There she blows
How do I fix it MR.?
TR what now?
No Longer Forgotten
100
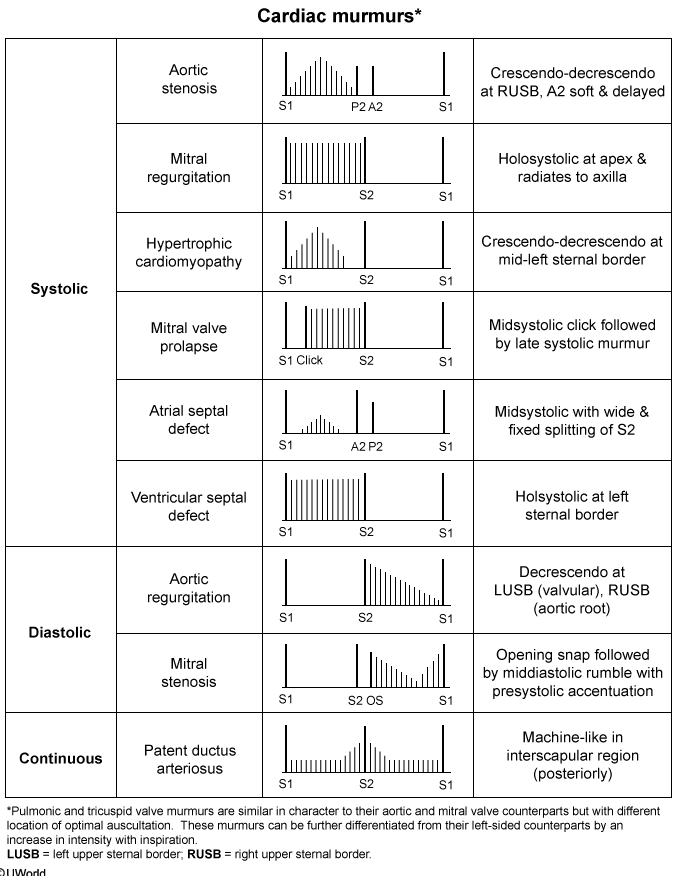
What type of murmur is associated with chronic mitral regurge?
A. Crescendo-decresendo murmur at the mid-left sternal border
B. Blowing, holosystolic murmur at the apex
C. Midsystolic click followed by a late systolic murmur
D. Opening snap followed by a middiastolic rumble with pre-systolic accentuation
B. Blowing, holosystolic murmur at the apex
100
In the absence of symptoms or LV dysfunction, is medical therapy with validators beneficial to patients with PRIMARY mitral regurgitation?
No.
Vasodilator therapy is generally not indicated for asymptomatic patients with chronic MR due to lack of data showing benefit and the possibility of masking symptoms that may indicate a need for surgical intervention.
100
Describe the murmur of Tricuspid regurgitation.
A. Crescendo-Decrescendo systolic murmur
B. A high pitched, holosystolic murmur
C. Continuous machine like murmur
D. Late systolic murmur with midsystolic click
B. A high pitched, holosystolic murmur best heard at the left lower sternal border that radiates to the right lower sternal border. Best auscultated over the 4th left sternal border
100
Which physical exam finding is not typically associated with isolated Tricuspid Regurgitation?
A. S3 heart sound
B. JVD
C. Pulmonary edema
D. Hepatomegaly
C. Pulmonary edema is not commonly associated with Tricuspid regurgitation.
Symptomatic TR typically presents with signs and symptoms of RHF : jugular venous distention, ascites, and peripheral edema.
200
Which of these can increase the intensity of the murmur of mitral valve regurgitation?
A. Squatting from a standing position
B. Valsalva maneuver
C. Transient arterial occlusion or hand-grip exercises
D. Amyl nitrate inhalation
C. Transient arterial occlusion or hand-grip exercises
Hand-grip exercises, performed by having the patient squeeze both hands intensely for at least one minute, increases afterload. When the afterload is increased, there is more resistance to blood flow from the left ventricle through the aortic valve, and thus more blood regurgitates through the mitral valve.
Transient arterial occlusion, or TAO, is performed by inflating blood pressure cuffs on both arms to increase the afterload. This has the same effect on the murmur of mitral regurgitation as handgrip exercises and may be the preferred method if a patient is not able to adequately perform a strong handgrip.
200
Guideline-directed therapy for ventricular dysfunction in patients with chronic secondary mitral regurgitation includes all of the following except:
A. ACE inhibitors
B. ARB's
C. Angiotensin receptor-neprilysin inhibitors (ARNi)
D. Calcium channel blockers
E. Beta blockers
F. Diuretics
G. Aldosterone antagonists
D. Calcium channel blockers
200
How does one intensify the murmur of Tricuspid Regurgitation?
A. Deep Inspiration
B. Squatting from standing
C. Valsalva Maneuver
D. Hand Grip exercise
A. Deep Inspiration causes increased venous return resulting in overall increased filling of the right ventricle during diastole and allowing for increased regurgitant flow during systole. This helps to distinguish it from mitral regurgitation.
