A
B
C
D
E
100
You are taking care of a 32 yo G1P0 at 28 weeks gestation. She comes into the office stating that her mother has shingles. Your patient is concerned because she has never received her chickenpox vaccine. Is she at risk of her fetus developing congenital varicella syndrome?
no, Herpes zoster poses no risk, but chickenpox (varicella zoster) would be really bad.
100
A patient has a prolonged stage 3 of labor lasting about 2 hours. If this is caused by the placenta growing through the myometrium into the surrounding tissue, what is the likely diagnosis?
placenta percreta
100
You are working with your attending to assess the risk of a patients fetus have a trisomy. You perform a cell-free DNA test on the patient, which comes back negative. Based on these results, your attending states no further testing needs to be done, and that there is no possible way for the fetus to have trisomy 21. Why should your patient trust the advice of a facebook post more than that of your attending?
cfDNA testing is just a screening tool, there can be false positives and negative. Only definitive test is amniocentesis or CVS
100
A G1P0 patient presents at 12 weeks gestation with vaginal bleeding. PE shows the os is closed, and fetal hearth rhythms are present. US shows that the patient may have marginal placental previa. If the mother's blood type is A-, would you recommend a RhoGam shot at this time?
yes
100
You are evaluating a fetus at 20 weeks gestation using a fetal heart monitor. At this point in time, the cardiac activity is consistently around 150 with no variability. Should you be worried?
No, absence of variability before the 24th week is normal. Absent variability after the 28th week indicates an ANS defect.
200
You are evaluation a pregnant patient using a fetal heart monitor. You keep seeing weird V-shaped decelerations on the monitor. Compression of what structure is most likely causing this issue?
umbilical cord
200
You are evaluating a Rh+ infant who was born to an Rh- mother. You want to perform the Coomb's test so that you can see whether Abs against the fetal RBCs were made. Your attending tells you that in order to do the Direct Coombs tests, you take maternal blood, add the coombs reagent, and if it agglutinates, then the result is positive. Why should your attending go beg for a job at Auntie Annies Preztels?
Direct Coombs test is only on fetal blood, doing the test on maternal blood wouldn't show a thing. Would need to do indirect coombs test if you wanted to use maternal serum.
200
During labor, the infants head is noted to be 2 cm below the level of the ischial spine. This is needed to gather information on what measurement of labor?
station
200
A pregnant patient tests positive for pooling, ferning, and nitrazine test. What is the most basic diagnosis?
Rupture of membranes
300
A 34 yo G2P1001 patient presents to the clinic for a routine check-up. While she is there, you realized that the attending never got her blood type during previous visits. You decide to screen her and see that she is A-, while records indicate that her first infant was AB+. Indirect Coombs test is positive. Would you give her RhoGam at this visit?
Nope, wouldn't do a thing
400
A G2P1001 27yo patient at 38 weeks gestation presents to the hospital in active labor. Hx shows that she was given a RhoGam shot during her last pregnancy, does she need to receive another during this delivery?
Yes
400
A 23yo G1P0 female at 6 weeks gestation presents to the clinic for her first evaluation. You decide to run titers to check her for TORCH infections. She comes back negative for everything, except there is IgG present for T. Gondii. If her IgG levels are at 500, and her IgM levels are 0, what is the risk of the fetus contracting the disease in utero?
pretty much 0 percent. IgG only signifies that it was more than likely a past infection, and not a current one.
400
You see this FHR tracing, are you concerned?
