Myeloid Leukemia
Myeloproliferative Neoplasms
Lymphoid Leukemia
Board Games
100
A 48-year-old woman comes to her physician because of a 2-month history of dull left-upper-quadrant pain and chronic fatigue. Laboratory test results include a WBC count of 38 × 109/L, 95% neutrophils, and 2% basophils. A bone marrow biopsy is performed. Genetic testing confirms the diagnosis, and the patient is treated with a drug that inhibits the BCR-ABL oncogene product in this disease.
Which of the following signaling pathways does this drug inhibit?
GPCR signaling
Nf-κB signaling
Steroid receptor signaling
TGF-β signaling
Tyrosine Kinase Signaling
5. Tyrosine Kinase Signaling
CML is characterized by marked neutrophilic leukocytosis and may present with abdominal pain and fatigue.
CML is responsive to imatinib, which inhibits the constitutive tyrosine kinase encoded by the BCR-ABL fusion gene
100
Do any Myeloproliferative Neoplasms present with fever?
No
100
What is the most common childhood malignancy?
A. CLL
B. ALL
C. MCHL
D. DLBCL
B. ALL(acute lymphoblastic leukemia)
100
What is Adam's favorite board game?
1. Payday
2. Monopoly
3. Sorry
4. Sequence
2. Monopoly
200
A 63-year-old woman comes to the office because of worsening fatigue for the past 2 weeks. She has also started noticing bruising on her skin and lips. She denies experiencing pain. The patient appears pale on physical examination. No enlarged lymph nodes are present, nor is there hepatosplenomegaly. Nonblanchable petechiae are present on the lower limbs. A complete blood count reveals the following:
Hemoglobin: 8 g/dL (↓)
Platelets: 67,000/mm3 (↓)
Leukocytes: 3000/mm3
Myeloblasts: 30%
Promyelocytes: 10%
Myelocytes: <5%
Metamyelocytes: <5%
Mature myelocytes: 50%
The patient’s peripheral blood smear is indicative of auer rods
Which of the following is most likely to be associated with the patient’s likely condition?
t(9;22)
Decreased vWF activity
> 20% lymphoblasts in the bone marrow
Increased leukocyte alkaline phosphatase
Microangiopathic Hemolytic Anemia
5. Microangiopathic Hemolytic Anemia
APL is associated with auer rods on PBS, t(15;17), and >20% myeloblasts
Auer rods in APL inappropriately activate coagulation cascade and is associated with DIC, thus showing one of its symptoms (MAHA)
200
A 65-year-old man comes to the physician because of a 6-month history of progressive fatigue and abdominal pain. Physical examination shows pale mucous membranes and splenomegaly. Hemoglobin concentration is 9.1 g/dL and leukocyte count is 3,400/mm3. Peripheral blood smear shows nucleated red blood cells and teardrop poikilocytosis. A Janus kinase 2 gene mutation is present. Which of the following is the most likely underlying mechanism of this patient's condition?
Viral replication in lymphoid cells
Lymphocytic infiltration of reticuloendothelial system
Fibrosis in the bone marrow
Translocation between chromosome 9 and 22
Elevated levels of circulating hepcidin
Fibrosis in the bone marrow
200
A 7-year-old girl is brought to the physician by her mother because of a 2-week history of generalized fatigue, intermittent fever, and progressively worsening shortness of breath. Physical examination shows pallor, jugular venous distention, and nontender cervical and axillary lymphadenopathy. Inspiratory stridor is heard on auscultation of the chest. The liver is palpated 3 cm below the right costal margin. Her hemoglobin concentration is 9.5 g/dL, leukocyte count is 66,000 mm3, and platelet count is 102,000 mm3. An x-ray of the chest shows a mediastinal mass. A bone marrow aspirate predominantly shows leukocytes and presence of 35% lymphoblasts. Which of the following additional findings is most likely in this patient?
A. t(8;14) translocation
B. Smudge cells
C. Positive myeloperoxidase staining
D. t(9;22) translocation
E. Reed-Sternberg cells
F. Positive CD3/CD7 staining
F. Positive CD3/CD7 staining
(T-cell is the least common of the ALLs. It can commonly be seen in adolescent males. It presents as a mass, especially as a mediastinal mass on X-ray (thymus is involved).
Quick Tip- lower numbers for CD-markers (CD3+, CD5+, CD7+)
200
What is Uty's favorite board game?
A. Catan
B. Monopoly
C. Chess
D. Scrabble
D. Scrabble
300
A 73-year-old woman who resides in a nursing home is being examined for an infection on her foot and increasing fatigue. She has had similar infections in the past year, typically after small scrapes to her lower extremities. She takes atorvastatin and a daily multivitamin. Physical examination shows an erythematous lesion on her foot measuring 2 cm by 2 cm. Laboratory studies show a hemoglobin of 9.8 g/dL, mean corpuscular volume of 110, RBC count of 3.5 million cells/mcL, and WBC count of 3000 cells/mcL. A bone marrow biopsy specimen shows hypercellularity and dysplasia with 10% myeloblasts.
