Bacteria 1
Bacteria 2
Bacteria 3
Bacteria 4
Bacteria 5
Parasites
Parasites 2
Viruses
Viruses 2
Fungi
Fungi 2
100
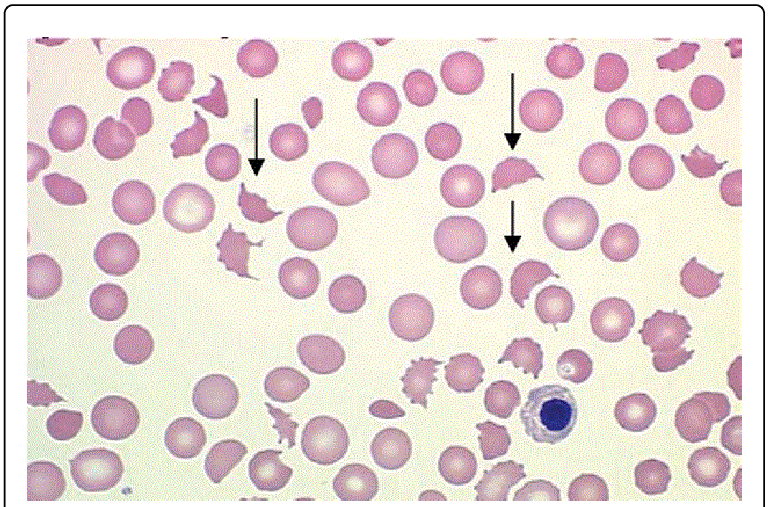
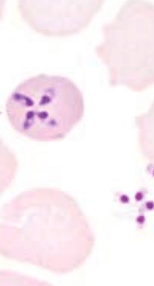
A 7-year-old boy presents to the emergency room with acute kidney failure. His initial lab work shows thrombocytopenia, and a blood smear shows:
What complication of STEC is this patient experiencing?
Hemolytic uremic syndrome
Hemolytic uremic syndrome is a toxin mediated microangiopathic injury that causes a prothrombotic state and causes intravascular microthrombi. it is well known for its three classical features of acute kidney failure caused by the occlusion of renal vessels, thrombocytopenia, and hemolytic anemia as shown in the photo above.
100
A 30 y.o. woman presents to clinic with increased frequency of urination, burning sensation when urinating, and suprapubic abdominal pain. Laboratory testing reveals that the organism is a non-motile. coagulase-negative, non-hemolytic, and urease-positive. What is the likely cause of the infection?
Staphylococcus saprophyticus
Reasoning: S. saprophyticus is the second most common cause of urinary tract infections behind uropathogenic E. coli. While you can differentiate the two species based on gram stain, E. coli is also urease negative while S. saprophyticus is urease positive. Proteus mirabilis is also a cause of urinary tract infections and is urease positive but can be differentiated from S. saprophyticus as Proteus mirabilis is motile and gram-negative.
100
Fourteen hours after birth, a neonate develops fever, hypotension, tachypnea, apnea, lethargy, poor feeding and vomiting. The newborn genetic screening panel returned normal. The mother reports no family history of any metabolic disorders. During one of her prenatal care visits, she remembers a doctor telling her she was colonized with “a bacteria of some kind” but declined treatment. What is the likely causative agent of the newborn’s illness?
Group B streptococci (Streptococcus agalactiae)
Reasoning: Group B strep is a major cause of disease in neonatal and perinatal periods. Mothers who are colonized by Group B strep can pass on the organisms to their child during birth. If the neonate becomes ill, they will often develop meningitis, septicemia, and pneumonia.
100
45-year-old man presents to the ER for a five-week history of cough with bloody sputum. He is HIV positive and has lived in several homeless shelters in Omaha. He also reports having night sweats and chest pain. He remembers other people in the shelter having similar symptoms as him. You perform an acid fast stain which shows:
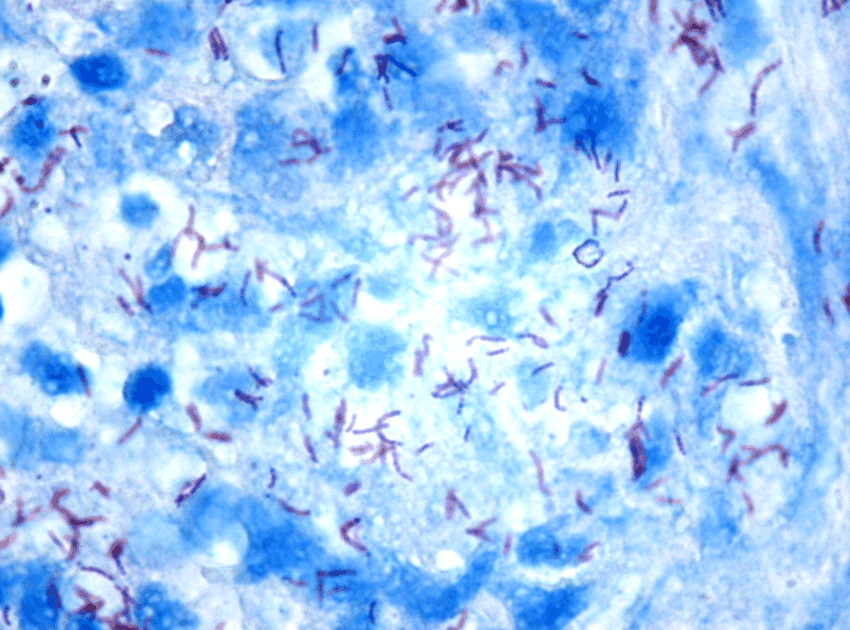
What organism is most likely responsible for his illness?
Mycobacterium tuberculosis
Reasoning: Mycobacterium tuberculosis is an acid-fast bacteria that causes cough with bloody sputum, night sweats, weight loss, chest pain, and fever. Living in close quarters like homeless shelters is a risk factor for getting TB as is being immunocompromised. Non-TB mycobacterium typically do not spread from person to person like TB does.
100
A 55-year-old woman is brought to the emergency department for confusion, cough, and diarrhea. Her and her family recently went on vacation to Richmond, VA and stayed in an old hotel where other people reported similar symptoms. Her past medical history include COPD and hypertension. She smokes 1 pack per day. On physical exam her oxygen saturation is 92% on room air. There are fine crackles bilaterally on chest auscultation. She was found to have hyponatremia upon further testing. What is the causative organism?
Answer: Legionella pneumophila
Explanation: Infection with Legionella typically occurs after aspiration of contaminated water/soil from air conditioning, hot tubs, and swimming pools. It is more commonly found in the elderly and risk factors include cruise ships, smoking, immunosuppression, and hospitalization. This patient is experiencing Legionnaires disease which is a lobar or interstitial pneumonia with gastrointestinal, and CNS involvement. Labs for diagnosis usually involve a urine antigen test. Hyponatremia is also common. The differential for this patient includes mycoplasma pneumoniae, but this bug does not cause GI or CNS involvement.
100
A 53-yo male presents to clinic with weight loss, fatigue, and steatorrhea. He tells you that his symptoms started after he got back from a hiking trip in Colorado where he drank out of "clean" stream. On microscopy of a stool sample, you see the following:

What is the causative organism?
Giardia lamblia
Giardia lamblia causes flatulence, nausea, and foul-smelling diarrhea acutely; steatorrhea and malabsorption syndromes chronically. History of drinking from a contaminated water source would raise suspicion, and the microscopy directly visualizes the trophozoite.
100
A 33 yo male presents with RUQ pain, nausea, and bloody diarrhea. He has no past medical history. He recently traveled on a cruise of the Caribbean around 2-3 weeks prior to symptom onset. He undergoes CT, which shows a liver abscess. What is the likely organism.
Answer: Entamoeba histolytica
Explanation: RUQ Pain and bloody diarrhea + tropical travel (trying to refer to poorer sanitation) + imaging showing liver abscess
100
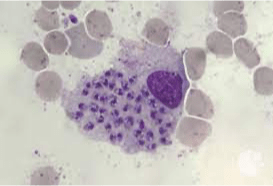
A 40-year-old man has recently undergone a kidney transplant and takes immunosuppressant drugs to prevent organ rejection. Three weeks after his transplant, he reports feelings of fatigue, malaise, muscle aches, and gastrointestinal distress. A biopsy of his small intestine shows this image. Which pathogen is most likely causing this patient’s symptoms?
