Skin
Skin cancer
Derm pt 3
Development
Rheumatology
Cosplay as Superman
Misc
100
Describe this lesion
A 3cm solid raised lesion with extension into the dermis
Nodule
100
This type of lesion presents as flat and brown smooth maculues. They are uniformly pigmented and are benign. 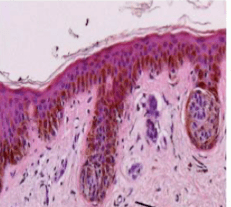

Junctional Melanocytic Nevus
100

Pt is a 26 y/o female presenting with this rash for 1 week. Pt recently recovered from a cold about and then noticed a single lesion that grew. She then noticed more lesions pop up over the next few days.
Pityriasis Rosea
100
These glands are regulated by androgens and retinoids and is commonly associated with hair follicles.
Double Jeopardy: What areas of the body would not have these type of glands?
Sebaceous glands
Palms of hands and soles of feet
100
 What other associated symptoms would you see in a patient with this finding in their synovial fluid?
What other associated symptoms would you see in a patient with this finding in their synovial fluid?
monoarthritis of knee and wrist
Chondrocalcinosis on xray
CCPD-
Acute-treated with NSAID, colchine, glucocorticoid
100
Pt is a 65 y/o female presenting to ER after a slip and fall on ice. What is the deformity in this picture
Closed Tibia and Fibula fracture
Image Cred: My cousin in Law: emily (Her Mom)
100
You suspect your patient has a soft tissue tumor. What is the first imaging you should get?
Xray/ultrasound
200

This often presents within the first year of life and is ultimately grown out of by adulthood.
Atopic Dermatitis
200
This lesion is very common in middle aged and elderly people. It presents as sharply delineated flesh colored or brown black warty plaques with a greasy texture. Often described as a stuck on or pasted appearance.
Seborrheic Keratosis
Due to proliferation of keratinocytes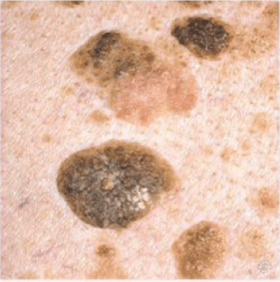
200

This condition is caused by a widespread apoptosis of keratinocytes via activation of cell mediated cytotoxic reaction. It involves >30% of the body surface area and is caused by a severe reaction to some medications
Toxic Epidermal necrolysis
(common meds-NSAIDS, antibiotics, allopurinol anticonvulsants)
200
The limb skeleton, sternum develop from this part of the mesoderm.
Parietal layer of the lateral plate of the mesoderm
200
What clinical presentation would you expect to see with a patient who had a joint aspiration with 150,000 WBC 90% neutrophils
Pt with a swollen red warm to touch joint (single joint primarily knee>>> hip, shoulder, wrist ankle)
fever, malaise, pain, limited to no rand of motion.
Presents acutely 1-2 weeks
positive gram stain (usually Staph culprit)
200
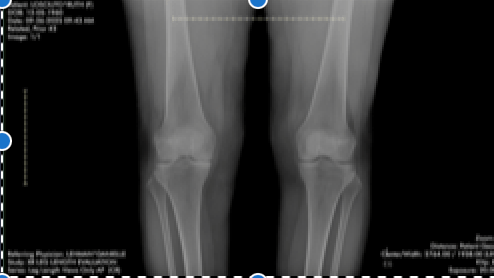
Pt is a 66 y/o female presenting to clinic with x6 months of knee pain. Pt walks every day and noticed she hasn't been able to walk as long or as fast as she used. She doesn't remember any trauma but does have a very large golden doodle she has been training so its possible he could have ran into her. She has a total of 6 siblings and 4/6 have had knee placements (2 had bilateral) and one has has also had a hip replacement. The xray and clinical presentation are most consistent with what clinical diagnosis.
Osteoporosis
Image creds: My Aunt Ruth
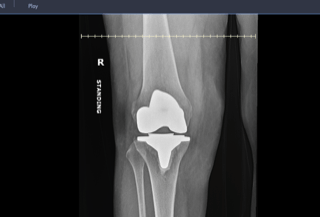
Post Surgery Image.