This inspiratory enhancement of the tricuspid regurgitation murmur is called "Carvallo's sign".
200
For patients with isolated symptomatic TR, which class(es) of medication are considered the mainstay of medical therapy?
A. Loop Diuretic
B. Aldosterone Antagonists
C. Beta-Blockers
D. ACE/ARB
E. A&B
F. C&D
E.
Recall that patients with symptomatic TR are suffering from symptoms of right-sided heart failure. As such patients are experiencing symptoms of volume overload include JVD, peripheral edema, and hepatic congestion. Loop Diuretics provide the mainstay of therapy in treating the volume overload status of the patient with Aldosterone antagonsits (spironalactone) usually being added when patients present with symptoms of hepatic congestion (ascites)
300
5. Which of the following is most likely to cause acute severe mitral valve regurgitation from papillary muscle rupture?
A. Anterior myocardial infarction
B. Inferior myocardial infarction
C. Lateral myocardial infarction
B. Inferior myocardial infarction
An inferior myocardial infarction is more likely to cause a posteromedial papillary muscle rupture and acute mitral regurgitation causing severe acute mitral valve regurgitation which can be life threatening if not immediately surgically repaired.
There are two papillary muscles that comprise the mitral valve. The anterolateral papillary muscle receives dual blood supply from the left anterior descending coronary artery and the left circumflex coronary artery in most individuals while the posteromedial papillary muscle receives its sole blood supply from the right coronary artery.
Complete infarction of the posteromedial papillary muscle can occur during an inferior MI (from thrombosis of the right coronary artery) while only partial or no damage will be done to the anterolateral papillary muscle during an anterior (left anterior descending) or lateral (circumflex) infarction since there is dual blood supply to this papillary muscle.
300
Which of the following has been shown to delay the need for mitral valve repair or replacement in the setting of severe mitral regurgitation?
A. Beta-blockers
B. Angiotensin converting enzyme inhibitors
C. Non-dihydropyridine calcium channel blockers
D. Hydralazine
E. None of the above
E. None of the above
No pharmacotherapy exists that can delay the need for mitral valve repair or replacement in the setting of severe mitral valve regurgitation.
Pharmacotherapy directed at afterload reduction with vasodilators can be useful during acute decompensated heart failure in people with severe MR, however chronic vasodilator therapy is indicated only for non-surgical candidates.
300
What are the two primary categories of Tricuspid Regurgitation and which is more common?
Primary Tricuspid Regurgitation (structural)- disorders of the valve apparatus
Secondary Tricuspid Regurgitation (functional)- regurgitation in the setting of anatomically normal leaflets and cords. Usually caused by dilation of the right ventricle or atrium leading to tethering of the tricuspid valve leaflets or tricuspid anular dilation
300
As functional TR is often associated with significant left sided heard disease, proper management of HF plays an important role. As such, which medication is not involved in initial Guideline Directed Medical Therapy for HFrEF.
A. Angiotensin System Blocker
B. B-Blocker
C. CCB
D. Diuretic
E. Hydralazine
F. Nitrate
C. CCB
Initial guideline directed medical therapy for all patients with HFrEF consists of combination of diuretic, B-Blocker, and ACD/ARB/ARNI or Hydralazine + Nitrate
400
Which of the following is a functional cause of mitral regurgitation?
A. Mitral valve endocarditis
B. Dilated cardiomyopathy
C. Mitral valve prolapse
D. Rheumatic mitral valve disease
B. Dilated cardiomyopathy

Functional MR occurs when the LA or LV dilates causing the MV annulus to also dilate thus preventing the MV leaflets from properly coapting. Organic MR results from actual disease of the MV apparatus. The MV leaflets, annulus, papillary muscles and chordae tendinae must interact properly for the MV to function properly. Thus, disruption of any of these structures can result in organic MR.
The most common cause of chronic MR in the United States is due to the myxomatous changes seen in mitral valve prolapse (MVP). In this condition, the middle layer of the valve leaflets become thickened frequently causing leaflet redundancy making it difficult for them to coapt properly.
400
Which of the following is effective as a bridge to mitral valve repair or replacement in the setting of acute severe mitral valve regurgitation?
A. Intraaortic balloon counterpulsation
B. Nitroprusside
C. Beta-blockers
D. Nitrates
E. A and B
F. All of the above
E. A and B
Reducing afterload is crucial to improve hemodynamics in the setting of acute severe mitral regurgitation. This can be achieved with intraaortic balloon counterpulsation or pharmacotherapy such as nitroprusside, hydralazine or non-dihydropyridine calcium channel blockers.
400
Which of the following is the most common cause of primary Tricuspid regurgitation?
A. Congenital - Ebstein's Anamoly
B. Endocarditis
C. Ischemia - papillary muscle rupture
D. Valve injury from PM or ICD lead
D. Valvular injury from implantable device leads that cross the TV can cause acute/chronic progressive TR.
A study involving 239 individuals receiving first time placement of an implantable device showed ~38% developed TR within 1-1.5 years
400
Grading of tricuspid valve regurgitation is based hemodynamic parameteres measured during 2D echocardiography. Which of the following is not used in determining the severity of TR?