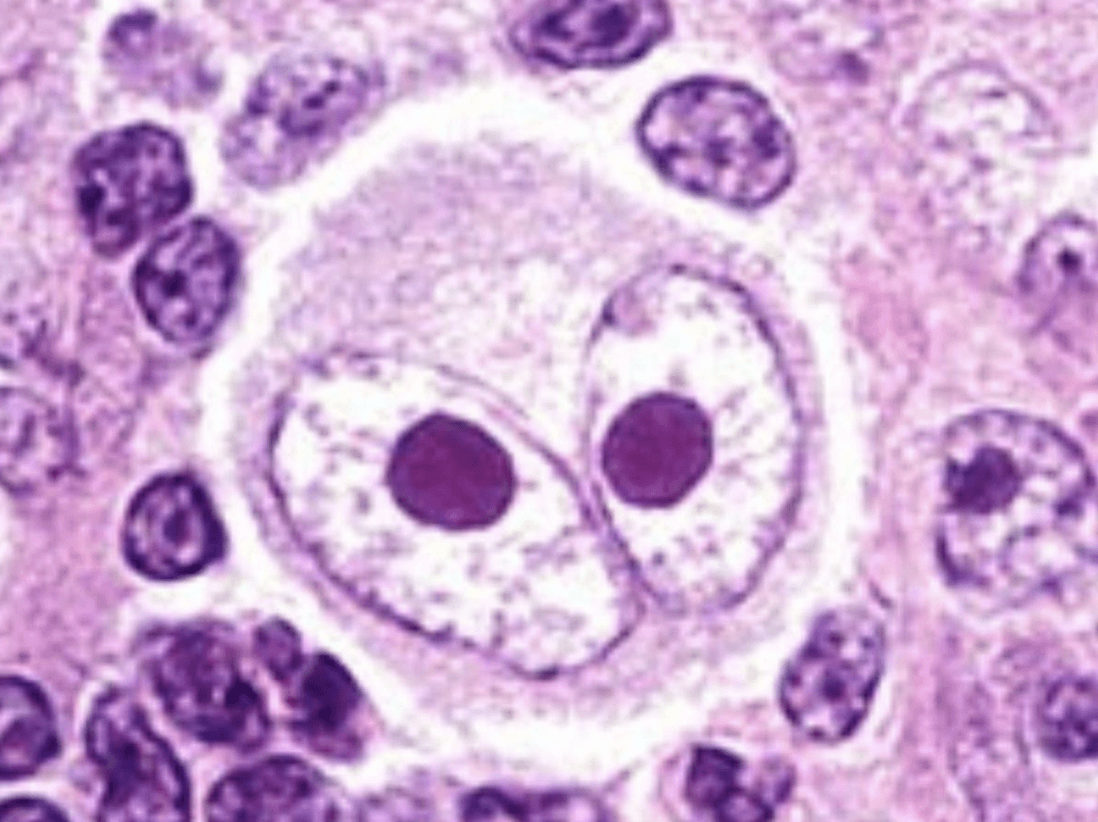
Cytomegalovirus (CMV)
CMV is very common – 90% of 80-year-olds have antibodies to the virus. Infection is usually asymptomatic; however, immunosuppressed patients can have severe manifestations ranging from nonspecific symptoms of viremia to end-stage organ disease and death. The patient in this vignette presents with nonspecific symptoms, but the biopsy shows an owl’s eye inclusion body, which is highly specific for CMV.
100
A 10 yo M over the past week comes to clinic complaining that he has been waking up sweaty. Vitals are T of 38C, HR is 85, RR is 18, BP is 110/70, O2 sats of 100%. BMI 17.5. PE is unremarkable aside from some neck lump on the right side. The cervical lymph node is biopsied, and pathology shows the following H&E stain:
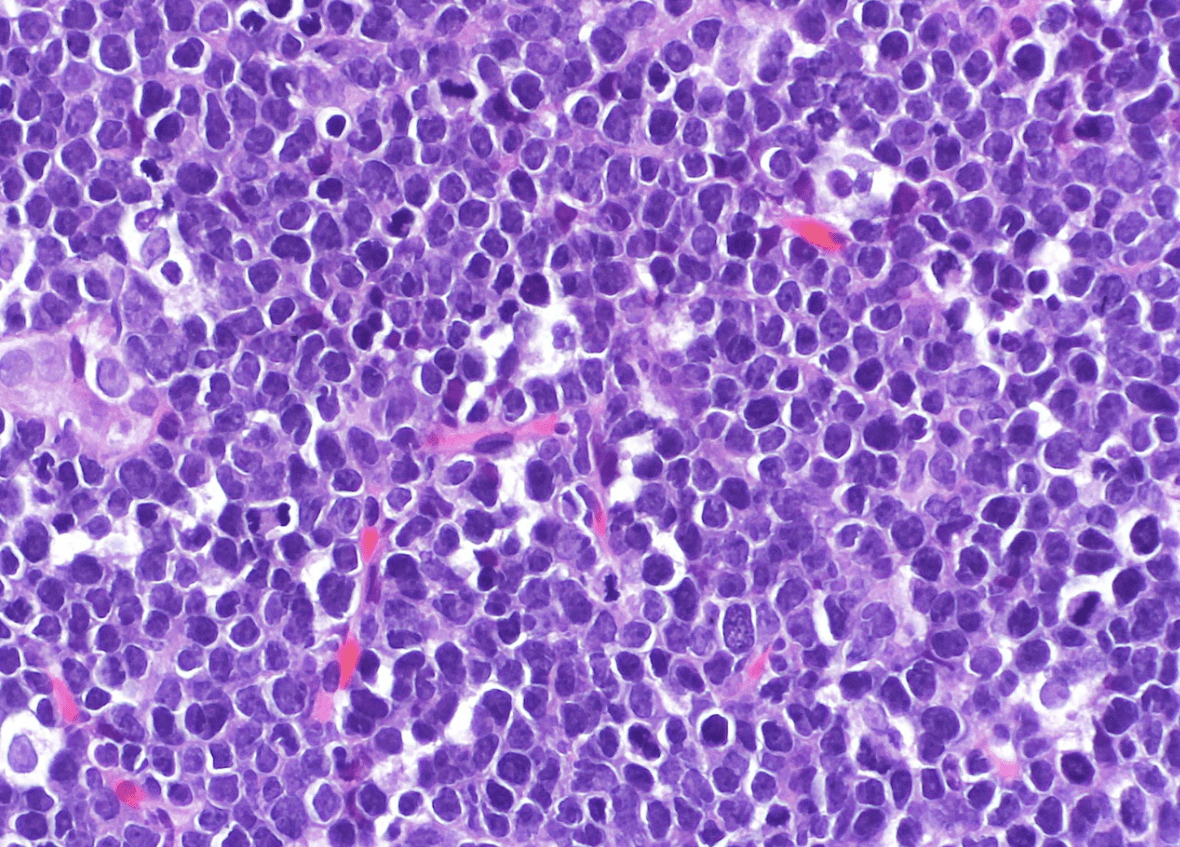
What infection is the most likely underlying cause?
Answer: EBV
Explanation: Image shows Burkitt Lymphoma, which has an association with EBV infections.
100
A 19 yo male presents to his PCP with concerns about an itchy rash. Upon closer inspection, the rash appears red and circular, with an area of clearing in the center. It is limited to the patient’s trunk. Scrapings of the rash also demonstrate hyphae on KOH wet mount. What is the causative agent of this rash?
Dermatophytes (Trichophytum, Epidermophyton, Microsporum)
Explanation: This is tinea corporis. The presentation is usually itchy ring-shaped scaly rashes. The name of the rash is based on the body site (capitis, cruis, pedis, etc.). Hyphae are the key finding on KOH mount. Sabourad agar can sometimes be used, but not often (time constraints of culture).
100
A 10-year-old patient with a history of asthma presents to the clinic with white patches in his oral cavity which can be easily scraped off. What finding would be most specific for if this fungus if it was grown at 37 degrees C on KOH prep?
Answer: Germ tubes (lateral extension of pseudohyphae)
Explanation: This is oral thrush, which is caused by candida. KOH prep can show a variety of morphologies including germ tubes, budding yeast, hyphae and pseudohyphae. However, the germ tube test is specific to identify Candida albicans.
