Drugs
Breast Cancer Questions
Cancer Trials
Prostate Cancer Questions
Miscellaneous
100
Maximum lifetime cumulative dose of adriamycin
450-550 mg/m2
100
63-year-old woman undergoes lumpectomy and sentinel lymph node biopsy for a newly diagnosed right breast cancer. On pathologic testing, she is noted to have 1.4-cm grade 2 invasive ductal carcinoma that is estrogen receptor–positive (95%), progesterone receptor–positive (95%), and HER2-negative (0 by immunohistochemistry). Her margins are negative. One of three lymph nodes has an 8-mm metastatic deposit. Radiation therapy is planned.
What is best next step in management?
Send Oncotype Dx, if more than 25 for her treat with adjuvant chemotherapy, followed by AI
RxPONDER trial studied postmenopausal patients with hormone receptor–positive breast cancer involving one to three lymph nodes. Trial results showed that a 21-gene recurrence score assay (Oncotype DX) should be ordered to assess the need for adjuvant chemotherapy. In patients with a recurrence score of 25 or below, there was no benefit of adjuvant chemotherapy seen. This finding was limited to postmenopausal patients. Oncotype testing assumes that the patient will receive five years of adjuvant endocrine therapy.


100
A trial which was presented at ASCO 2022 plenary session, which received standing Ovation and changed management of breast cancer patients who were previously not able to get anti her2 drugs.
Destiny-Breast 04.
Destiny Breast 01 - open-label, single-group, multicenter, phase 2 study. Median duration of progression-free survival was 16.4 months. response to therapy was reported in 112 patients (60.9%; 95% confidence interval [CI], 53.4 to 68.0)
Destiny Breast 02 - because DB01 was a single arm phase two trial, it needed confirmation and that was the rationale for doing the DESTINY-Breast02 trial, looking at the post T-DM1 population comparing trastuzumab Deruxtecan versus treatment of physician's choice, which in this trial was either capecitabine with trastuzumab or with lapatinib. randomized, open-label, multicenter, phase 3 trial was conducted at 227 sites. aged 18 years or older, had unresectable or HER2-positive metastatic breast cancer, previously received trastuzumab emtansine, disease progression, an Eastern Cooperative Oncology Group performance status of 0 or 1, and adequate renal and hepatic function. Median PFS was 17.8 vs 6.9 months (p<0.0001). Median OS 39.2 months vs 26.5 months (p=0.0021).
Destiny Breast 3 - phase 3, multicenter, open-label, randomized trial to compare the efficacy and safety of trastuzumab deruxtecan (a HER2 antibody–drug conjugate) with those of trastuzumab emtansine in patients with HER2-positive metastatic breast cancer previously treated with trastuzumab and a taxane. alive without disease progression at 12 months was 75.8% (95% confidence interval [CI], 69.8 to 80.7) with trastuzumab deruxtecan and 34.1% (95% CI, 27.7 to 40.5) with trastuzumab emtansine (hazard ratio for progression or death from any cause, 0.28; 95% CI, 0.22 to 0.37; P<0.001). An overall response (a complete or partial response) occurred in 79.7% (95% CI, 74.3 to 84.4) of the patients who received trastuzumab deruxtecan and in 34.2% (95% CI, 28.5 to 40.3) of those who received trastuzumab emtansine.