200
Place these local anesthetics in order of increasing toxicity:
tetracaine, mepivacaine, bupivacaine, lidocaine
lidocaine~mepivacaine<<bupivacaine<tetracaine
300
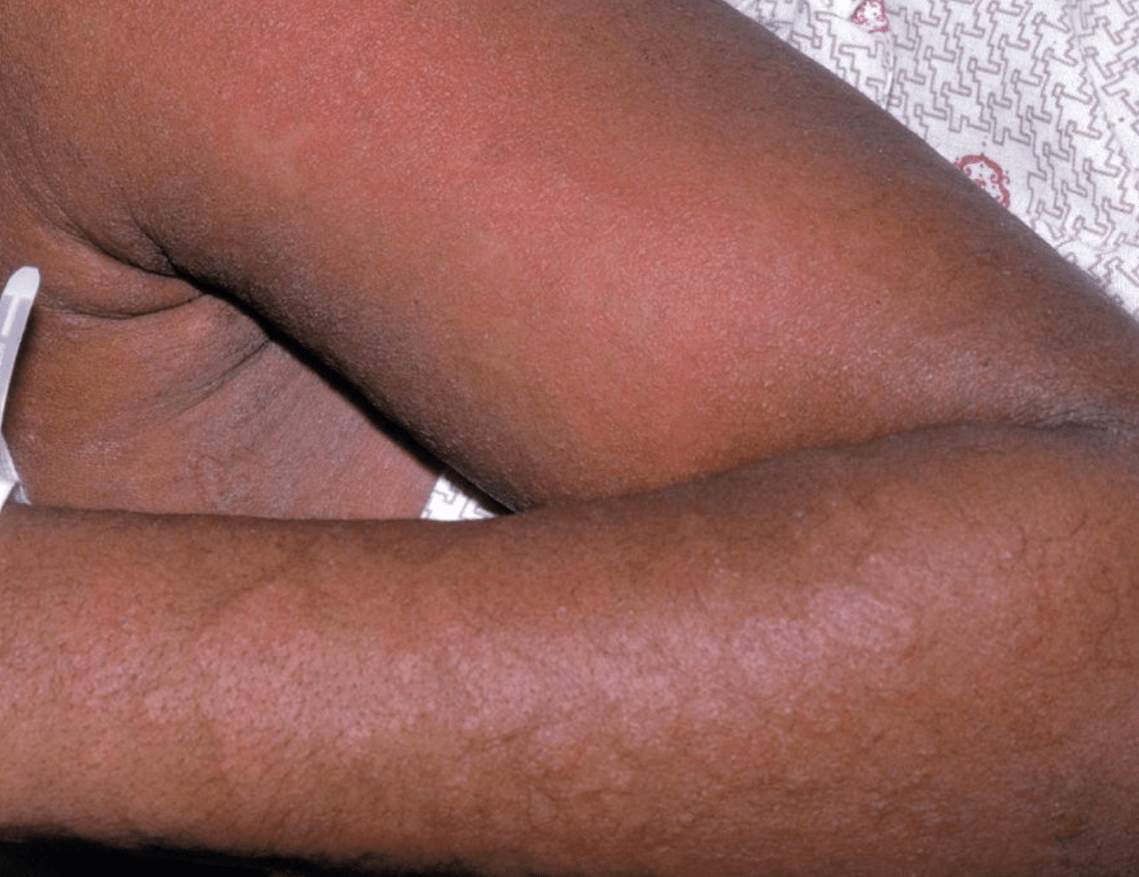
A 16 month old male presents to his pediatrician for erythematous, scaly and pustular lesions on the buttocks, thighs and the posterior scalp with alopecia.
What is the diagnosis and treatment for this patient
Acrodermatitis enteropathica,Oral Zinc

300
50 y/o woman present to her pcp with a 6 month hx o fatigue, night sweats and unintentional weight loss. She denied any recent sickness and has no prior medical hx. She's been to the dermatologist a few times for weird wart on her thumb, but the derm said not to worry it will eventually go away.
This is the wart she is referring to:

What is this called and what does it indicate?
Hutchinson's Sign
Acral Lentiginous Melanoma
300
This idiopathic condition can present with a shawl sign, itchy scalp, mechanic hands, and pink papules over the knuckles. Pts can also have elevated CPK and aldolase.
Dermatomyositis
(Idiopathic inflammatory myopathy)
300
Epidermolytic Ichthyosis is skin condition caused by abnormal secondary keratin. At what level is secondary keratin expressed?