200
A 60-year-old patient in the ICU develops thick secretions from his endotracheal tube, fever and chills. He has a past medical history of COPD, hypertension and type 2 diabetes. When you collect his sputum it looks like: 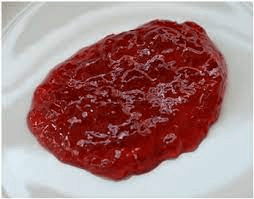
What is the virulence factor that the patient’s infection produces to cause ”currant jelly” sputum.
Polysaccharide matrix
Reasoning: This patient is suffering from nosocomial Klebsiella pneumoniae infection which classically presents with “currant jelly” sputum. The polysaccharide matrix produces a thick layer that prevents phagocytosis and causes an inflammatory response leading to necrosis in the lungs and the characteristic look of the sputum.
200
A 32-year-old arrives in clinic for a suspected UTI. She has had increased frequency of urination, back pain, increased urgency, and she has noted gross blood in her urine. An ultrasound was performed to look at her kidneys and staghorn calculi were noted. Lab work showed that the bacteria cultured was negative for lactose fermentation and negative for oxidase. What mechanism does this bacterium use that leads to struvite stones as seen in this patient?
Urease
Reasoning: The organism in this prompt is Proteus mirabilis. It classically causes UTIs as it infects the genito-urinary tract. It is known to produce large quantities of urease which hydrolyzes urea into ammonia and carbon dioxide. As it creates an alkaline environment it leads to the precipitation of phosphate, carbonate, and magnesium which leads to the characteristic struvite stones.
200
A 22 year old female patient arrives in clinic with a suspected UTI. She has an urgent, frequent need to pee, increased bladder fullness, burning while urinating, and pelvic pain. You take a urine sample and send it in for culture. The bacteria is found to be aerobic and have positive lactose fermentation. On gram stain it is revealed to be a gram-negative rod. What virulence factor does this organism have that allows it to colonize and invade the bladder?
P pili or P fimbriae adhesions
Escherichia coli is the most common cause of community acquired urinary tract infections (UPEC). It is heavily associated with ascending infections. It is a lactose fermenting bacterium. It uses adhesions to bind cells lining the bladder and upper urinary tract preventing bacterial elimination when urine is voided from the bladder.
200
You have a 23-year-old patient who contracted Mycobacterium tuberculosis when doing her emergency medicine rotation. Her X-ray showed the following:
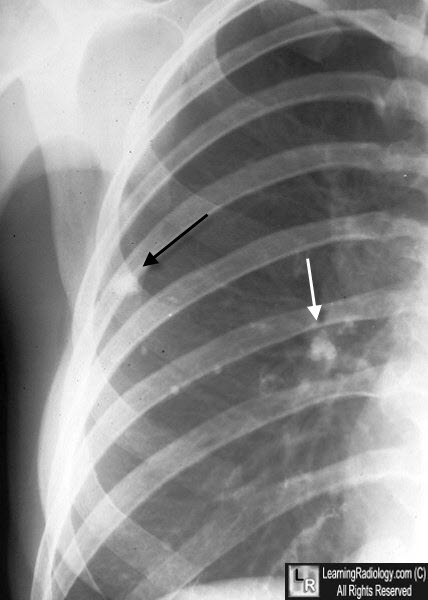
What is this classic finding of TB called?
Ghon complex
Reasoning: TB classically forms necrotizing granulomas. When there is a combination of a parenchymal granuloma and an involved hilar lymph node on the same side, the two together are called a “Ghon Complex”.
200
A 33-year-old man presents to clinic in Ohio for evaluation of fever, fatigue, and productive cough for one week. He has been involved in a work-stay program on a sheep far that specialized in exporting high-quality wool. On physical exam she has rhonchi in the left lower lobe of the lung and chest radiography confirms pneumonia diagnosis. What should she be given to treat her illness?
Answer: Doxycycline.
Explanation: The patient has a Coxiella burnetii infection which causes Q fever and culture-negative bacterial endocarditis. This is transmitted from farm animals/sheep, goat, and cattle amniotic fluid via inhalation of aerosolized spores even at low doses. Risk factors include exposure to farm animals, occupational exposure to animal products, and immunosuppression. The differential for this patient would also include tularemia which typically also presents with a maculopapular rash that may ulcerate.
200
A patient presents to ER with watery diarrhea, abdominal discomfort, and an itchy foot. The following is seen in physical exam. Patient most likely has an infection cause by which parasite?

Strongyloides stercoralis
Stronyloides presents in immunocompetent patient with GI symptoms like diarrhea, constipation, and abdominal discomfort. They also get larva currens (urticaria due to migration of larvae) rash as a key finding (image). Transmitted via contact and penetration of unbroken skin. Immunocompromised hosts can also get pulmonary ssx (pneumonia) due to life cycle in the lungs, hyperinfection, and subsequent sepsis from enteric microbes in the gut.
200
A 23 yo female presents with vaginal discharge and pruritus. She describes the color of the discharge as a green yellow. She has one male partner of 3 months. On pelvic exam, the cervix appears as showed. A molecular test confirms the infection. What is the next best step?
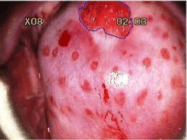
Answer: Metronidazole for patient and her partner.
Explanation: This is trichomonas. Symptoms and "strawberry cervix" support diagnosis. Rx is with metronidazole, and partner should be treated empirically to prevent re-infection.
200
A 36-year-old woman presents to her primary care physician with complaints of painful recurrent sores that appear on her lower lip. She shows this recent picture to her physician. Which type of cell does this pathogen reside in during its latent phase?

Sensory neurons (trigeminal ganglion)
This patient is infected with herpes simplex virus 1 (HSV-1). The alpha sub-family of human herpesviruses includes HSV-1, HSV-2, and varicella-zoster virus (VZV). Viruses of the alpha sub-family reside in sensory neurons in their latent phase (trigeminal ganglion for HSV-1), and cause pain in the local skin and mucous membranes during reactivation.
200
55 yo M comes to clinic with worsening fatigue and a cough. Pertinent PMH includes HIV, tobacco use, and depression. Most recent CD4+ count was 2500. Upon further questioning, patient hasn’t refilled any medications in the past couple months after losing insurance. On exam, patient has white patches on roof of mouth. CXR shows diffuse ground glass opacities. In addition to regular HAART, what else could be added to prevent similar infections in the future?
Answer: Bactrim prophylaxis
Explanation: Question most likely depicting PJP PNA as a consquence of going off his medications (CD4 count no longer accurate). In addition to starting meds, Bactrim prophylaxis should be initiated until CD4 counts recover.
200
A 53 yo female presents to the ER with fever, cough, and chest pain that worsens with normal breathing. Upon getting an X-ray, nodular infiltrates are noted. When taking the patient’s history, the ER physician notes that she had recently traveled to Arizona to visit her sister. Her medication list includes etanercept, ibuprofen, and propanolol. What is the most likely agent responsible for the patient’s illness?
Coccidioides imitis
Explanation: Pt is presenting with pulmonary signs of a possible fungal infection. Nodular infiltrates and history of immunosuppression (etanercept) also raises this on the differential. History of travel to Southwest US would raise suspicion for Coccidioides.
Other important info: This fungus forms spherules in the tissue as part of its pathogenesis, which can help differentiate it from other fungi.
200
A patient’s chest X-ray (with a past history of TB) reveals a round mass with the opacity of that of a soft-tissue mass. Upon culturing the fungus you notice septate hyphae with acute angle branching. What type of fungal infection does this patient have?
Answer: Aspergilloma/Fungal Ball
Explanation: Aspergillus has a variety of presentations. Fungal balls occur when aspergillus colonize an already existing cavity/abscess (such as from TB), and can be asx or lead to typical pulmonary symptoms.
300
An 18-year-old male arrives to the emergency room with shortness of breath, extreme fatigue, productive cough that he reports steadily worsened over the past 12 hours. He has a past medical history of cystic fibrosis and several episodes of pneumonia. A sputum culture is ordered that grows green with a metallic sheen on Mueller-Hinton agar. The laboratory technician notes that the colonies smell like grapes. What is the main endotoxin that this organism produces that trigger cytokine pathways in its hosts?
Lipopolysaccharide
The patient in this scenario is infected with Pseudomonas aeruginosa which commonly is a cause of pneumonia in patients that are on ventilators and patients with neutropenia, burns, or cystic fibrosis. This organism classically grows a green/blue color that has a metallic sheen and these colonies smell “grape-like” or “corn tortilla-like". These are gram-negative organisms and have many molecules that contribute to pathogenesis, but in this case, lipopolysaccharide is an endotoxin that resists host defenses and often triggers cytokine pathways. Not to be confused with Exotoxin A which is responsible for disrupting protein synthesis by blocking peptide elongation.