Destiny Breast 04 -60% of human epidermal growth factor receptor 2 (HER2)–negative metastatic breast cancers express low levels of HER2, defined as a score of 1+ on immunohistochemical (IHC) analysis or as an IHC score of 2+ and negative results on in situ hybridization (ISH). median progression-free survival was 10.1 months in the trastuzumab deruxtecan group and 5.4 months in the physician’s choice group (hazard ratio for disease progression or death, 0.51; P<0.001), and overall survival was 23.9 months and 17.5 months, respectively (hazard ratio for death, 0.64; P=0.003)
Destiny Breast 05 - A Phase 3, Multicenter, Randomized, Open-Label, Active-Controlled Study of Trastuzumab Deruxtecan (T-DXd) Versus Trastuzumab Emtansine (T-DM1) in Participants With High-Risk HER2-Positive Primary Breast Cancer Who Have Residual Invasive Disease in Breast or Axillary Lymph Nodes Following Neoadjuvant Therapy (DESTINY-Breast05)
Destiny breast 06 - A Phase 3, Randomized, Multi-center, Open-label Study of Trastuzumab Deruxtecan (T-DXd) Versus Investigator's Choice Chemotherapy in HER2-Low, Hormone Receptor Positive Breast Cancer Patients Whose Disease Has Progressed on Endocrine Therapy in the Metastatic Setting (DESTINY-Breast06)
Destiny Breast 07 - A Phase 1b/2 Multicentre, Open-label, Modular, Dose-finding and Dose-expansion Study to Explore the Safety, Tolerability, and Anti-tumour Activity of Trastuzumab Deruxtecan (T-DXd) in Combination With Other Anti-cancer Agents in Patients With HER2-positive Metastatic Breast Cancer (DESTINY-Breast07)
Destiny Breast 08 - A Phase 1b Multicentre, Open-label, Modular, Dose-finding and Dose-expansion Study to Explore the Safety, Tolerability, Pharmacokinetics and Anti-tumour Activity of Trastuzumab Deruxtecan (T-DXd) in Combination With Other Anti-cancer Agents in Patients With Metastatic HER2-low Breast Cancer (DESTINY-Breast08)
Destiny Breast 09 - Phase III Study of Trastuzumab Deruxtecan (T-DXd) With or Without Pertuzumab Versus Taxane, Trastuzumab and Pertuzumab in HER2-positive, First-line Metastatic Breast Cancer (DESTINY-Breast09)
Destiny Breast 12 - An Open-Label, Multinational, Multicenter, Phase 3b/4 Study of Trastuzumab Deruxtecan in Patients With or Without Baseline Brain Metastasis With Previously Treated Advanced/Metastatic HER2-Positive Breast Cancer (DESTINY-Breast12)
100
What is mechanism of action of Zytiga?
inhibits CYP17A1, which manifests as two enzymes, 17α-hydroxylase and 17,20-lyase

Hence prednisone is given with zytiga, also we have to monitor for mineralocorticoid side effects.
100
What is nickname of Syracuse?
"The Salt City"
Onondaga lake was previously called "salt lake". Salt production industry boomed in 1700s-early 1900s. And as there was rapid development of salt production industry, the city got a nickname of "The Salt City".
200
Name of Phosphoinositide 3-kinase inhibitor used in Breast cancer treatment.
Alpelisib (Piqray) - Based on SOLAR 1 trial, which showed treatment with alpelisib–fulvestrant prolonged progression-free survival among patients with PIK3CA-mutated, HR-positive, HER2-negative advanced breast cancer who had received endocrine therapy previously.
Idelalisib (Zydelig), Copanlisib (Aliqopa), Duvelisib (Copiktra), Umbralisib (Ukoniq), Leniolisib (Joenja) - Most of them are usually used in follicular lymphoma, SLL/CLL, Marginal Zone lymphoma.
200
A 43-year-old woman with a history of early stage triple-negative breast cancer (TNBC) presents with new back pain and shortness of breath. She is found to have widespread metastatic disease to her lungs, liver, and bone. Liver biopsy confirms metastatic invasive ductal carcinoma, negative for estrogen receptor, progesterone receptor, and HER2. She was previously treated for a T1cN0M0 TNBC with lumpectomy, sentinel lymph node biopsy, breast radiation, and adjuvant chemotherapy with dose-dense doxorubicin, cyclophosphamide, and paclitaxel, was completed 11 months before her metastatic breast cancer diagnosis.
Which of the following is the most appropriate next step?
Check PD-L1, if CPS is 10 or higher, can be treated with chemo + keytruda.