Double Jeopardy: What are these secondary keratins?
Stratum Spinosum
(K1/K10)
300
Match the lab value to the Condtion
Lab values: HLA-B27, SSA/SSB, Scl70, HMGCoa
Conditions: systemic sclerosis, necrotizing myopathy, Spondyloarthritis, Sjogren's Syndrome,
HLA-B27-Spondyloarthritis
SSA/SSB-Sjogren's Syndrome
Scl70-Systemic Sclerosis
HMGCoA-nectrotizing myopathy (from statin use)
300
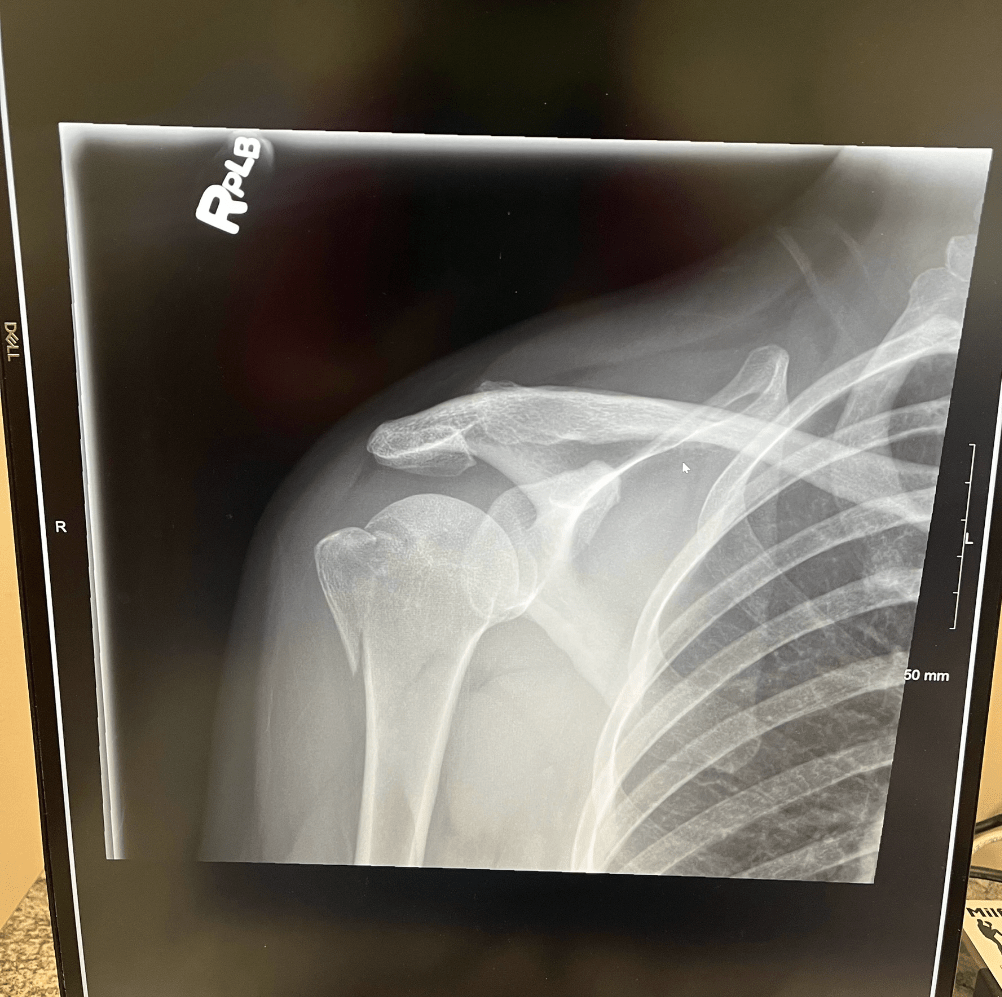 33 y/o female presents to emergency room status post crash while riding a motorcycle with her boyfriend. She is susceptible to a nerve injury that present with this weakness/deficit