300
A 68 y.o. male with a past medical history of asthma and a 40-pack year smoking history presents to clinic with cough, fatigue, fever, and chills. You obtain a gram stain that shows:
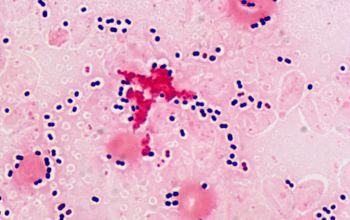
What is the main virulence factor produced by this organism protects it from host immunity?
Polysaccharide capsule
Reasoning: The organism shown by the gram stain is Streptococcus pneumoniae which is a gram-positive bacterium that is typically described as “lancet shaped” and found in diplococci. The polysaccharide capsule it produces makes it difficult for macrophages to phagocytose the organism. Streptococcus pneumoniae is a common cause of community acquired pneumonia, adult meningitis, sinusitis, otitis media, and bacteremia.
300
A 34-year-old woman comes to clinic complaining of joint pain in her knees, elbows and wrists. She tells you that she arrived in the U.S. three years ago from El Salvador and when asked tells you that she remembers having some throat infections as a child. Upon examination, she has a fever of 100 F and a systolic heart murmur on auscultation. What is the likely mechanism causing this woman’s symptoms?
Cross-reactive antibodies to Group A strep
This patient likely has rheumatic fever which is characterized by arthritis, fever, and heart failure but can also present with fatigue, and chorea (uncontrollable movements). Rheumatic fever develops when strep pharyngitis or scarlet fever infections are not treated, and the immune system develops cross-reactive antibodies that target healthy tissue. While it is not a common illness in the US, it remains relatively common in other countries.
300
A 55-year-old patient arrives to the emergency room with severe leg weakness. He has a past medical history of hypertension, asthma and untreated Mycobacterium tuberculosis infection. You perform an MRI of the spine and find:
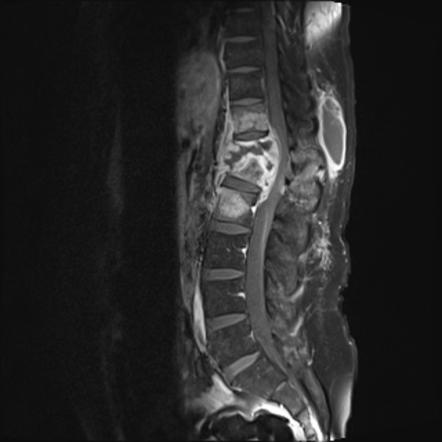
What complication of TB has this patient developed?
Pott’s Disease
Reasoning: While TB is classically a pulmonary disease, it has several extra-pulmonary symptoms including bone infection, especially in the spine. This can lead to bony destruction as what is depicted above.
300
A 25-year-old man presents to the urgent care clinic for diarrhea. His symptoms began approximately 2 days ago and are associated with abdominal pain, malaise, and fatigue. He denies the presence of blood or pus in the stool. He states that he returned from his trip to Peru one week ago. Physical examination is notable for mild abdominal tenderness upon palpation, but there is no hepatosplenomegaly or skin changes. What virulence factors from this pathogen are the cause of the patient’s watery diarrhea?
Answer: Heat-stable enterotoxin and heat labile enterotoxin.
Explanation: This patient with recent travel history and non-blood diarrhea without hepatosplenomegaly is experiences enterotoxigenic ETEC which causes traveler’s diarrhea. Treatment for this patient is supportive care.
300
This organism uses snails as an intermediate host in its life cycle. Once they leave the snail, they swim towards the light in order to find a human within 8 hours. What parasite is this?
Schistosoma mansoni
This parasite has its eggs deposited in water sources. From here, the larvae hatch and migrate to snails where they develop into cercariae. After leaving the snails they must find a human host via chemotaxis in order to survive. If successful, they enter the unbroken skin and a male and female mate in the liver, before traveling to the intestines to deposit their eggs. Illness includes Katayama fever (fever, flu-like ssx, swollen lymph nodes, hepatosplenomegaly; hypersensitivity to antigens), granulomas, portal HTN from fibrosis, and GI hemorrhage.
300
A 26 yo male presents to clinic with periorbital edema. He states that this appeared overnight with no other symptoms outside of some intermittent chest pain. He has no PMH and takes no medications. Physical exam shows the following:

Based on the category and presentation, name 1 of the 3 chronic complications of this disease.
Answer: Achalasia, megacolon, dilated cardiomyopahy.
Explanation: This is Chagas Disease, cased by trypanomsoma cruzii. Acute disease occurs after the "kissing bug" bites and rubs its feces into the wound, presenting with Romana's sign (as pictured). Other acute presentations can include myocarditis and meningoencephalitis. To help remember the chronic conditions, they are all similar in that their organ structures are dilated.
300
A 3-month-old infant presents to the emergency department with intermittent apnea. His parents state that he started attending a new daycare three weeks ago and has been showing signs of lethargy and poor appetite for the past four days. Which pathogen is most likely responsible for this infant’s illness?
Respiratory syncytial virus (RSV)
Explanation: Although RSV can infect people of any age, it is most common and often most severe in infants < 6 months of age. The classic presentation of RSV in infants includes poor appetite, irritability, and lethargy. In severe cases, it can cause apnea. Another clue for RSV in this vignette is the fact that the infant started at a new daycare recently – RSV is transmitted through direct contact of mucous membranes with infectious respiratory droplets.
300
35-year-old female presents to ER with worsening fatigue and abdominal pain for the past few months. More recently, she noticed her urine becoming darker despite trying to stay hydrated. Vitals are stable. U/S shows hepatomegaly. ALT is 3500. AST is 2000. Upon further history taking, she states that she has had three new sexual partners in the last 4 months. Labs are drawn to workup the patient. A hepatitis serology work-up would most likely show?
Answer: HBsAg+, Anti-HBc+, HBeAg+
Explanation: Symptoms and given labs point to hepatitis. HBV can be transmitted sexually or parenterally. Additionally, these symptoms indicate an acute infection, which would correlate with the above lab serologies.
300
A 34 yo HIV positive male with a CD4 count <100 presents to clinic concerned about new dysphagia. Most of the physical is normal, except for white plaques noted in the patient's oral cavity, which are removed and bleed upon scraping. After being referred for swallowing difficulties, endoscopy shows similar white plaques along the esophagus as well. Upon visualization, yeast and psuedohyphae can be visualized. What is the causative agent of this patient’s dysphagia?
Candida albicans
Reasoning: white plaques in the oral cavity that you can scrape off are a key physical finding. Additionally, esophagitis is another clinical presentation of candida infections which is usually confirmed with endoscopy. Yeast and pseudohyphae are the typical pathological description of candida species. Another clue is that the patient has a CD4 <100 (level associated with infections like esophageal candidiasis)
300
A 7 yo boy presents with hair loss and a pruritic lesion of the scalp. On physical examination, you notice the following: 
What is the most appropriate treatment?
Answer: Griseofulvin (or Terbinafine)
Explanation: This is tinea capitis, a dermatophyte infection. While many can be treated with topical azoles, ringworm of the scalp requires oral medications for longer periods to adequately treat the infection.
400
A 23 y.o. male presents to the emergency room with a 24-hour history of fever, chills, abdominal pain, vomiting and confusion. His mother tells you that he had surgery to remove his gallbladder last week. The patient has a 102 F fever and a BP of 80/50. Upon physical examination, the patient has a diffuse, red, macular rash resembling a sunburn with peeling skin shown in the picture below: 
What toxin is most likely responsible for this patient’s symptoms?
Toxic Shock Syndrome Toxin 1 (TSST1)
Reasoning: Staphylococcus toxic shock syndrome is characterized by rapid onset of fever, rash, hypotension and multiorgan involvement. While classically associated with tampon use, it can also occur with recent surgery, or recent cellulitis. The picture depicts scalded skin syndrome which is induced by toxin damage to the skin causing blisters that frequently rupture. While Group A strep can also cause toxic shock syndrome, the “sunburn like rash” is only occasionally seen in Group A strep toxic shock syndrome.