Based on Keynote 355
The addition of pembrolizumab to chemotherapy with either paclitaxel, nab-paclitaxel, or carboplatin-gemcitabine improved progression-free and overall survival
200
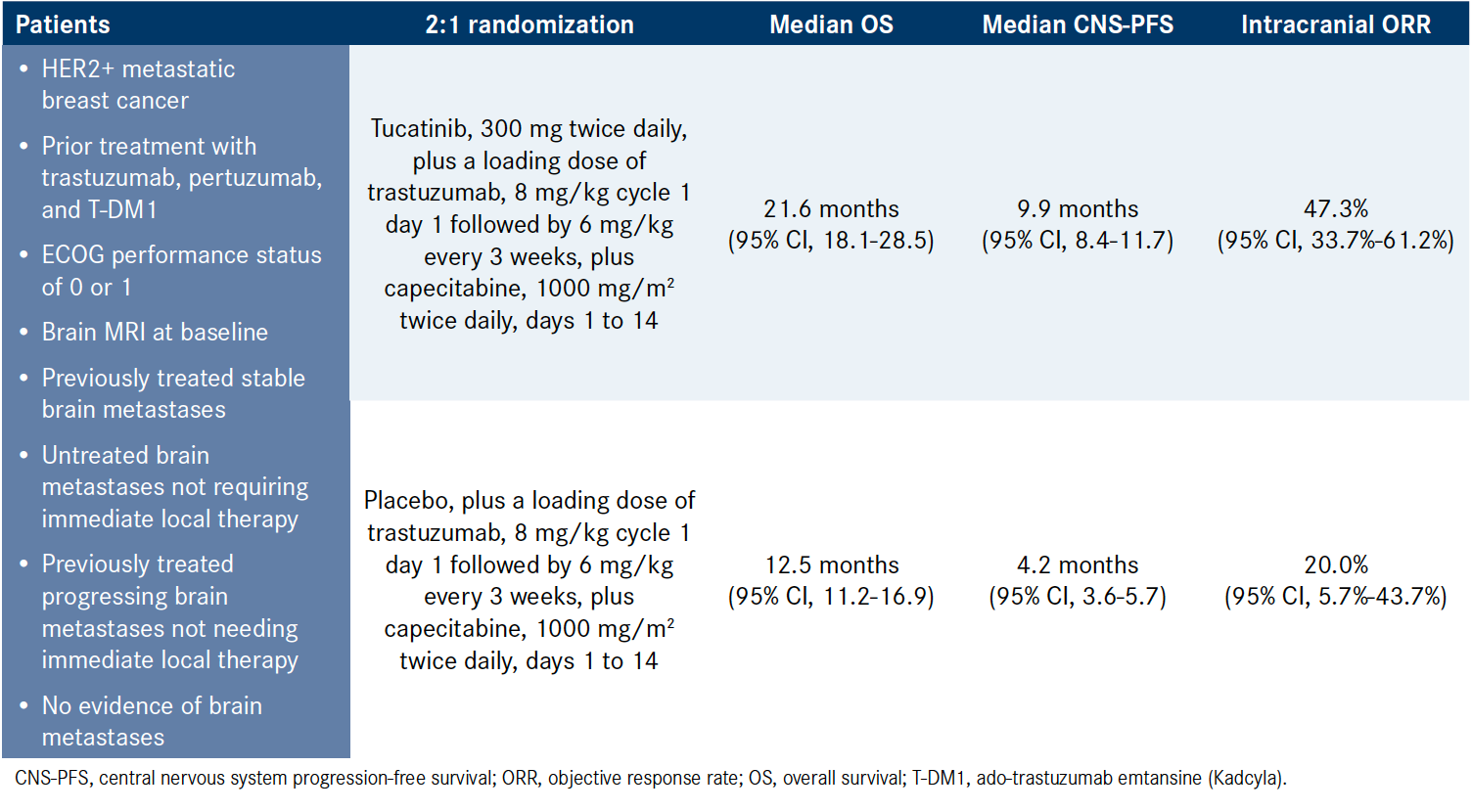
Trial name which showed benefit of tucatinib in breast cancer with mets to brain?