33 y/o female presents to emergency room status post crash while riding a motorcycle with her boyfriend. She is susceptible to a nerve injury that present with this weakness/deficit
Flattened deltoid, loss of abduction at shoulder (>15), loss of sensation over deltoid and lateral arm
Axillary Nerve injury
Post surgery repair
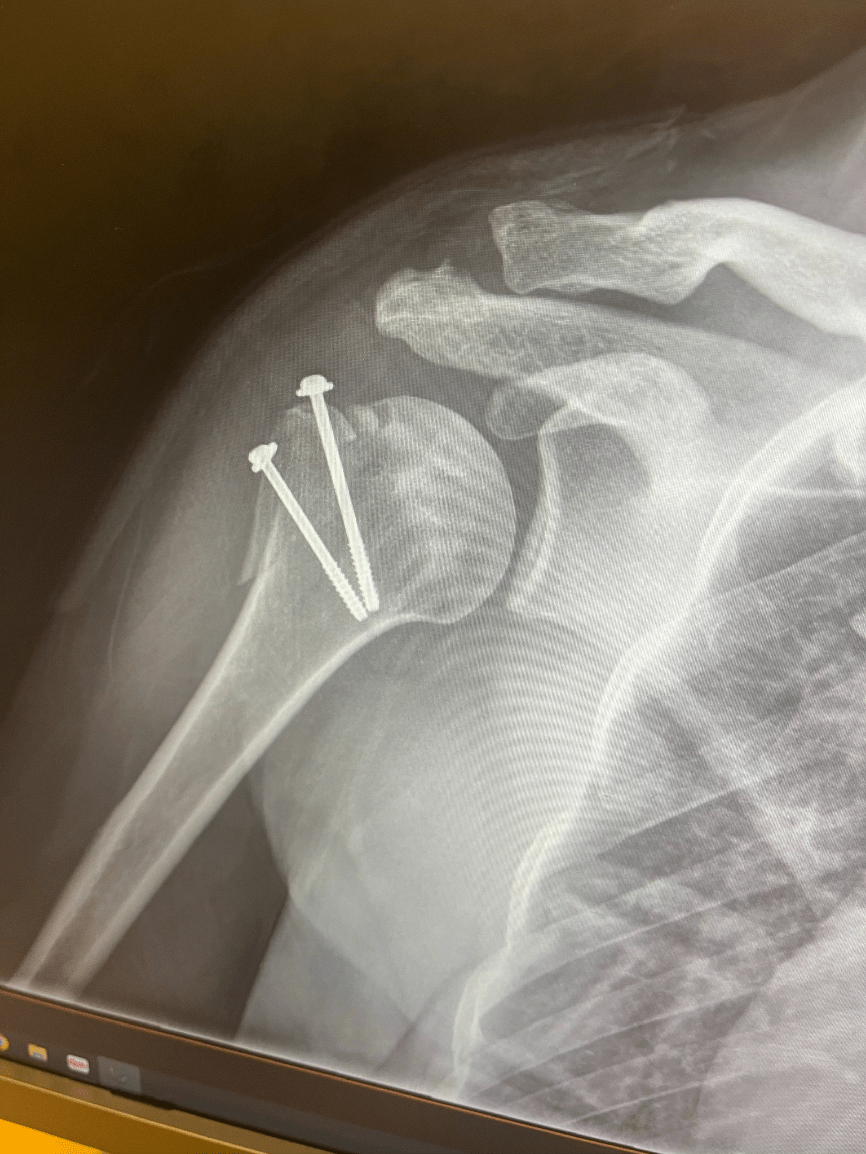
Image cred: My cousin Keri
300
Pts with this condition are at an increased risk of death, disease recurrence, adverse drug reactions and decreased response to medications. Though it can be a natural process with aging, it can be exacerbated by inflammation, hormonal changes and poor nutritional intake.
Sarcopenia
400
What clinical presentation would be associated with these images?