400
You have a 40-year-old patient in clinic who has recently returned from Mexico with a weeklong history of non-bloody diarrhea and abdominal pain. He reports only drinking bottled water however he does recall eating fresh fruits and vegetables while on the beach. He denies fever and chills. Which of the toxins the organism produces binds to the intestinal receptor guanylyl cyclase C?
Heat stable enterotoxin
This patient likely received enterotoxigenic E coli from eating fruits and vegetables washed with contaminated water. This is likely as he has recently traveled abroad. Enterotoxigenic E coli produces 2 enterotoxins the first one is heat stable enterotoxin which binds to guanylyl cyclase receptor causing hypersecretion of fluids and inhibition of fluid absorption. The second is heat labile enterotoxin which interacts with a membrane protein (Gs) that upregulates adenylyl cyclase to increase cAMP, and thus Cl- secretion.
400
You have a patient in the ICU who is being treated for S. aureus bacteremia with clindamycin. After 3 days of therapy, the patient develops abdominal pain, distention and severe diarrhea. A glutamate dehydrogenase antigen test returns positive. What medication would you give to treat this patient’s infection?
Oral vancomycin
Reasoning: This patient developed severe diarrhea in a hospital setting after receiving antibiotics (particularly clindamycin) is a classic patient presentation of Clostridioides difficile. A positive glutamate dehydrogenase antigen test is a highly sensitive test that detects the presence of C. difficile but does not discern toxigenic vs. non-toxigenic strains. Given the patient’s symptoms and history though, you would treat by discontinuing clindamycin, give supportive care and oral vancomycin.
400
A 45-year-old male arrives in clinic with a chief complaint of skin lesions. Upon physical exam you find a sporotrichoid pattern of lesions like so: 
You order microbiological testing and find acid fast bacteria. What is the most likely cause of this patient's infection?
Mycobacterium marinum
Reasoning: Mycobacterium marinum is an acid-fast organism that commonly follow minor trauma or inadvertent inoculation that led to “fish tank granulomas” as shown in the picture above. The organism produces specific membrane lipids that recruit permissive macrophages to the site of infection which allow the bacteria to spread.
400
A farmer from Chile presents to your local clinic with daily fevers and fatigue. He supports his family by selling woold and providing unpasteurized milk for drinking and making cheese. For the past month, he has had general malaise, daily fevers and some nausea and vomiting. On physical exam he has a fever of 100 F, but is otherwise normal. What is the causative organism?
Answer: Brucella genus (likely Brucella melitensis)
Explanation: Brucella is a facultative intracellular gram-negative zoonotic coccobacillus. Transmission often occurs via ingestion of contaminated foods. It typically presents as an undulant fever. This bacteria is endemic to Mediterranean countries and South America and is the most common bacterial zoonosis. Risk factors include ingestion of unpasteurized dairy products. Symptoms include undulant fever, malaise, headaches, nausea and vomiting, and arthritis. Also on the differential is Q fever, but this presents with pneumonia symptoms. Treatment is doxycycline or aminoglycosides.
400
A 24-yo female who recently immigrated from Nigeria presents to your clinic for fever, malaise, and myalgia. Upon ordering a CBC, you also find that she has a hemoglobin of 10.1. A giemsa-stained blood smear is completed, and shows the following:
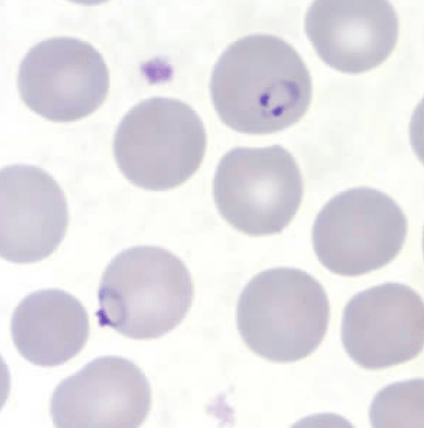
Further analysis identifies the organism as P. falciparum. Based on this information, what fever cycle would you expect the patient to be experiencing?
malignant tertian (48-hour) fever.
Malaria generally presents with ssx of fever, malaise, myalgia, headache, and mild anemia. The blood smear also shows the rings they form in RBCs as part of their life cycle. Giemsa-stained smears can be used to help in ID'ing the species.
P. falciparum has malignant tertian fever as an individual characteristic where if the fever is recurring, it occurs every second day. P. falciparum also causes more severe symptoms (cerebral malaria, placental malaria, blackwater fever) due to its later stages causing sequestration of RBCs to the endothelial lining.
400
A 38-year-old recent immigrant from Brazil comes into the clinic with a 4-month history of painless, ulcerated plaques on his left arm. He denies fever, fatigue, or weight loss. Physical exam revealed ulcers of varying sizes on the left arm, covered with a yellow-white fibrinous material. There are no mucosal lesions, pallor, lymphadenopathy, or hepatosplenomegaly. A complete blood count and liver function test were within normal limits. HIV serology, AFB for lepra bacilli, and serum VDRL were all negative. Histopathology shows the following:
What is the disease vector?
Answer: Sandfly
Explanation: This is cutaneous leishmaniasis. Question gives history of individual from South America. Presentation includes painless, ulcerated lesions with no other symptoms to indicate visceral involvement. Other workup is negative. Histopathology image shows an amastigote, which is a macrophage with the replicating parasite.
400
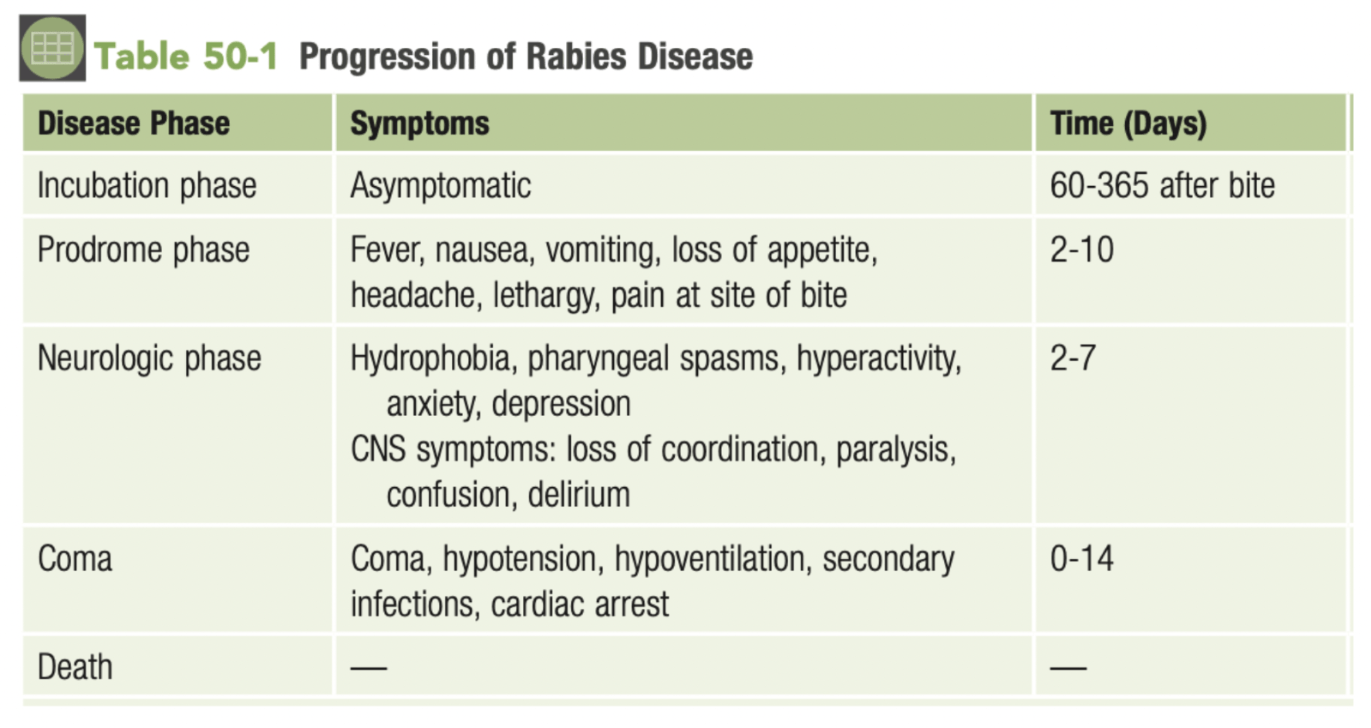
A 24-year-old woman was bitten by a stray dog during a trip to Madagascar. Three months later, her roommate brings her to the emergency department. She presents with hydrophobia, pharyngeal spasms, lack of coordination, and confusion. Based on her clinical presentation and travel history, an infectious disease physician diagnoses her with rabies. Considering the natural course of rabies, which disease stage was this patient in when she presented to the emergency department?