This patient’s current disorder may progress into which of the following conditions?
1. Acute lymphoblastic leukemia
2. Acute myelogenous leukemia
3. Chronic myelogenous leukemia
4. Aplastic anemia
5. Chronic lymphocytic leukemia
2. Acute myelogenous leukemia
Myelodysplastic syndromes (“preleukemia”) are a group of hematologic malignancies characterized by clonal proliferation leading to cytopenias.
AML is characterized by >20% blasts, while myelodysplastic syndromes have <20%.
Patient fatigue likely from anemia, and recurrent skin infections from leukopenia. BM showing hypercellularity, dysplasia, and myeloblasts <20% confirms MDS. MDS has a 30% chance of developing into AML
300
A 50-year-old African-American woman comes to the physician because of right elbow pain for the past 12 hours. The pain is currently at 7 out of 10 in intensity. She has not had any trauma to the right elbow. She also reports general malaise. She had a miscarriage at the age of 37 years. One year ago, she had carpal tunnel syndrome that was treated with a volar splint. Three months ago, she was diagnosed with thrombophlebitis, which responded well to treatment with ibuprofen and compression therapy. She runs 5 km (3.1 miles) per week. She works as an accountant. She drinks 1–2 glasses of wine on weekends. She is 171 cm (5 ft 7 in) tall and weighs 70 kg (154 lb); BMI is 24 kg/m2. Her temperature is 38.3°C (101°F), pulse is 110/min, and blood pressure is 130/80 mm Hg. On physical examination, the skin above her right elbow is erythematous and severely tender to palpation. Abdominal examination shows no abnormalities. Laboratory studies show:
Hemoglobin:13.5 g/dL
Leukocyte count: 9520/mm3
Platelet count: 853,000/mm3
Serum
Na+: 136 mEq/L
K+: 3.7 mEq/L
Cl-: 96 mEq/L
Ca2+: 11.0 mg/dL
HCO3-: 25 mEq/L
Glucose: 92 mg/dL
Creatinine: 1.0 mg/dL
Uric acid: 10.5 mg/dL
Further evaluation of this patient is most likely to show which of the following?
Mutation in Janus kinase 2 gene
Howell-Jolly bodies
Antibodies against citrullinated peptides
Calcium pyrophosphate dihydrate deposits
Anti-phospholipid antibodies
Mutation in Janus kinase 2 gene
300
A 69-year-old woman comes to the physician for a routine health maintenance examination. She feels well. Physical examination shows nontender cervical and axillary lymphadenopathy. The spleen is palpated 5 cm below the costal margin. Her leukocyte count is 12,000/mm3 and platelet count is 217,000/mm3. Further evaluation is most likely to show which of the following findings?
A. Ringed sideroblastsB. Teardrop cells
C. Smudge cells
D. Reed-Sternberg cells
C. Smudge cells (these are commonly found in CLL unlike ALL. Smudge cells reflect the fragility of peripheral lymphocytes which can be disrupted during preparation of blood smear which leads to smudging of the cells)
300
Athinas Fav Board game?
CHESS
MONOPOLY
BACKGAMON
STAR WARS REBELLION
SNAKES AND LADDERS
CANDYLAND
CHESS
400
A 59-year-old man comes to the office because of an unintentional 6.8-kg (15-lb) weight loss over the past 2 months. He also reports occasional night sweats. His history is significant for radiation exposure as a result of working in a uranium processing factory. Temperature is 37°C (98.6°F). On physical examination, the spleen tip is palpable. His leukocyte count is 126,000/mm3, and a peripheral blood smear is shown.

Which of the following test results is most likely to confirm the patient’s diagnosis?
1. Cytogenetic identification of t(9;22)
2. Elevated LAP score
3. Presence of JAK2 mutation
4. Lymph node biopsy showing Reed-Sternberg cells
1. Cytogenetic identification of t(9;22)
CML may present with unintentional weight loss, night sweats, splenomegaly, leukocytosis, and a peripheral smear revealing leukocytes of myeloid origin at various stages of development.
Definitive diagnosis depends on cytogenetic identification of the Philadelphia chromosome (a translocation between chromosome 9 and chromosome 22) or the BCR-ABL fusion product.