The 5 Ps
Pruritic, purple, planar, polygonal, papulues/plaques
Linchen Planus
400
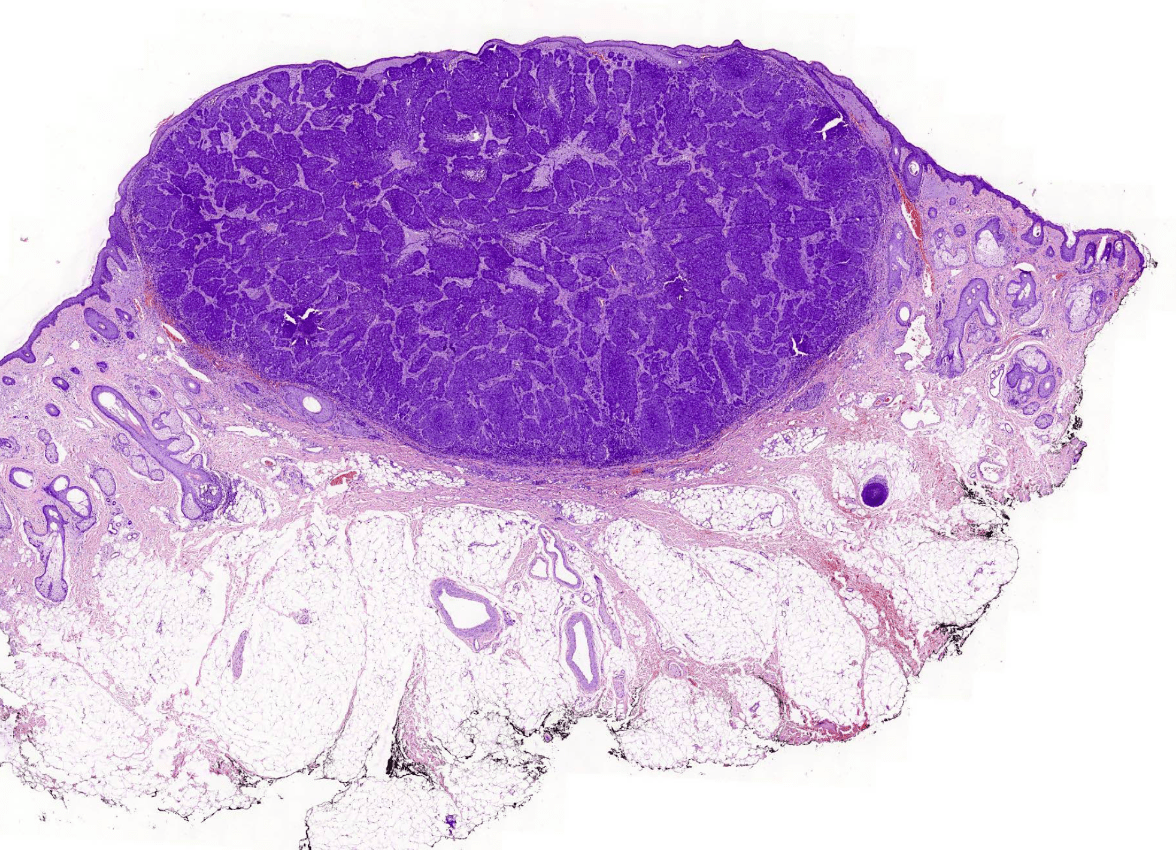
This type of surgery for the lesion in the histology slide has the best cure rate of 97-99%.
Double Jeopardy what type of lesion is this?
Mohs Surgery
Lesion: Nodular Basal Cell Carcinoma
400
This auto-inflammatory disorder often has delayed diagnosis (7-10 years) and presents with tunnels, severe scaring and abscesses. It has a higher prevalence in females.
It typically affects areas with this kind of gland.
Apocrine sweat glands
Hidradenitis suppurativa
400
In order to aid in the process of somite differentiation the notochord secretes these signals to cause the somite to form the sclerotome and express another important signaling model. Name all three.
Sonic Hedgehog, noggin
PAX1
400
pt is a 55 y/o feamle presenting to clinical today with hand and finger pain. Pt stated she has difficulty getting ready for work due to the stiffness in her hands, often taking an extra hour to be be able to start doing her morning routine. Blood work shows elevated ESR CRP and positive CCP. What inflammatory factors are involved with this patients condition.
