or PA projections of the lumbar spine.
False, 20-30% less dose
300
Congenital defect in which the posterior elements of the vertebrae fail to unite:
1. Spina bifida
300
Name the anatomy: A, B, C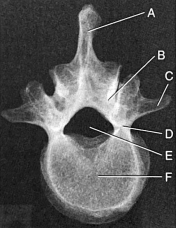
A. Lumbar spinous process
B. Lamina
C. (L) Transverse process
300

AP Axial Coccyx
Pt: Recumbent, knees supported
CR: 10° caudal, 2” ↑ symph/2” ↓ ASIS, MSP
IR: 5x5, 6x6
T: 80±5 / 4-6 / 40” SID / Suspend respiration
400
What is another term for sacral horns?
Cornua (cornu, sing.)
400
Why should knees and hips be flexed for a recumbent AP projection of the L-spine?
To lower OID by reducing lumbar curvature
400
Most common at L4-L5 level, may result in sciatica:
2. HNP
400
Name the anatomy: A, D, F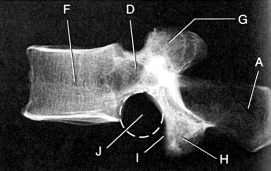
A. Spinous process
D. Pedicle
F. Lumbar Body
400

(L) Lateral Lumbar Spine
Pt: Recumbent, (L) side down closest to IR
CR: ⊥ beam, @ iliac crest, long axis of spine
IR: 10x17, Portrait
T: 85±5 / 25-80 / 40” SID / ↑Expiration
500
Name the mobility type and movement type for the (A) Zygapophyseal joint and (B) Intervertebral joint.
(A)
Mobility: diarthrodial
Movement: plane (gliding)
(B)
Mobility: Amphirathrodial (slightly movable)
Movement: N/A
500
T/F: A lead mat or masking for lateral positions of the L-spine should not be used with digital imaging.
False
500
Forward displacement of one vertebra onto another vertebra:
4. Spondylolisthesis
500
Name the anatomy: A, B, C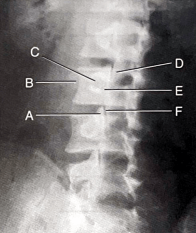
A. Superior articular process (ear), L3
B. Transverse process (nose), L3
C. Pedicle (eye), L3
500

Oblique Lumbar Spine, LPO/RPO
Pt: recumbent, obliqued 45°
CR: ⊥ beam, 2” ↑ iliac crest, 2” medial to upside ASIS
IR: 10x17, Portrait
T: 85±5 / 25-80 / 40” SID / ↑Expiration
600
Compared with the spinous processes of the C-spine/T-spine, the lumbar spinous processes are:
Larger and more blunt
600
Which set of z/p jts of the L-spine is best demonstrated with an LAO position?
Upside, farthest from IR (Right)
600
Inflammatory condition that is most common in males in their 30s:
7. Ankylosing spondylitis
600
Name the anatomy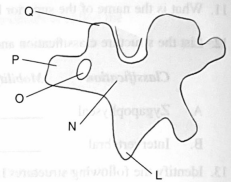
L. Inferior articular process (leg)
N. Pars interarticularis (neck)
O. Pedicle (eye)
P. Transverse process (nose)
Q. Superior articular process (ear)
600

L5-S1 Spot Lateral Lumbar Spine
Pt: Recumbent, (L) side down closest to IR
CR: 5°-7° caudal (no support)/⊥ beam (w/support), 1.5” ↓ iliac crest, 2” posterior to ASIS
IR: 8x8, 6x6
T: 90±5 / 25-80 / 39” SID / Suspend respiration
700
Each SI joint opens obliquely _________° (degrees) posteriorly.
30°
700
How much rotation is required to demonstrate the z/p jt space btw L1-L2?
50°
700
Dissolution and separation of the pars interarticularis:
6. Spondylolysis
700
Name the exam and anatomy: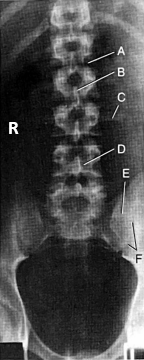
AP Lumbar Spine
A. Intervertebral disk space, L1-L2
B. Spinous process, L2
C. (L) Transverse process, L3
D. (L) Lamina, L4
E. (L) Ala of sacrum
F. (L) Sacroiliac joint
700