Neurologic phase
There are four phases of rabies disease: incubation, prodrome, neurologic, coma, and death. Summaries of each phase are included in the image. The patient in this vignette is in the neurologic phase due to her distinct symptoms of hydrophobia, pharyngeal spasm, lack of coordination, and confusion.
400
A 6 mo F child is brought into clinic for a rash. Rash started 3 days ago along with a fever. No birth history, born vaginally. Vitals are as follows: patient has a fever in clinic, otherwise vitals are stable. On exam, patient is fussy, has a few vesicles on roof of mouth, and has some skin peeling on her feet. Labs are positive for elevated WBC count of 13k. What is the most likely cause of the rash?
Answer: Cocksackie A Virus
Explanation: This is hand foot and mouth disease. Presents with herpangina (vesicles in mouth), as well as a maculopapular or blistering rash of the extremities.
400
A 44-yo woman present to clinic with recent concerns about changes in skin coloration. During her physical exam, you note areas of hyperpigmentation which also fluoresce under Wood’s Lamp. Upon taking skin scrapings, what would you expect to see on a KOH prep?
Clusters of yeast cells and long hyphae (“spaghetti and meatballs”)
Explanation: Hyperpigmentation or hypopigmentation (tinea versicolor) is the typical presentation for malassezia furfur (neonates and those on TPN can get funginemia). Additionally, the patches fluorescing under wood’s lamp is a key point in the physical (dermatophytes can also fluoresce). “Spaghetti and meatball’ is the typical described appearance due to the mix of yeast cells and longer hyphae on KOH wet mount.
400
A 53-yo woman presents with a skin infection of the nose. The skin in the area is necrotic as pictured below. No other symptoms noted. She has a history of T2DM. KOH prep shows right-angle branching of hyphae. What is the most appropriate next step in management?

Answer: Debridement
Explanation: This woman has a mucor fungal infection. These infections need surgical debridement to help with infection control and prevention of further spread, along with an aggressive antifungal regimen.
500
A 65-year-old patient on a ventilator due to complications from bacterial pneumonia developed thick secretions from his endotracheal tube. He has been diagnosed with stage II renal cell carcinoma and has been on a chemotherapy regiment for the past 4 months. A sample from the endotracheal tube is sent to the lab for an initial gram stain and culture. The lab report shows that the organism is a gram-negative rod with uniform staining that is non-lactose fermenting, and oxidase negative. What is the likely identity of this organism?
Stenotrophomonas maltophilia
Reasoning: Stenotrophomonas maltophilia typically causes a wide range of opportunistic infections in hosts and fits the lab characteristics presented. Pseudomonas aeruginosa is oxidase positive. Acinetrobacter baumannii are coccobacilli typically found as single cells or in pairs.
500
A 55-year-old woman has come into clinic today for concerns about her peripherally inserted central catheter (PICC) line. The patient receives regular doses of chemotherapy to treat her medullary thyroid cancer. Upon examination, the area around the PICC line insertion site is erythematous, hot to the touch, and has purulent exudate. You collect a sample from the line and send it to the medical microbiology lab for analysis. Labs reveal large, gram-negative coccobacilli arranged in pairs. It does not ferment lactose and is oxidase negative. What is the likely identity of this organism?
Acinetrobacter baumannii
Acinetrobacter baumannii fits the description above and is typically associated with ventilator-associated pneumonia, central line associated infections, and skin and soft tissue infections. Stenotrophomonas maltophilia is a gram-negative rod. Pseudomonas aeruginosa is oxidase positive.
500
What are two common causes of hematogenous urinary tract infections?
Staphylococcus aureus bacteremia and Mycobacterium tuberculosis.
Reasoning: there are two major mechanisms for urinary tract infections. Ascending urinary tract infections are the most common and there are hematogenous urinary tract infections.
500
You have a patient who has recently immigrated from Nepal, who comes into clinic with very dry, scaly, hypopigmented patches with very sharply defined edges:
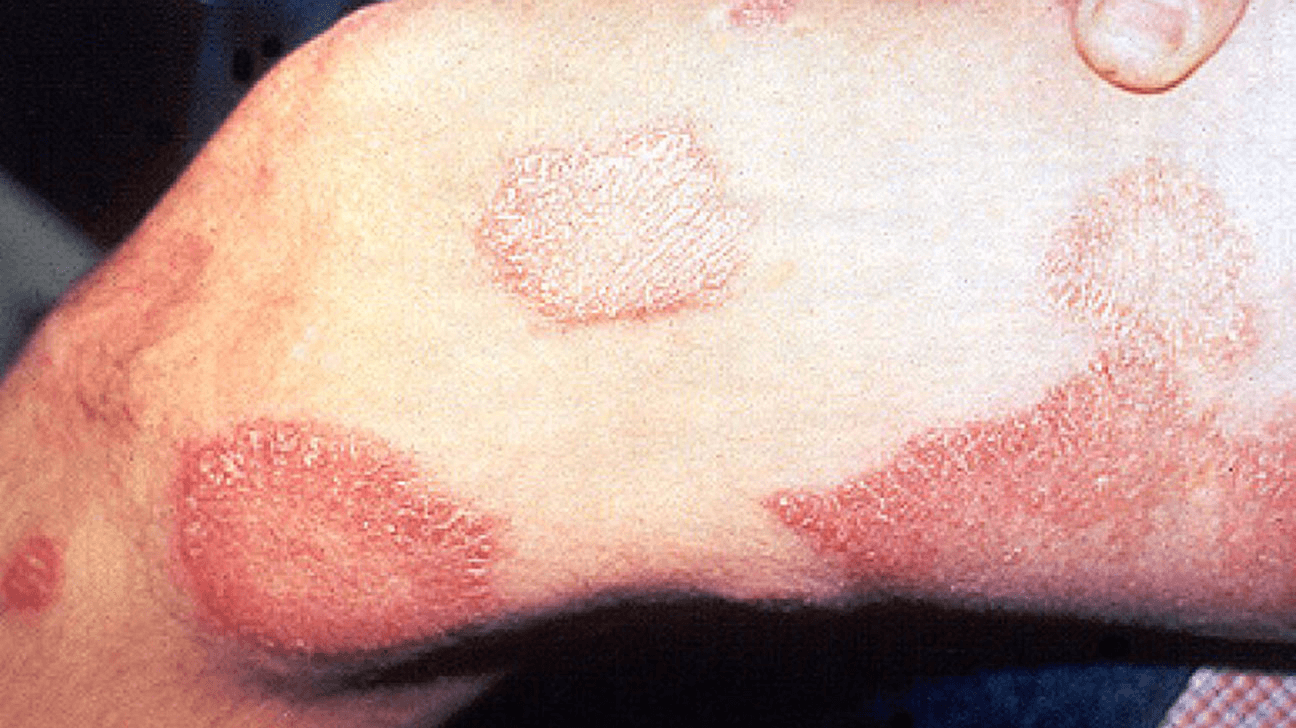
Upon palpation, the plaques are anesthetic. A biopsy is performed on the plaques revealing well-formed granulomas, and a few acid-fast bacteria. What is the most likely cause of this person's lesions?
Mycobacterium leprae
Reasoning: This patient is likely suffering from tuberculoid leprosy. It is classically characterized by anesthetic macules or plaques, enlarged peripheral nerves near the skin lesions, and histology with well-formed granulomas with few acid-fast bacteria.
500
A 23-year-old woman presents to the emergency department with fever, chills, and water diarrhea. Her symptoms began approximately 1 day after menstruation began. Her temperature is 102 F, blood pressure is 75/50 mmHg, pulse is 125/min, and respirations are 20/min. Physical examination is notable for a diffuse erythematous rash and desquamation of the palms and souls. What is the best treatment for this patient.
Answer: Source control (remove tampon)
Explanation: This patient is experiencing toxic shock syndrome, likely due to leaning a tampon in place for a long period of time. This stimulates bacteria (likely Staphylococcus aureus in this case) to produce toxins such as toxic shock syndrome toxin-1 which can cross the vaginal mucosa and cross link the beta region of the T cell receptor to MHC class II. This leads to an overwhelming release of cytokines. Treatment is first and foremost source control. Antibiotics can also be given, but this will not cure this disease, only help remove any additional bacteria producing the toxin.