A. Central Jet Area
B. Vena Contracta
C. CW jet density and contour
D. Hepatic vein flow
E. Color flow area of regurgitant jet
E. Color flow area of the reguritant jet can be used to diagnose TR but is not used in the grading of severity.
Severe TR Valve hemodynamics:
- Central jet area >10.0 cm2
- Vena contracta width >0.70 cm
- CW jet density and contour: dense, triangular with early peak
- Hepatic vein flow: systolic reversal
500
6. Which of the following is the cause of mitral regurgitation in the setting of hypertrophic obstructive cardiomyopathy?
A. Myocardial disarray of the papillary muscles causing dysfunction
B. Systolic anterior motion of the mitral valve leaflet into the left ventricular outflow tract
C. Mitral annular dilation causing functional mitral regurgitation
D. Mitral valve leaflet degeneration from the increased hemodynamic stress present in HOCM
B. Systolic anterior motion of the mitral valve leaflet into the left ventricular outflow tract
The Venturi effect is described as a decrease in pressure when blood flows through a stenosis at a high velocity. This relates to the hemodynamics in hypertrophic obstructive cardiomyopathy (HOCM). In HOCM, the increased velocity in the left ventricular outflow tract decreases pressure in this region causing the anterior leaflet of the mitral valve to be pulled in that direction. This is called “systolic anterior motion” of the mitral valve or SAM. Mitral regurgitation can result and contribute to congestive heart failure symptoms in the setting of HOCM.
500
Which is the following is NOT an indication for mitral valve repair or replacement?
A. Severe mitral regurgitation from mitral valve prolapse in an asymptomatic patient when repair instead of replacement is anticipated
B. Severe mitral regurgitation causing severe systolic dysfunction and an ejection fraction of 20% regardless of the etiology
C. Acute severe mitral regurgitation from a rupture papillary muscle after an inferior myocardial infarction
D. Severe mitral regurgitation with normal left ventricular systolic function causing New York Heart Association functional class III symptoms
E. Asymptomatic severe mitral regurgitation with the left ventricular ejection fraction > 60% and end systolic dimension < 40 mm without atrial fibrillation or pulmonary hypertension.
E. Asymptomatic severe mitral regurgitation with the left ventricular ejection fraction > 60% and end systolic dimension < 40 mm WITHOUT atrial fibrillation or pulmonary hypertension.
The indications for mitral valve repair or replacement according to the ACC/AHA guidelines are:
1. Symptoms related to heart failure that can be attributed to the mitral regurgitation and left ventricular ejection fraction > 30% (Class I)
2. Symptoms related to heart failure that can be attributed to the mitral regurgitation and left ventricular ejection fraction < 30%. Mitral repair not replacement likely. (Class IIa)
3. Asymptomatic severe mitral regurgitation if the left ventricular ejection fraction is < 60% and/or the end systolic dimension is > 40 mm. (Class I).
4. Asymptomatic severe mitral regurgitation with the left ventricular ejection fraction > 60% and end systolic dimension < 40 mm if atrial fibrillation or pulmonary hypertension (>50 mm Hg) IS present (Class IIa).
5. Severe mitral valve regurgitation (usually from mitral valve prolapse) if repair rather than replacement is likely, even in the lack of symptoms and normal left ventricular ejection fraction (Class IIa).
500
Functional tricuspid regurgitation is often secondary to pulmonary hypertension. List the WHO classifications for pulmonary hypertension.
Group 1: Pulmonary Arterial Hypertension (primary)
Group 2: Pulmonary hypertension 2/2 left heart disease
Group 3: PHTN 2/2 lung disease or chronic hypoxia
Group 4: PHTN 2/2 thromboembolic disease
Group 5: PHTN 2/2 blood and other disorders
500
Per the ACC/AHA guidelines, which is a class I recommendation for surgical repair of the tricuspid valve?
A. repair or annuloplasty ring in patient's with severe primary TR when right heart failure symptoms are present
B. replacement for severe tricuspid regurgitation due to organic valve disease not amenable to anuloplasty ring
C. annuloplasty ring for moderate TR in patients undergoing mitral valve surgery in the presence of PHTN or tricuspid annular dilation
D. repair in severe TR with mitral valve surgery is planned
D
Surgical repair or replacement is rarely required. The ACC/AHA Guidelines give the following indications to surgically repair the tricuspid valve:
- Repair of the tricuspid valve in severe tricuspid regurgitation when mitral valve surgery is planned (class I, level of evidence B).
- Tricuspid valve replacement or annuloplasty ring is reasonable to severe primary tricuspid regurgitation when right heart failure symptoms are present (class IIa, level of evidence C).
- Tricuspid valve replacement is reasonable for severe tricuspid regurgitation due to organic valve disease that is not amenable to annuloplasty ring (class IIa, level of evidence C).
- Tricuspid annuloplasty ring may be considered for moderate tricuspid regurgitation in patients undergoing mitral valve surgery when there is pulmonary hypertension or tricuspid annular dilatation (class IIb, level of evidence C).