AP Axial SI joints
Pt: supine, knees supported
CR: 30° cephalic, 2” ↓ ASIS/ 2" ↑ symph, MSP
IR: 10x12, Landscape
A: SI jt centered, jt spaces & L5-S1 open
T: 85±5 / 6-10 / 34” SID / Suspend respiration
800
The anterior/superior ridge of the upper sacrum is called:
Promontory
800
What type of CR angulation should be used for the lateral L5-S1 projection if the waist is not supported?
5°-8° caudal
800
A type of fx that rarely causes neurologic deficits:
5. Compression fx
800
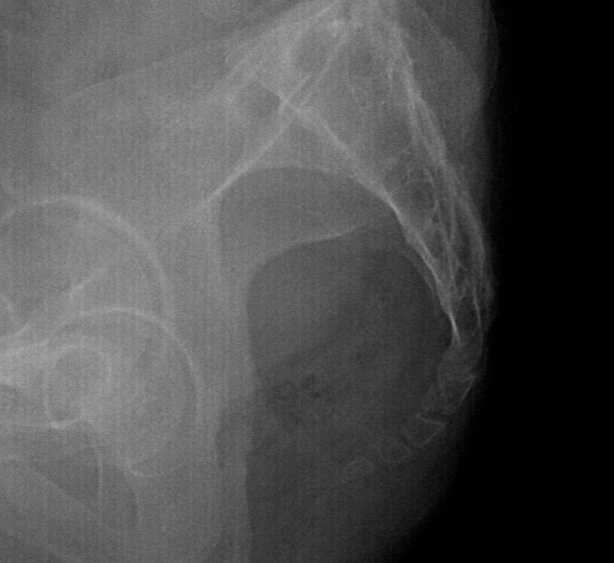
Name the exam and anatomy: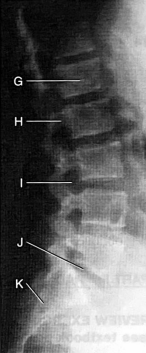
(L) Lateral Lumbar Spine
G. Body, L1
H. (R/L) Superimposed pedicles, L2
I. Intervertebral foramina, L3-L4
J. Intervertrbal disk space, L5-S1 (Spot)
K. Sacrum
800