The combination of tucatinib/trastuzumab/capecitabine received FDA approval in April 2020 for patients with metastatic HER2-positive breast cancer, including those with brain metastases, based on efficacy results from HER2CLIMB .
200
A 63-year-old man with metastatic castration-resistant prostate cancer and an excellent performance status returns to your oncology clinic to review recent test results and recommendations. He was originally diagnosed with early stage disease 7 years ago and underwent definitive surgery. When he relapsed 2 years ago with bone and lymph node metastases, he was started on androgen deprivation therapy (ADT), abiraterone, and prednisone. Germline testing was negative for BRCA1/2 mutations. Initial response was good, noted by achieving an undetectable prostate-specific antigen (PSA) level; however, 6 months ago, restaging done as a result of rising PSA level revealed progressive skeletal and lymph node disease, as well as new liver metastases. Docetaxel was initiated but the patient‘s disease continued to progress. PSMA PET/CT scan was performed and no hypermetabolic uptake was seen within the known metastatic lesions.
Which of the following should you recommend now?
a. Cabazitaxel
b. Enzalutamide
c. Lutetium-177 (Lu-177)–PSMA-617
b. Rucaparib
A.
In the absence of PSMA-avid disease, cabazitaxel is the appropriate third-line treatment for progressive, metastatic, castration-resistant prostate cancer. Enzalutamide has little activity following the use of abiraterone/prednisone and docetaxel. Lu-177–PSMA-617 is indicated for men with PSMA-avid, metastatic, castration-resistant prostate cancer after treatment with at least one line of nonhormonal therapy and one line of taxane-based chemotherapy. Rucaparib is only indicated in men with known homologous recombination repair mutations (eg, BRCA1/2) after treatment with both nonhormonal therapy and taxane-based chemotherapy.
200
Most visited event in Syracuse?
New York State Fair.
It handles a lot of people with highest one day record of 147,749 on day 11 in 2019.
300
Does T-DM1 has bystander effect?
No.
Emtansine is microtubule inhibitor, but is not cell membrane permeable, unlike deruxtecan.
Main differences between T-DM1 and T-Dxt:
1. as mentioned above, T-Dxt has cell membrane permeability and hence has bystander effect
2. 3.5:1 payload to mAb in T-DM1; while 8:1 payload to mAB in T-Dxt
3. the linker molecule in T-DM1 is non cleavable, which gives more stability to the drug in plasma, while T-Dxt is cleavable, which is cleaved by specific enzymes, usually more in cancer cells, and in this case is cathepsin B. Cathepsin B are usually overexpressed in cancer cells, allowing the drug to be released precisely in the vicinity of the tumor. In addition, the linkers are usually stable in the systemic circulation due to the presence of protease inhibitors in the blood, and it reduces the risk of side effects. other eg. Brentuximab vedotin.
300
A 39-year-old woman presents with a left breast mass. Imaging demonstrates a 45-mm mass in her left breast with several suspicious axillary nodes. Biopsy reveals invasive ductal cancer, grade 2, that is estrogen receptor–positive (100%), progesterone receptor–negative, HER2-negative, with Ki-67 expression of 35%. Core biopsy of an axillary node is positive for carcinoma, clinical stage cT2, N1. Systemic staging is negative for metastatic disease. She is premenopausal. She has two children and is not planning on further pregnancies. She receives preoperative chemotherapy with doxorubicin and cyclophosphamide, followed by paclitaxel with minimal clinical response. She undergoes bilateral mastectomies with left axillary lymph node dissection. Final pathology is ypT2 (25 mm), pN1 (two nodes with macrometastases). Postmastectomy radiation is planned.
Which of the following should you recommend now?
Ovarian Suppression with an AI and abemaciclib.
Based on TEXT/SOFT data, that AI (exemestane) had better outcome than Tamoxifen.