500
A 33-yo HIV+ female presents to their CP with a two-month history of bloody diarrhea for 2 weeks and abdominal tenderness. Bedside U/S finds a hepatic cyst on the right lobe. What would you expect to see on stool microscopy?
Trophozoites containing RBCs and charcot-leyden crystals
The suspected organism here is Entamoeba histolytica. Patient presentation with long-standing bloody diarrhea, abdominal tenderness, and hepatic involvement would raise suspicion for this parasite. Patient being immunocompromised is also a risk factor. Since the patient has intestinal disease, a stool microscopy would show trophozoites with 2+ RBCs and charcot-leyden crystals. Another possible finding would be a blue staining nucleus with trichrome stain.
500
A 35-year-old man presents to the emergency department for seizures. Prior to developing seizures, he complained of a headache and was progressively confused. He eventually became nauseous and had multiple episodes of emesis. He recently emigrated from Mexico to the United States and did not have a seizure history. Imaging shows:
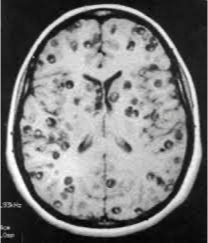
What would most likely be found on stool O&P for this diagnosis?
Answer: Proglottids
Explanation: This vignette is describing neurocysticercosis. Presents with seizures and other neuro complaints, with imaging showing parenchymal cysts and calcifications. History of emigration also supportive. Transmitted via contaminated meat products and treated with praziquantel.
500
A 74-year-old man of Swedish descent reports receiving countless blood transfusions to treat his hemophilia. This history includes hundreds of transfusions received before 1992, when blood donations began to be screened for all variants of HIV. Despite his very high risk of HIV exposure, he never became infected with the virus. Which homozygous mutation is most likely contributing to this patient’s inability to become infected with HIV?
CCR5 gene deletion
The CCR5 receptor is a protein expressed on the surface of leukocytes and is used by HIV to enter and infect the cells. Up to 13% of individuals of Northern European descent have a deletion of the CCR5 receptor gene, which codes for a mutant CCR5 receptor that fails to reach the cell surface. Homozygotes for this deletion do not become infected with HIV despite multiple exposures, and heterozygotes, if infected, have a very slow course of disease. The patient in this vignette is likely to be a homozygote for this mutation.
500
A 22yo male presents to clinic with new onset weakness and speech difficulties. He has a history of HIV with sporadic use of HAART. After a thorough neurologic exam, a head CT is ordered and shows the following:

What cell type is infected by this virus?
Answer: Oligodendrocyte
Explanation: This is progressive multifocal leukoencephalopathy from JC virus. Condition usually associated with immunocompromised status. White matter lesions usually lead to motor and speech related issues.
500
A 70 yo male presents to clinic with the following skin findings. When asked about his recent activities, he tells you that he has been working in his garden with his wife. Based on these findings, what histopath would you expect to see for the most likely causative organism?

Cigar shaped yeast
Explanation: This is sporotrichosis cause by Sporothrix schenckii. It is a nodular, ulcerative skin finding that follows the lymphatics, and is typically associated with gardeners (source is soil and decaying plant material; needs direct inoculation like rose thorns)
500
A 17yo male presents to clinic with flu-like symptoms. He has no PMH, but did recently immigrate from Central America. On physical exam, he has cervical and axillary lymphadenopathy, as well as multiple mucocutaneous ulcers. A scraping from one of the lesions is taken, and shows the following on KOH prep:
What is the causative organism?
Answer: Paracoccidioides brasiliensis
Explanation: Usually presents in individuals from Central or South America with a history of outdoor work. Presentation includes flu-like symptoms or those similar to PNA, with lymphadenopathy and mucocutaneous lesions on exam. KOH prep image is very specific.
600
A 19-year-old male arrives at the emergency room with trismus, difficulty breathing and muscles spasms. His mother found him unable to move two hours prior when coming over to visit. Physical exam shows a deep puncture wound on the bottom of his foot. What neurotransmitters are blocked by the toxin produced by this patient’s infection?
GABA and glycine
Reasoning: Trismus (“lock jaw”) is a classic system of generalized Clostridium tetani infection which causes spastic paralysis. The toxin that the organism produces is Tetanospasmin which blocks the release of inhibitory neurotransmitters GABA and glycine.
600
A 6-month-old child arrives to the emergency department with constipation, poor feeding, hypotonia and a weak cry. The child had been healthy up to this point with no complications during birth. The mother recalls the child had been eating normally and had recently filmed a video of her child trying honey for the first time. What is the gold standard for diagnosis of the organism responsible for the infant’s symptoms?
Mouse bioassay
Reasoning: The infant is suffering from infection of food botulism caused by Clostridium botulinum. In infants, it is classically caused by ingestion of spores (particularly through consumption of raw honey). In adults it is more associated with wound botulism. In the laboratory, conventional health diagnosis requires demonstration of the toxin for which mouse bioassay is the gold standard.
600
A 65 y.o. woman arrives at the hospital with worsening shortness of breath, fever, chills. Upon admission she was diagnosed with COVID-19 and after a week, required ventilator assistance to breathe. After being placed on a ventilator, purulent tracheal discharge was sent for a gram stain revealing gram-positive cocci in clusters. What other clinical manifestations would you expect to see in this patient?
Secondary bacteremia with subsequent seeding to the kidney, bones, or heart.
Reasoning: The most common causes of ventilator associated pneumonia are Pseudomonas aeruginosa, Escherichia coli, Klebsiella pneumoniae, Acinetobacter, and Staphylococcus aureus. The Gram stain reveals gram-positive cocci in clusters, which is characteristic of S. aureus. S. aureus can colonize the respiratory tract leading to pneumonia, especially when patients are already ill. Bacteremia is a common complication.
600
An 80-year-old woman presents to clinic with A four-year history of productive cough, and intermittent dyspnea with exertion. She has been treated with azithromycin for presumed community acquired pneumonia, and her symptoms had initially improved. Subsequently she experienced discrete recurrent episodes of “bronchitis” with productive cough. She reported a 10-year pack smoking history in the past. Her past medical history includes asthma, atrial fibrillation, GERD, osteopenia, and hyperthyroidism. Her sputum culture returned positive for an acid fast bacteria, but her TB test returned normal. CT imaging was performed and it showed:
What is the most likely cause of her symptoms?
MAC
This woman likely suffers from MAC pulmonary disease. This patient fits the pattern of lady Windermere syndrome, which is typically seen in elderly white woman who chronically suppressed the normal cough reflex.
600
A 43-yo male presents with fatigue, low grade fever, and heart murmur, and the following painless lesions pictured below. Blood cultures return positive for S. bovis. After appropriate antimicrobial treatment, what is recommended to do in the outpatient setting?

Answer: Colonoscopy
Explanation: S. bovis bacteremia or endocarditis are associated with colonic malignancies. Current IDSA and AHA guidelines recommend follow-up colonoscopy to screen for malignancy. Other infections associated with colon malignancy include C. septicum and S. gallolyticus.
600
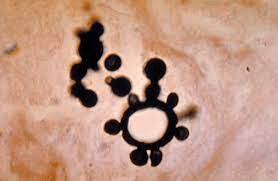
A 27-yo male from Ohio presents to the clinic with fever, weakness, and exercise intolerance. He tells you this is abnormal for him, as he usually goes on 5 mile hikes each weekend on wooded trail near his home. Physical exam demonstrates a male who appears with slight jaundice. A thin blood smear is ordered an demonstrates the following:
How do you suspect the causative organism was transmitted in this case (be specific)?
Ixodes scapularis (tick bite)
The causative organism of the patient's symptoms is Babesia microti. Patients usually present with non-specific ssx and fever. This organism can also cause anemia, which lends to the ssx profile as well (weakness, exercise intolerance). The blood smear shows a key finding (maltese cross). This organism can be transmitted via tick bites (ixodes scapularis is the vector; white tailed deer and white footed mouse are the reservoirs) or blood transfusions.
