Giving Birth/ labor & delivery
Intrapartum monitoring/assessment
Pain management
Therapeutic nursing /procedures
Nursing care during labor & delivery
100
Contractions that help the mother's body prepare for true labor; they do not indicate that labor has begun.
What is Braxton-Hicks contractions
100
These are the Four Characteristics used to describe contractions.
•Resting Tone •Intensity •Duration •Frequency
100
Epidurals and Spinals cannot be given when a patients lab results show _________________, which can be seen in cases of PIH and HELLP.
What are low platelets?
100
The nurse recognizes these 5 Ps are essential for successful vaginal delivery.
1.Passage (the pelvis)
2.Psyche (the response of woman)—
3.Position (maternal position)
4. Passenger (the fetus)
5. Power (the contractions)
100
A nurse explains these nursing actions and teachings as part of initial process for laboring patient.
●Monitor V/S, FHR, cervical changes and fetal station
●Diet- usually clears, ice chips, or NPO
●18 g (20 smallest) IV in hand/forearm, avoid AC
●Encourage rest now as you’ll need energy later
●Frequent voids to ensure fetal descent
●Provide comfort measure for pain
200
The 3 phases within the first stage of labor
What is latent, active, and transition?
200
This is the difference between Cervical dilation, effacement and station.
What is effacement means that the cervix stretches and gets thinner from 0-100%, Dilatation means that the cervix opens from 0-10cm and station is the fetal descent in relation to the ischial spine (-3 to +3).
200
A form of anesthesia that is administered to mothers in labor which numbs the pain of labor without affecting the mother's ability to push.
What is an epidural?
200
A small cut that prevents tearing during delivery.
What is an episiotomy
200
This is the primary goal of an external cephalic version (ECV)
To turn the fetus to a vertex position to allow for a vaginal delivery
300
The difference between true and false labor
What is true labor contractions last more than 30 seconds at the onset and get progressively longer, up to 60 seconds, whereas false labor contractions vary in length.
300
This nurse recognized this FHR Category as an emergency.
Describe the FHR indications for this category.
What is a Category III
300
These are some applications of Nonpharmacologic Techniques.
What is:
Back counter pressure
Mental stimulation (guided imagery, focal points, music)
Aromatherapy
Mind-Body Stimulation/ massage
Hydrotherapy
Breathing Techniques
Modified-Paced Breathing
300
A patient is to have an amniotomy to induce labor. The nurse recognizes this priority assessment/intervention after AROM:
What is to assess the fetal heart rate?
(FHR)
300
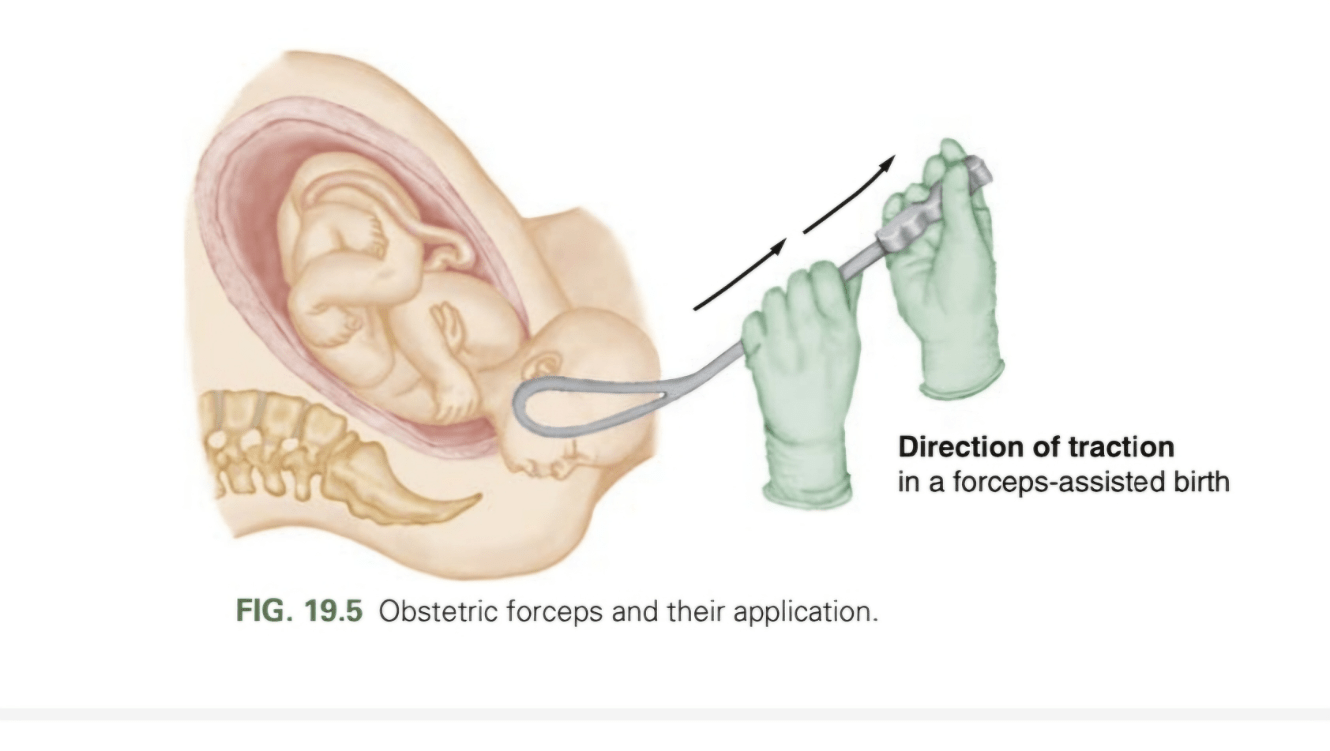
What tool are they utilizing?