400
A 59-year-old woman is brought to the emergency department with an acute onset of weakness in her left hand that started 6 hours ago. She has not had numbness or tingling of the hand. Other than recent episodes of blurry vision and headaches, her medical history is unremarkable. She has one daughter who was diagnosed with multiple sclerosis at age 23. Her temperature is 36.7°C (98.1°F), pulse is 80/min, and blood pressure is 144/84 mm Hg. Examination shows facial erythema. There are mild scratch marks on her arms and torso. Left hand strength is slightly decreased and there is mild dysmetria of the left hand on finger-to-nose testing. The remainder of the neurological examination shows no abnormalities. Her laboratory studies show:
Hematocrit: 55%
Leukocyte count 14500/mm3
Segmented neutrophils: 61%
Eosinophils: 3%
Lymphocytes: 29%
Monocytes: 7%
Platelet count: 690,000/mm3
Her erythropoietin levels are decreased. CT scan of the head without contrast shows two focal areas of hypo-attenuation in the right frontal lobe. Which of the following is the most appropriate treatment to prevent complications of this patient's underlying condition?
Radiation therapy
Glucocorticoid therapy
Warfarin therapy
Imatinib therapy
Repeated phlebotomies
Interferon alpha
Repeated phlebotomies
400
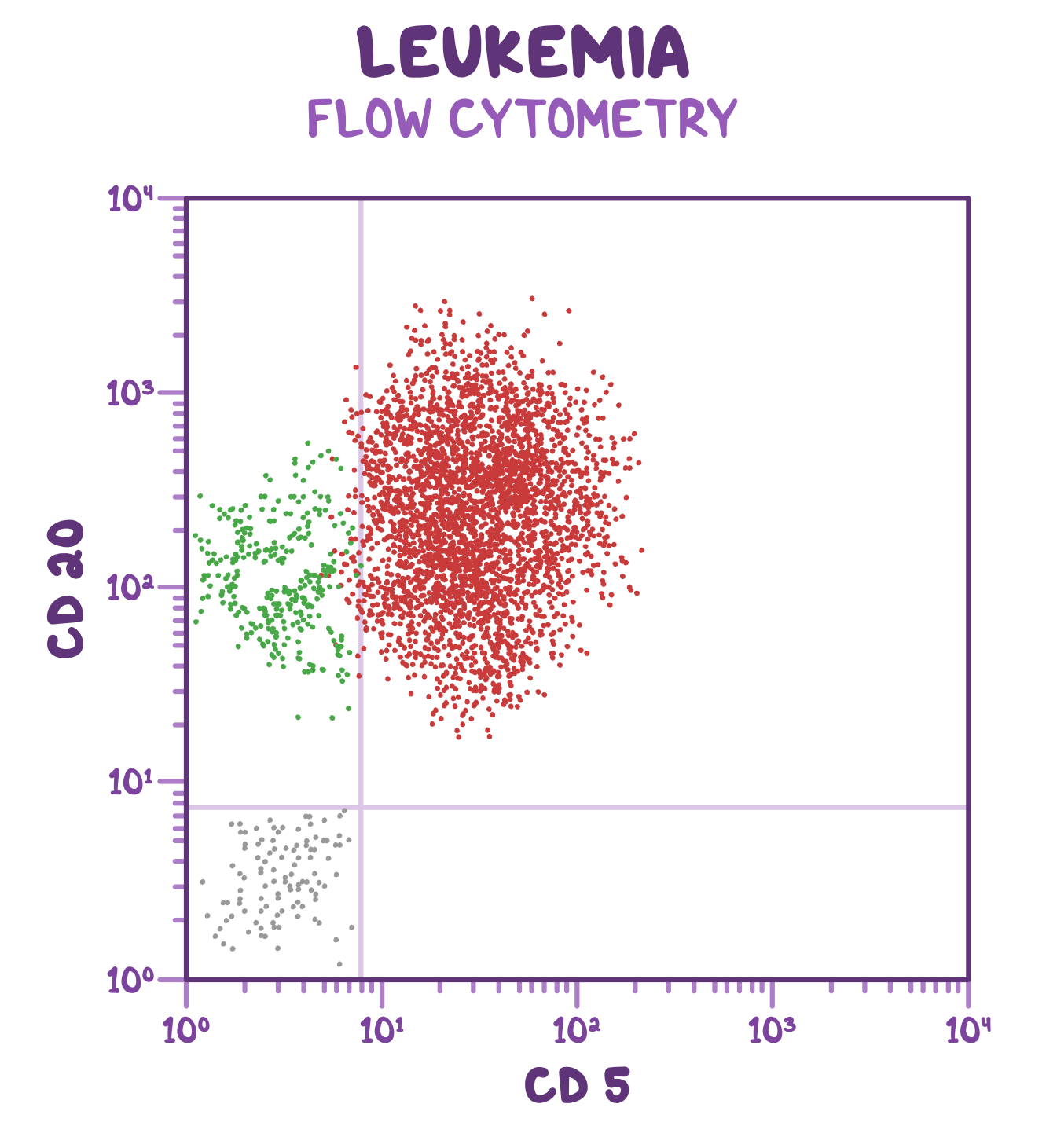
A 56-year-old man comes to the clinic for evaluation of abnormal results of a routine blood count. The patient does not have any symptoms of fatigue, malaise, fever, or shortness of breath. Past medical history is unremarkable. Temperature is 37.0°C (98.6°F), pulse is 95/min, respirations are 20/min, and blood pressure is 135/85 mmHg. Physical examination shows enlarged, firm, mobile cervical lymph nodes on both sides. Fecal occult blood is negative. Laboratory results are shown.