600
A 55-year-old woman comes to the emergency department complaining of abdominal pain. She states that she has suffered intermittent nausea for 2 years. Then 3 months ago she began to notice right-sided abdominal pain. She denies vomiting, diarrhea, or constipation. She has not been to a doctor in 3 years since she moved from Peru. She has had no surgeries. She takes no medications. On physical examination, there is moderate right upper quadrant tenderness. CT shows the following:
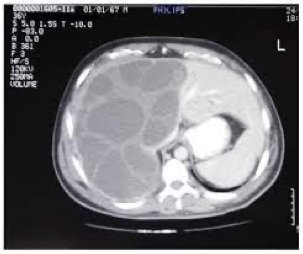
What is the most likely possibly complicated with percutaneous drainage?
Answer: Anaphylaxis
Explanation: This vignette is describing a hydatid cyst secondary to echinococcus. The present with RUQ and nausea, and possible respiratory ssx if lung involvement. The largest precaution with removal is that rupture of the cyst can result in an anaphylactic reaction.
600
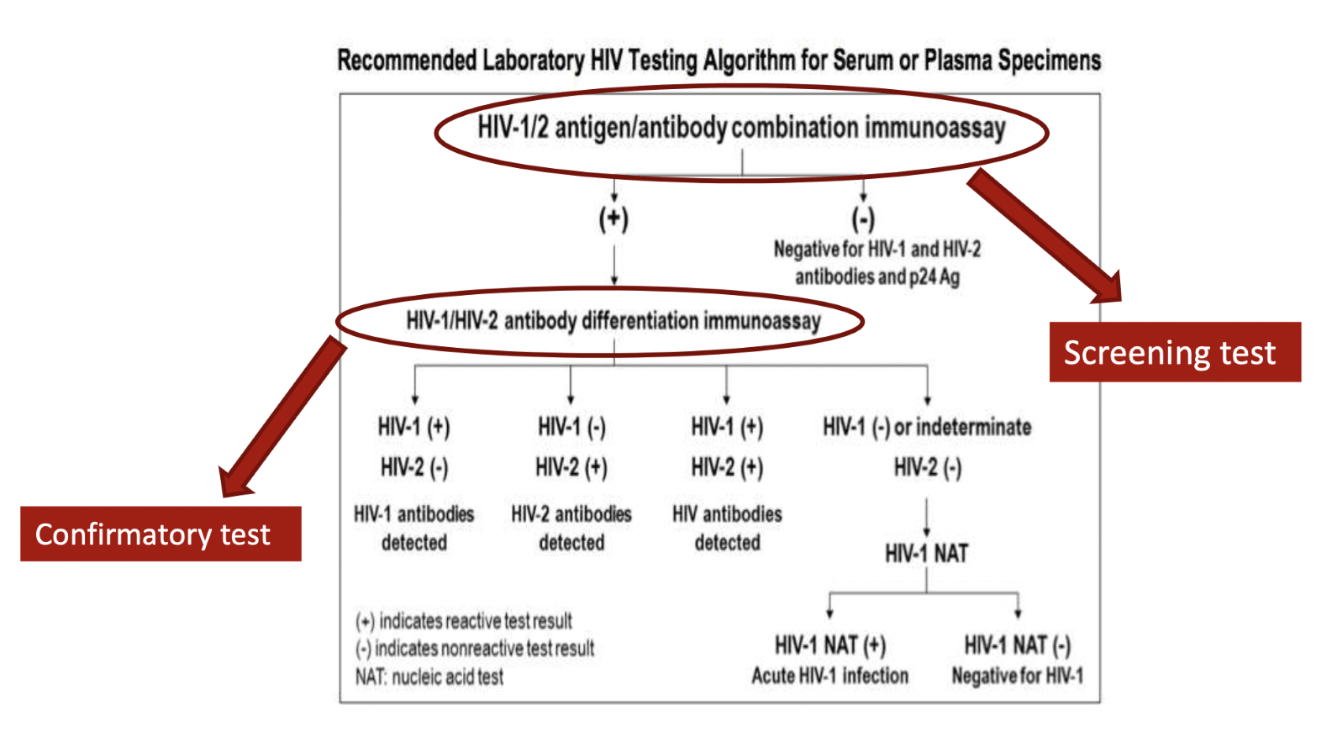
An 18-year-old man tested positive for HIV on an HIV 1/2 antigen/antibody combination immunoassay (screening test). His physician explains that an HIV diagnosis cannot be made based on the screening test alone, and that a confirmatory test must be ordered to make a definitive diagnosis. What is the confirmatory test for HIV testing?
HIV-1/HIV-2 antibody differentiation immunoassay
The HIV screening test includes antibodies for HIV-1 and HIV-2, as well as the p24 antigen. Detection of any of these components yields a positive result. To make a definitive diagnosis of HIV, an antibody differentiation immunoassay must be performed. This is a confirmatory test and yields information about whether the patient is infected with HIV-1, HIV-2, both viruses, or neither.
600
An infant presents to clinic with concerns about possible hearing loss. Birth history included a spontaneous vaginal delivery with no complications. Mom started having prenatal visits in the third trimester. On exam, the infant has various purpura and jaundice apparent, along with hepatomegaly. Eye exam shows cataracts. What would have most likely prevented this infants presentation?
Answer: MMR vaccination for mom prior to pregnancy
Explanation: This is congenital rubella. All congenital torch infections have some shared features (jaundice, blueberry muffin rash, hepatosplenomegaly). Cataracts and hearing loss is specific for Rubella. However, the most common congenital cause for hearing loss is CMV.
600
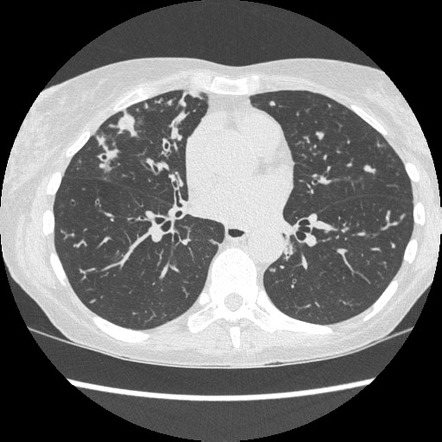
A 23 yo male presents to the ER with fatigue, fever, cough, and shortness of breath. He has a history of lupus for which he takes prednisone. A chest CT is performed shows the following. What marker could you test for in the blood for diagnosis of this infectious organism?
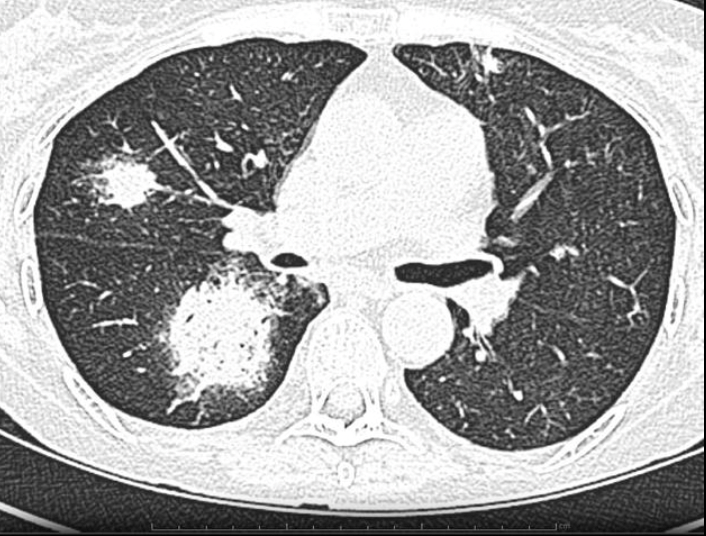
Galactomannan
Explanation: This is pneumonia caused by aspergillus. The patient presentation, history of steroid use (for lupus), and characteristic imaging on chest CT (halo sign) can all lend to this on the differential. Galactomannan is a polysaccharide antigen in the cell walls of aspergillus that can be released into the bloodstream during infection. It is very specific for aspergillus.
Other key findings: septate, acute-angle branching histopath; risk factor of chronic granulomatous disease (NADPH oxidase deficiency/dysfunction); voriconazole is first-line treatment
600
A 26 yo female presents to clinic with a chronic cough. Additionally, in recent days she has been experiencing tender lesions on her shins. She has no past medical history. She enjoys traveling to different locations around the US, and recently did a roadtrip from Ohio to Kentucky to explore different cave sites. A CXR shows:

What would be observed on biopsy?
Answer: Caseating granulomas.
Explanation: This woman has a histoplasma infection. Question highlights the typical region/activities associated, as well as symptom profile. CXR shows hilar lymphadenopathy. Caseating granulomas are typical for biopsy of a lesion in histoplasma infection.