400
This terminology refers to a medical emergency when the umbilical cord becomes compressed between the cervical opening and the baby's head.
What is Umbilical cord prolapse
400
This test is used for real time view of physical and physiological characteristics of the fetus to determine fetal wellebing.
Biophysical Profile
Includes 5 parts, graded with either 0 or 2 points for each
Fetal Breathing movements
Fetal Tone
Fetal Movement / Gross Body Movements
Amniotic Fluid Volume
NST (Fetal Heart Rate)
TOTAL SCORE
8-10 = normal - low risk of chronic fetal asphyxia
○4-6 = abnormal – suspect to chronic fetal asphyxia
○<4 – abnormal – strongly suspect to chronic fetal asphyxia
400
These medications can be used to control bleeding and reduce the incidence of PPH
What is oxytocin, misoprostol, methergine, hemabate and txa.
400
The nurse explains to the patient that these are different methods to induce/augment labor.
What is Cervical ripening: prostaglandins, Oxytocin, AROM, Foley bulb
400
These factors contribute to Cephalopelvic Disproportion (CPD)
•Fetal size, presentation, and position
•Size and shape of the maternal pelvis
•Quality of the uterine contractions
500
These 7 cardinal movements assist the fetus through the birth process.
• Engagement: The baby’s head enters the pelvic inlet.
• Descent: The baby’s head descends further into the pelvic cavity. This occurs throughout labor, aided by uterine contractions, amniotic fluid pressure, and maternal pushing.
• Flexion: As the baby’s head descends and encounters resistance from the pelvic bones and soft tissues, it naturally tucks its chin toward its chest, presenting the smallest head diameter to the birth canal.
• Internal rotation: The baby’s head rotates about 90 degrees to align with the long axis of the body as it moves down the pelvis, typically from an orientation where the baby is facing sideways to facing the mother’s back.
• Extension: As the baby’s head passes under the pubic bone, it extends backwards, with the chin leaving the chest, so that the head can fully emerge.
• External rotation: After the head is delivered, it rotates again so that the baby’s face is turned towards one of the mother’s inner thighs, allowing the shoulders to align with the pelvic outlet.
• Expulsion: Following delivery of the head and shoulders, the rest of the baby’s body is delivered relatively easily and quickly.
500
This acronym is used when observing fetal heart rate characteristics.
What is VEAL CHOP: Variable deceleration= Cord compression; Early deceleration = Head compression Acceleration = Okay/Oxygenation; Late deceleration= Placental insufficiency
500
These pharmacological pain managements can be utilized during labor/ C-section.
What is:
Regional Anesthesia
Pudendal Block
Local Anesthesia
Epidural Block
Spinal Block
Opioid Analgesics
General Anesthesia
500
The most commonly used method to rate the readiness of the cervix for induction of labor.
What is the Bishop Score? The Bishop Score gives points to 5 measurements of the pelvic examination dilation, effacement of the cervix, station of the fetus, consistency of the cervix, and position of the cervix.
If the Bishop score is 8 or greater the chances of having a vaginal delivery are good and the cervix is said to be favorable or "ripe" for induction. If the Bishop score is 6 or less the chances of having a vaginal delivery are low and the cervix is said to be unfavorable or "unripe" for induction.
500
This manuever is used as the first step when a Shoulder Dystocia is noted.
What is McRoberts?