Laboratory values:
Hemoglobin 10 g/dL
Platelets 90,000/mm3
Leukocytes 20,000/mm3
Neutrophils 20%
Lymphocytes 75%
Eosinophils 2%
Basophils 1%
Monocytes 1%
After appropriate workup, flow cytometry is indicated which shows the following results.
A. Aplastic anemia
B. Chronic myeloid leukemia
C. Chronic lymphocytic leukemia
D. Hodgkin lymphoma
E. Hairy cell leukemia
C. CLL
(CLL/SLL is a monoclonal B cell tumor which is mostly asymptomatic or can present with B symptoms. Lymphocytosis (>5000/mL) is the most common laboratory finding. Diagnosis is established by flow cytometry findings of clonal B cell proliferation)
(Important note: CD5 is a common T cell marker, but CD5+ B cells are seen here)
500
A 65-year-old woman is in remission for lung cancer after aggressive treatment with surgery and chemotherapy. She finished her treatment 3 years ago. She smoked one-half pack of cigarettes daily for 40 years, quitting when she was diagnosed with cancer. Over the past month, she has noticed increasing fatigue and shortness of breath. She has also noticed bleeding from her gums. Her temperature is 37.3°C (99.1°F). On physical examination, she appears pale with bruising over the anterior aspect of her lower legs. Bone marrow biopsy reveals numerous myeloid blast cells.
Which of the following is the most likely risk factor for this patient’s newest condition?
1. Transfusion
2. Exposure to chemotherapy
3. HIV infection
4. Exposure to radon
5. Exposure to UV radiation
2. Exposure to chemotherapy
AML involves the malignant transformation of myeloid precursor cells and presents with fatigue, weakness, shortness of breath, bleeding, petechiae, bruising, and headaches.
AML may occur after exposure to chemotherapy, most commonly occurring three to five years or as a de novo mutation.
Specifically an alkylating agent
Also exposure to ionizing radiation, benzene and tobacco smoke may contribute
500
A 45-year-old woman comes to the physician for a 1-week history of headache, lightheadedness, and tingling of the hands and feet. Her medical history is significant for deep vein thrombosis and two spontaneous abortions at 12 and 15 weeks' gestation. Physical examination shows no abnormalities. Her serum erythrocyte count is 5.3 million/mm3, leukocyte count is 10,500/mm3, and platelet count is 1,120,000/mm3. A photomicrograph of a bone marrow biopsy obtained from the patient is shown. Which of the following is the most likely diagnosis? (Hint: its a myeloproliferative neoplasm)

Essential Thrombocythemia
500
A 4-year-old boy is brought to the emergency department by his parent because of a sore throat for the past 2 days. The patient’s parent reports that the patient feels tired all the time and has not been interested in playing his favorite video games over the last several weeks. Temperature is 38.3°C (101°F), pulse is 110/min, respirations are 24/min, and blood pressure is 105/65 mmHg. Physical examination shows pharyngeal erythema without exudates, mucosal pallor and petechiae on lower extremities. Abdominal examination reveals hepatosplenomegaly. Peripheral blood smear is shown below: 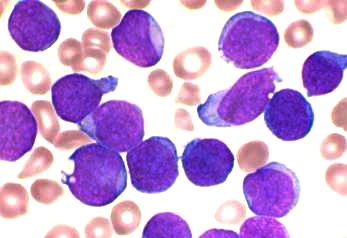
The cells stain positive for terminal deoxynucleotidyl transferase (TdT) and CD10. The cells identified in this patient’s peripheral blood smear are precursors to which of the following cell types?
Erythrocytes
Monocytes
Platelet
B lymphocytes
T lymphocytes
D. B lymphocytes
( B-cell lymphoblasts express CD10, CD19 and CD20. ALL occurs due to mutations in NOTCH1, t(12;21) or, rarely, t(9;22). It presents with findings of pancytopenia, hepatosplenomegaly, lymphadenopathy and/or mass effects. Lymphoblasts are characterized by positive nuclear staining for TdT. Bone marrow biopsy shows ≥20% lymphoblasts, and diagnosis is confirmed by flow cytometry)