IL-6, TNF and IL1
Rheumatoid Arthritis
400

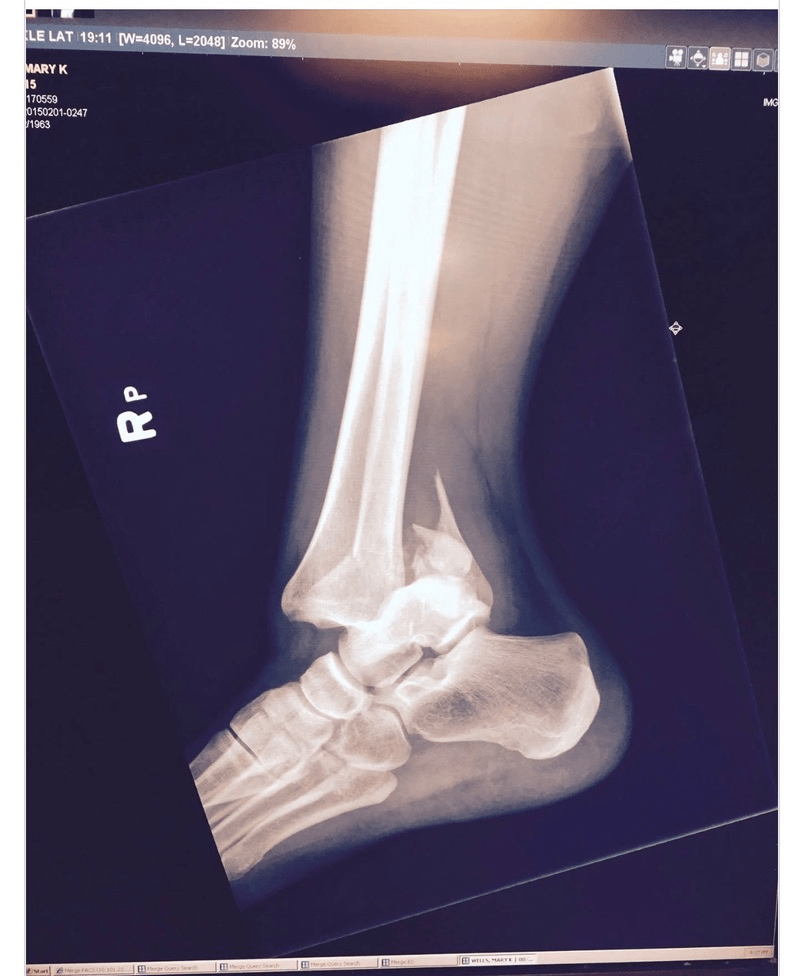
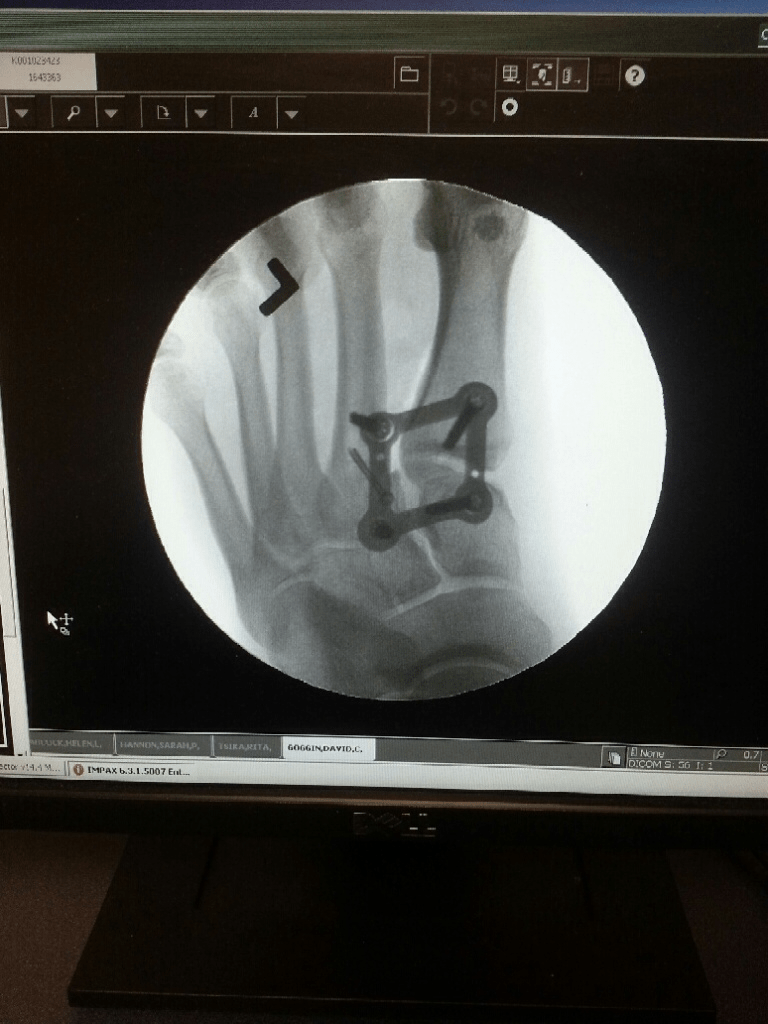
Pt is a 17 y/o female that presents to the clinic with left foot pain x1 year. Pt injured herself in a volleyball game a year prior but her foot did not heal. What clinical condition is shown on this xray and where?