The MonarchE trial recruited patients with high-risk, hormone receptor–positive breast cancer based on anatomic stage and/or high Ki-67 expression. The addition of abemaciclib to endocrine therapy significantly improved invasive disease-free and distant recurrence-free survival compared to endocrine therapy alone. The FDA approved the use of adjuvant abemaciclib for patients with hormone receptor–positive, HER2-negative, node-positive breast cancer at high risk of recurrence and a Ki-67 score of at least 20%.
The CREATE-X trial evaluated capecitabine for six to eight cycles in patients with residual HER2-negative breast cancer after preoperative chemotherapy. Although the trial was positive, the benefit was largely seen in patients with triple-negative breast cancer and the difference in disease-free survival was not significant in patients with hormone receptor–positive disease.
300
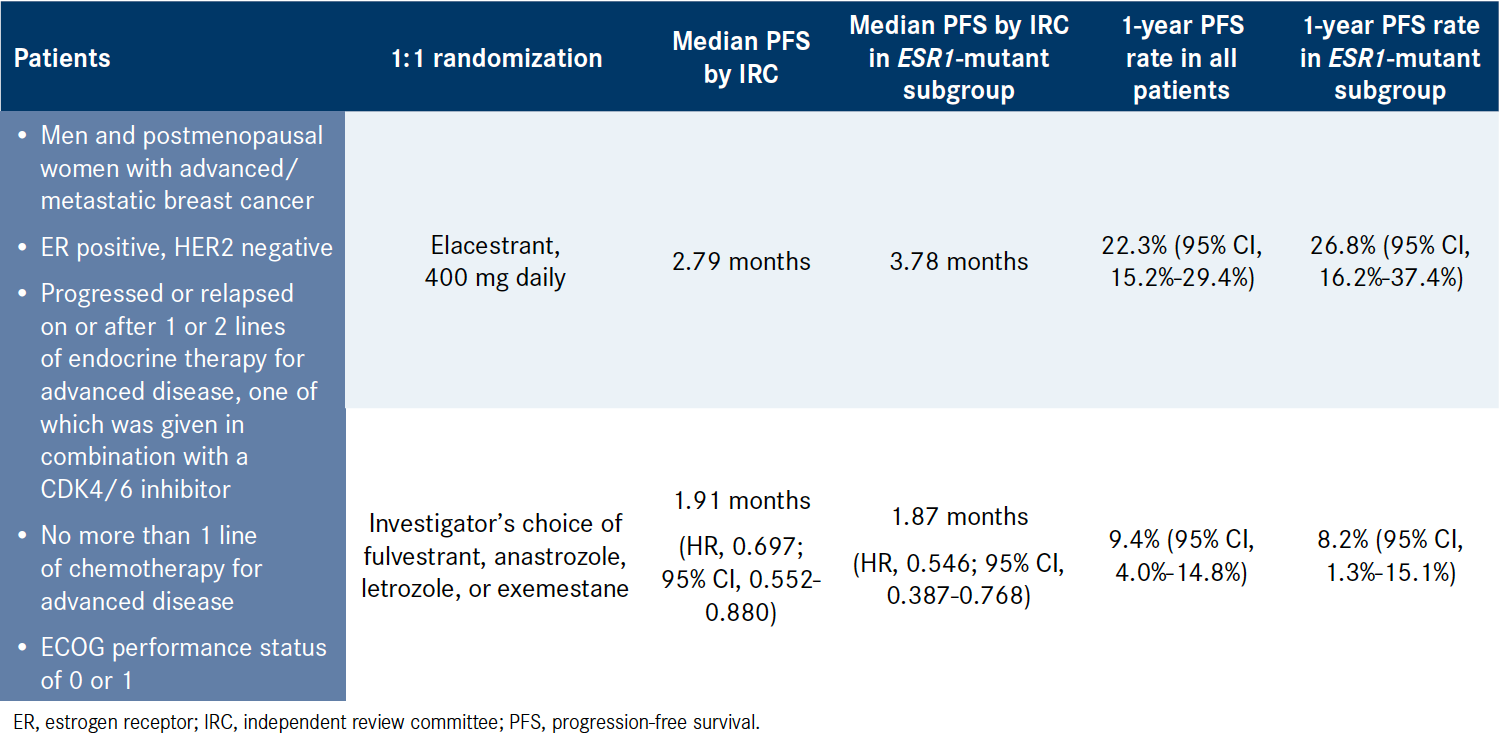
What drug was studied in EMERALD Trial and in which setting?
first oral selective estrogen receptor degrader, elacestrant, against treatment of physician’s choice, standard-of-care endocrine therapy.