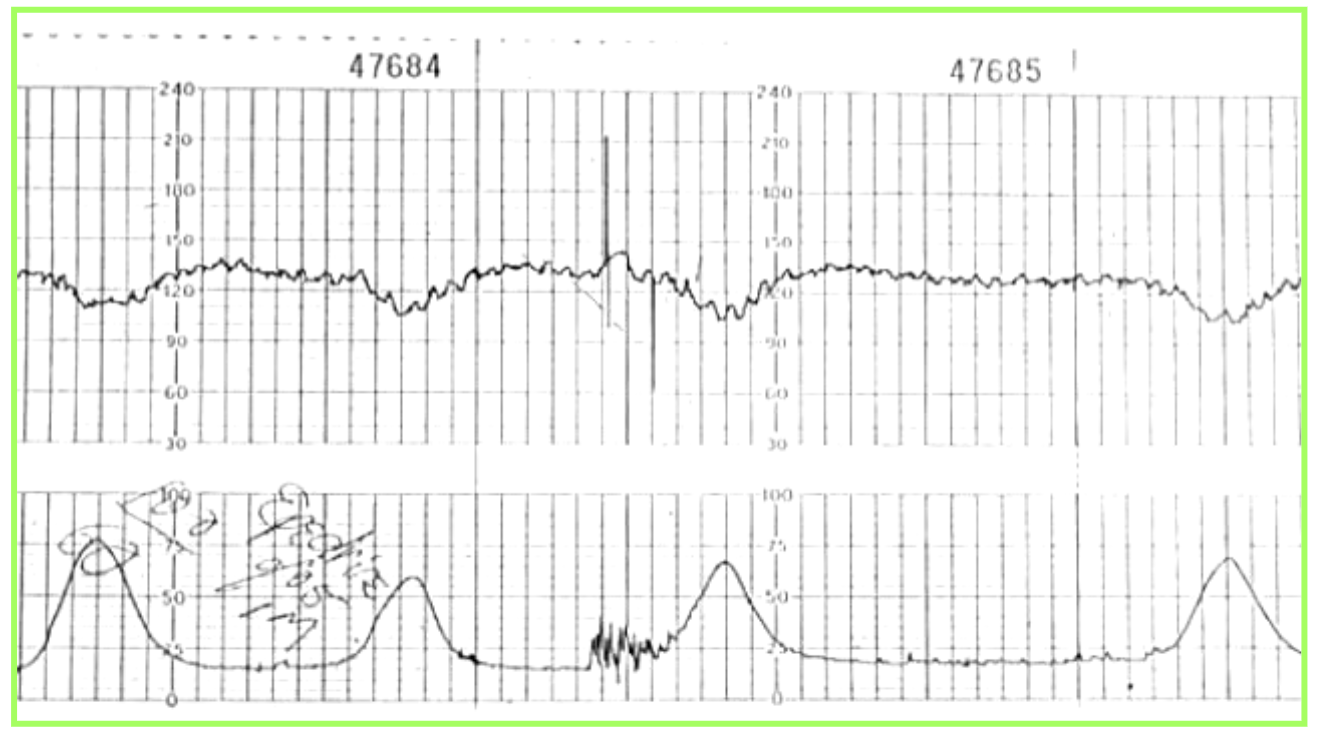
early decels, probably normal
400
A G1P0 female at 36 weeks gestation presents for screening of GBS. She is found to be positive at the time of the visit. Would it be appropriate to start her on antibiotics immediately, given the risk that GBS poses to a newborn?
no, treat right before birth
500
A pregnant patient at 35 weeks gestation presents to the clinic stating she is in labor. Pelvic exam show she is at 0/0/-5. The contractions get better when she is laying down, and US shows intact membranes. What is the most likely diagnosis?
false labor
500
You are evaluating a patient in labor who is having contractions every 2 minutes, as noted on the external FHR monitor. Labor has been progressing for a while, but the patient is not dilating any further, they are persistently at 4 cm for the past 10 hours. Your attending tells you that it is probably cervical Failure to Dilate, because the external monitor shows strong contractions, and that a c-section is needed. Why do I think your attending got his medical license from Craigslist?
You can't tell from an external monitor how strong the contractions are, you need an internal monitor. She could just be having weak contractions.
500
You give a patient in labor pitocin to help stimulate contractions. Shortly after, you notice on FHR that the fetus is losing variability and beginning to show late decelerations. What should you do next?
stop pitocin
500
What is the ideal fetal position just before labor if you want it to progress as smoothly as possible?
OA