Bonus Points: How was it treated?
Enchondroma on the 5th Metatarsal
Surgical repair with a cadaver bone
 Image and Clinical case Creds:
Image and Clinical case Creds:
400
A 16 y/o male presents to his PCP office with knee pain x3 months, Pt does cross country at school and reports he hasnt been able to run as far. Pt was prescribed PT wit quad strengthening with good effect. What complications could he get from this condition?
Double jeopardy: What condition presents very similarly but at a younger age?
Complications rare: could get avulsion fracture at tibial tubercle. (Osgood Schlatter Disease)
Sinding Larsen-Johansson (SLJS)-presents similar but complication is patellar sleeve fracture
500
This autoimmune disorder is caused by a lack of cohesion between keratinocytes at the suprabasilar level causing oral and other mucous membrane erosions.
What antibody is associated with this condition?
IgG
Pemphigus Vulgaris
500
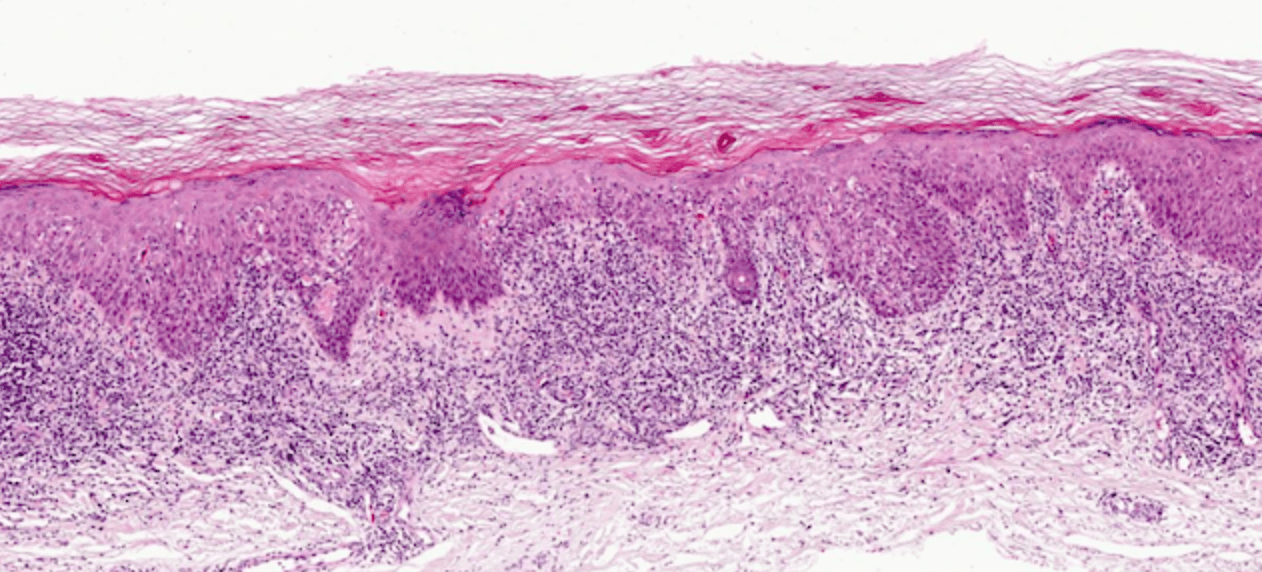
A 67 y/o male presents to clinic with well demarcated rough scaly plaque on his forehead and arm. A biospy was performed and the histology slide is shown below.