300
76 year old male referred to you for recently diagnosed with prostate adenocarcinoma on biopsy, which was done for PSA result of 12ng/ml. Physical exam reveals palpable tumor only on right side. You reviewed the biopsy report which mentioned that he has 5/12 core positivity, with gleason score of 8 (4+4). Staging scans done shows no distant mets/lymph node enlargement.
What is the stage, risk and volume of the prostate cancer?
It is high risk, low volume, stage IIC (cT2bN0M0).
300
When was SUNY Upstate Medical University founded?
- Founded in 1834 Gevena medical school (Dr. Elizabeth Blackwell, first female MD, studied here).
- In 1871, GMC was disbanded and Syracuse University of Medicine was started.
- SUNY took over the medical university in 1951. Upstate is the 15th oldest accredited medical school in the United States.
Fun Fact:
- Dr. William (Bill) Williams, was recruited in 1969 as chair of medicine at SUNY.
- Sarah Marinda Loguen Fraser, (January 29, 1850 – April 9, 1933) was an American physician and pediatrician. She was the fourth female African-American physician in the United States, and the first female doctor in the Dominican Republic. In 1876, she became the first woman to gain an M.D. from Syracuse University School of Medicine. When Sarah Fraser died in 1933, the Dominican Republic declared a nine-day period of national mourning with flags flown at half-mast. A small park in Syracuse honors the Loguen family, including a mural of the family, while the Child Care Center at Upstate Medical University is named in Sarah’s honor. Each year, Upstate also awards the "Sarah Loguen Fraser Scholarship" to a first or second year medical student who demonstrates need and "holds similar ideals to Dr. Sarah Loguen Fraser.
Data from 2018:
Nearly 7,900 SUNY Upstate alumni physicians are licensed throughout the United States. Tripp Umbach estimates that these alumni are generating more than $24.8 billion in economic activity and support or employ nearly 132,354 employees throughout the United States.
400
Name FDA approved CDK4/6 inhibitors for advanced breast cancer treatment?
And which can be given in early breast cancer?
Palbociclib (Ibrance)
Ribociclib (Kisqali)
Abemaciclib (Verzenio) - Based on MonarchE trial verzenio was approved by FDA to be given in high risk early breast cancer as adjuvant therapy for HR+/HER2- patient with hormone therapy. The study has shown significant invasive disease free survival.
400
A 45-year-old premenopausal woman presents to the office for a follow-up visit after completing neoadjuvant chemotherapy with dose-dense doxorubicin and cyclophosphamide, followed by paclitaxel and carboplatin for a 4.1-cm left breast cancer. There was no evidence of lymph node involvement. The tumor was estrogen receptor–positive (5%), progesterone receptor–negative, and HER2-negative. After completing neoadjuvant chemotherapy, she underwent left mastectomy with sentinel lymph node evaluation and prophylactic right mastectomy with sentinel lymph node evaluation. One small foci of residual carcinoma measuring 0.3 cm within a 4-cm tumor bed was noted in the postoperative specimen. Three benign sentinel lymph nodes were removed. Repeat biomarker status on the residual disease is notable for estrogen receptor, progesterone receptor, and HER2-negative disease. Right breast mastectomy specimen and lymph nodes were benign. Genetic testing is notable for pathologic BRCA2 mutation. She will meet with a gynecologic surgeon for prophylactic bilateral salpingo-oophorectomy.
Which of the following should you recommend now?