Oblique SI joints, LPO (Right SI jts)/RPO (Left SI jts)
Pt: Supine, obliqued 25°-30°
CR: ⊥ beam, 1” medial to upside ASIS, level of ASIS
IR: 10x12, Landscape
T: 85±5 / 6-10 / 40” SID / Suspend respiration
900
The angle of the mid-lumbar spine z/p joints in relation to the midsagittal plane is _____________.
45°
900
For the lateral L5-S1 projection, the CR is // to the _______ plane.
Interiliac
900
T/F: Ankylosing spondylitis usually requires an increase in manual exposure factors.
False, none
900
Name the exam and anatomy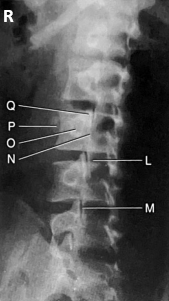
RPO Oblique Lumbar Spine
L. (R) Inferior articular process (leg), L3
M. Zygapophyseal joint, L4-L5
N. (R) Pars interarticularis (neck), L3
O. (R) Pedicle (eye), L3
P. (R) Transverse process (nose), L3
Q. (R) Superior articular process (ear), L3
900
Lateral Sacrum & Coccyx
Pt: lateral recumbent, hip/knees flexed
CR: ⊥ beam, level of ASIS, 3"-4" posterior to ASIS
IR: 8x10, Portrait
T: 90±5 / 20-30 / 40” SID / Suspend respiration
1000
The pars interarticularis is found btw the ___________ and _________ __________ __________.
Superior, inferior articular processes
1000
T/F: A kVp range of 90-100 can be used for a lateral L5-S1 projection when using a digital imaging system.
True
1000
Which of the following conditions is often diagnosed by prenatal ultrasound?
A. Scoliosis
B. Spina bifida
C. Spondylolisthesis
D. Ankylosing spondylitis
B. Spina bifida
1000
Name the anatomy: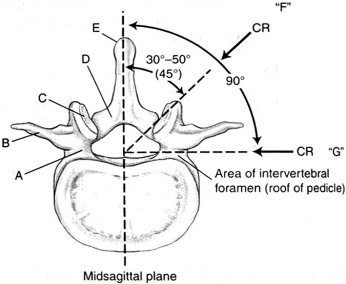
A. (R) Pedicle
B. (R) Transverse process
C. (R) Superior articular process/facet
D. (R) Lamina (pars interarticularis)
E. Spinous process
F. (L) Zygapophyseal joint
G. Intervertebral foramina
1100
The degree of obliquity required for an oblique projection at the T12-L1 level is approx _________, whereas the L5-S1 spine level requires a(n) _______ oblique. Therefore, a(n) ______ oblique is performed for the general lumbar spine.
50°, 30°, 45°
1100
Which projection or method is designed to demonstrate the degree of scoliosis deformity btw the primary and compensatory curves as part of the scoliosis study?
Ferguson method
1100
Anterior wedging and loss of vertebral body height are characteristics of:
A. Chance fx
B. Spina bifida
C. Compression fx
D. Spondylolysis
C. Compression fx
1100
Name the anatomy: D, F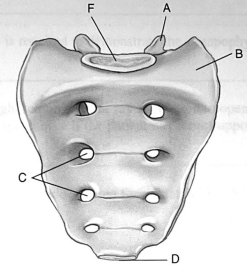
D. Apex of Sacrum
F. Promontory
1200
List the specific joints or foramina that are demonstrated with the following L-spine positions:
A. LPO
B. RPO
C. Lateral
D. RAO
E. LAO
A. LPO = (L) ⬇️ z/p jts
B. RPO = (R) ⬇️ z/p jts
C. Lat = intervertebral foramina
D. RAO = (L) ⬆️ z/p jts
E. LAO = (R) ⬆️ z/p jts
1200
What two things can be done to reduce the high amounts of scatter reaching the IR during a lateral projection of the sacrum and coccyx?
1. lead mat behind pt
2. close collimation
1200
Select the imaging modality that best demonstrates each of the following pathologic features or conditions.
(Choose from MRI, CT, Myelography, BD, NM)
A. Osteoporosis
B. Soft tissues of L-spine
C. Structures w/in subarachnoid space
D. Inflammatory conditions such as Paget disease
E. Compression fx of L-spine
A. BD
B. MRI
C. MRI, Myelo
D. NM
E. CT
1200
Name the anatomy: D, E, F
D. (L) Pedicle
E. Vertebral foramen
F. Lumbar body
1300
Why should a single lateral projection of the sacrum and coccyx be performed rather than separate laterals of the sacrum and coccyx?
to decrease gonadal dose
1300
Name the anatomy: I, J, K, L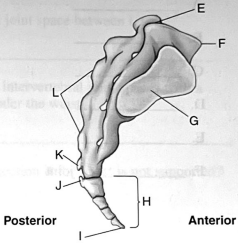
I. Apex of Coccyx
J. Horn (Cornu) of Coccyx
K. Sacral Horn (Cornu)
L. Median sacral crest
1400
T/F: The pelvis must remain as stationary as possible when positioning for the hyperextension/hyperflexion projections.
True
1400
Name the anatomy: D, E, F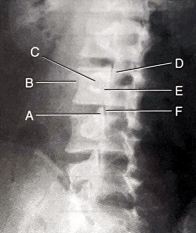
D. Inferior articular process (leg), L2
E. Pars interarticularis (neck), L3
F. Zygapophyseal joint, L3-L4
1500
A r/g of an AP projection of the L-spine reveals that the SI jts are not equidistant from the spine. The R ala of the sacrum appears wider, and the left SI joint is more open than the right. Which specific position error is evident on this graph?
Reduce RPO rotation, rotate more to the left
1500
Name the anatomy: G, H, I, J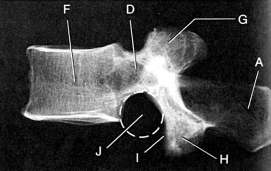
G. Superior articular process
H. Inferior articular process
I. Inferior articular facet
J. Inferior vertebral notch (intervertebral foramen)