Olaparib
In this patient with residual cancer after adequate neoadjuvant chemotherapy, 1 year of adjuvant olaparib is indicated based on the results from OlympiA trial which showed improved overall survival in the adjuvant setting when compared with placebo in patients who have high-risk, HER2-negative breast cancer with pathogenic or likely pathogenic germline mutations in BRCA1 and BRCA2
400
What were the trials which showed benefit of continuing Tamoxifen beyond 5 years in adjuvant setting?
ATLAS (Davies et el, 2012): N = 6846; Risk of recurrence: 21% vs 25%; P=0.002, Breast cancer mortality: 12% vs 15%; P=0.01, Overall mortality: 639 vs 722 deaths; P=0.01
ATTOM (Gray et el, 2013): N = 6953; Recurrence rate: 17% vs 19%; P=0.003, Breast cancer mortality: 392 vs 443 deaths; P=0.05, Overall mortality: 849 vs 910 deaths; P=0.1.
400
A 82-year-old man with coronary artery disease and diabetes mellitus managed on insulin has a remote history of intermediate-risk prostate cancer (Gleason score of 7 [3+4]). He was treated with radiation 13 years ago and is now seeking to establish care. He has no urinary symptoms at this time, though he reports diminished erectile function since completing radiation therapy. Records reveal he had Gleason 3+4 disease in three of 12 cores, involving up to 30% of the cores with an initial prostate-specific antigen (PSA) level of 5.7 ng/dL; after radiation, his PSA nadir was 0.3 ng/dL. Records from the past two years show PSA levels of 0.7 ng/mL, 0.9 ng/mL, and most recently, 1 ng/mL. Digital rectal examination detected no abnormalities. He is concerned about the rise in his PSA levels.
Which of the following is the most appropriate next step?
a. Obtain bone scan and CT of the chest, abdomen, and pelvis
b. Obtain MRI of the prostate
c. Obtain prostate-specific membrane antigen (PSMA) PET/CT scan
d. Reassure patient and repeat PSA testing in six months
D.
This patient underwent definitive treatment with radiation more than 12 years ago with a PSA nadir of 0.3 ng/mL. Per the Phoenix criteria, a PSA relapse is defined as a PSA level 2 ng/mL greater than the patient‘s absolute PSA nadir after completing external beam radiation therapy. Given this patient‘s PSA nadir of 0.3 ng/mL, a PSA level concerning for relapse would be 2.3 ng/mL. If PSA level is rising after radiation but not yet 2 ng/mL over nadir, recurrence evaluation may be considered, especially in patients who are young and healthy. In this patient with multiple comorbidities and a PSA level below the criteria for relapse, reassurance and monitoring without additional imaging is most appropriate.
PSA doubling time: The risk of prostate cancer death within five-years of relapse was 50% for patients with a PSA doubling time of 12 months or less compared to 10% for patients with a doubling time greater than 12 months.
400
What was the first ever chemotherapy regimen for breast cancer?
Cyclophosphamide + Methotrexate + 5 FU (CMF) was first effective chemotherapy regimen for breast cancer (Bonadonna et al. 1976).
- mustard gas used in World War I and II showed that there is decrease in blood counts and when studied in rats showed decrease in the lymphomas
- Dr. Gilman and Dr. Goodman, in 1946 used nitrogen mustards as chemotherapy.
- At the same time in 1948, Dr. Farber et al. worked on antifolate mechanism for cancer treatment.
- Later in 1957, 5 FU was developed and studied in mouse.
Which led to first chemotherapy regimen for breast cancer : CMF
Anthracyclines were also discovered around same time, and studied in breast cancer as well, but first regimen to become gold standard till date was Doxorubicin+Cyclophosphamide (AC), and the data was published in 1990 by Fisher et al.
Fun Fact:
First ever radical surgery performed for breast cancer was in 1882 by Dr. William Halsted in NY.
In 1898, Marie and Pierre Curie discovered Radioactive elements radium and polonium, and after that they were used in cancer treatment.
In 1920, radium was used following conservative surgery by surgeon Geoffrey Keynes at St. Bartholomew’s, London, producing equivalent survival rates to Halsted’s radical mastectomy.

500
56 year old female comes for follow up after getting started on abemaciclib and letrozole for metastatic HR+/HER2- lobular breast carcinoma with mets to liver and spine. Her routine blood work shows elevated creatinine of 1.3, one month ago was 0.9.
What is the best next step in management of AKI.
1. Check history of diarrhea (as verzenio can cause diarrhea and about 90% patients will have it).
2. Verzenio has been shown to increase serum creatinine due to inhibition of renal tubular transporters, without affecting glomerular function. So check cystatin C for checking accurate GFR.
500
A 54-year-old woman presents to your clinic for management of HER2-positive early breast cancer. She has completed six cycles of docetaxel, carboplatin, trastuzumab, and pertuzumab (TCHP) chemotherapy and has undergone surgery. Surgical pathology findings revealed residual invasive disease.
Which of the following is the most appropriate next step?
T-DM1 based on Katherine Trial, which showed that T-DM1 increased invasive disease-free survival in patients who had residual invasive, HER2-positive, early breast cancer after completing six cycles of TCHP therapy.
500
Drug studied in ASCENT Trial?
Sacituzumab govitecan-hziy vs. chemotherapy.
median PFS for patients receiving sacituzumab govitecan was 4.8 months (95% CI: 4.1, 5.8) compared with 1.7 months (95% CI: 1.5, 2.5) in those receiving chemotherapy (HR 0.43; 95% CI: 0.35, 0.54; p<0.0001). Median OS was 11.8 months (95% CI: 10.5, 13.8) and 6.9 months (95% CI: 5.9, 7.6) respectively (HR 0.51; 95% CI: 0.41, 0.62; p<0.0001).
500
The patient is a 67-year-old man with known prostate cancer; he presents to your clinic with a rising prostate-specific antigen (PSA) level. He was originally diagnosed five years prior, when he was found to have a PSA of 8.5 ng/mL and cT2 disease with a Gleason score of 9 (5 + 4) in eight of 12 cores. He underwent robotic prostatectomy, which demonstrated stage pT3bN0 disease and a focally positive margin. His PSA level four weeks after surgery was 0.2 ng/mL. Cross-sectional imaging demonstrated no evidence of disease. He completed salvage radiation with six months of androgen deprivation therapy with leuprolide. His PSA level became undetectable. Two years later, his PSA once again became detectable at 0.2 ng/mL, rising to 0.4 ng/mL three months later. Cross-sectional imaging at that time demonstrated no evidence of disease. He was started on androgen deprivation therapy with leuprolide, lowering his PSA to undetectable levels. Since then, his PSA has risen to detectable levels and continued to increase gradually. Today, his PSA level is 2.0 ng/mL. His PSA doubling time is nine months. Cross-sectional imaging demonstrates no evidence of disease.
Which of the following should you recommend now?
a. Bicalutamide
b. Darolutamide
c. Docetaxel
d. Observation
Darolutamide
In the ARAMIS trial, patients with non metastatic castration resistant prostate cancer, a baseline PSA level of at least 2 ng/mL, and a PSA doubling time of 10 months or less were randomly selected in a 2:1 ratio to receive darolutamide (600 mg twice daily) or placebo while continuing androgen-deprivation therapy. The primary endpoint was metastasis-free survival. In the planned primary analysis, the median metastasis-free survival was 40.4 months with darolutamide, as compared to 18.4 months with placebo (hazard ratio for metastasis or death in the darolutamide group, 0.41; 95% CI, 0.34-0.50; P less than .001). Darolutamide was also associated with benefits with regard to secondary endpoints, including overall survival, time to pain progression, time to cytotoxic chemotherapy, and time to a symptomatic skeletal event.
500
Where in Syracuse there is a green light above red light?
Tipperary Hill, in front of Coleman Irish Pub.
Its one of a kind in USA