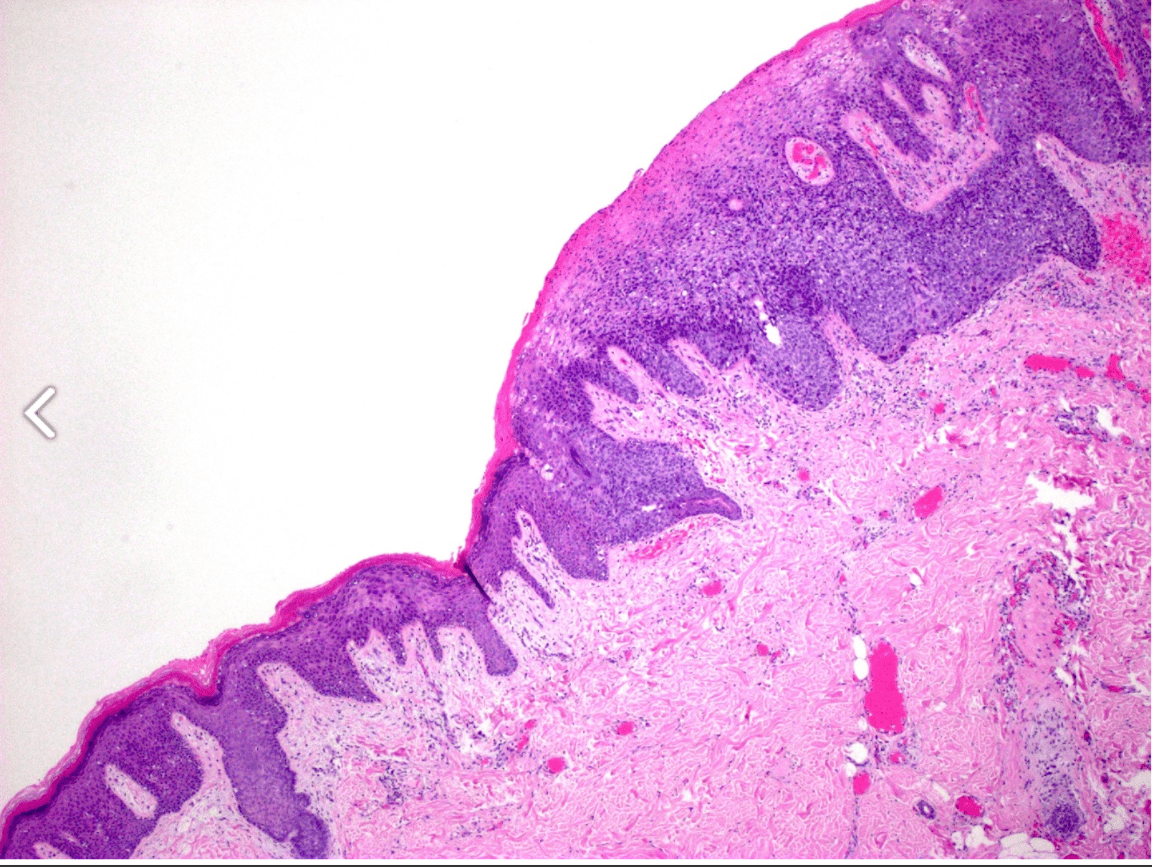
What is his diagnosis?
SCC in situ i.e Bowen's disease
can look very similar to psoriasis and tinea.
500
This potentially fatal hypersensitivity reaction occurs 4-6 weeks most commonly after taking which medications.
aromatic anticonvulsants: phenobarbital, phenytoin, and carbamazapine
DRESS (Drug rash eosinophilia and systemic symptoms)
500
This condition presents only in males with the following symptom known as scaling skin disorder. 
What two other clinical manifestation are associated with this condition?
Double Jeopardy: Name the condition
Cryptorchidism and corneal opacity
X linked recessive Ichthyosis
(abnormal steroid sulfatase)
500
This condition is associated with lower respiratory tract infections, glomerulonephritis and a presence of P-ANCA.
Microscopic polyangiitis (MPA)
necrotizing vasculitis without granuloma
500
Pt is a 17 y/o male presenting to emergency room after a fall after a dirt bike. This image is post surgical repair of the foot. What anterior nerve could be damaged from this type of injury
 Bonus: What major anterior tendon would be disrupted?
Bonus: What major anterior tendon would be disrupted?
Deep Fibular Nerve
Extensor Hallucis Longus Tendon (major flexor of toe)
Muscle: Extensor Hallucis Brevis
Image Creds: My brother Dave
500
Draw out brachial plexus
An injury to which level would cause the arm to hang by the side, medially rotated and extended and protonated.
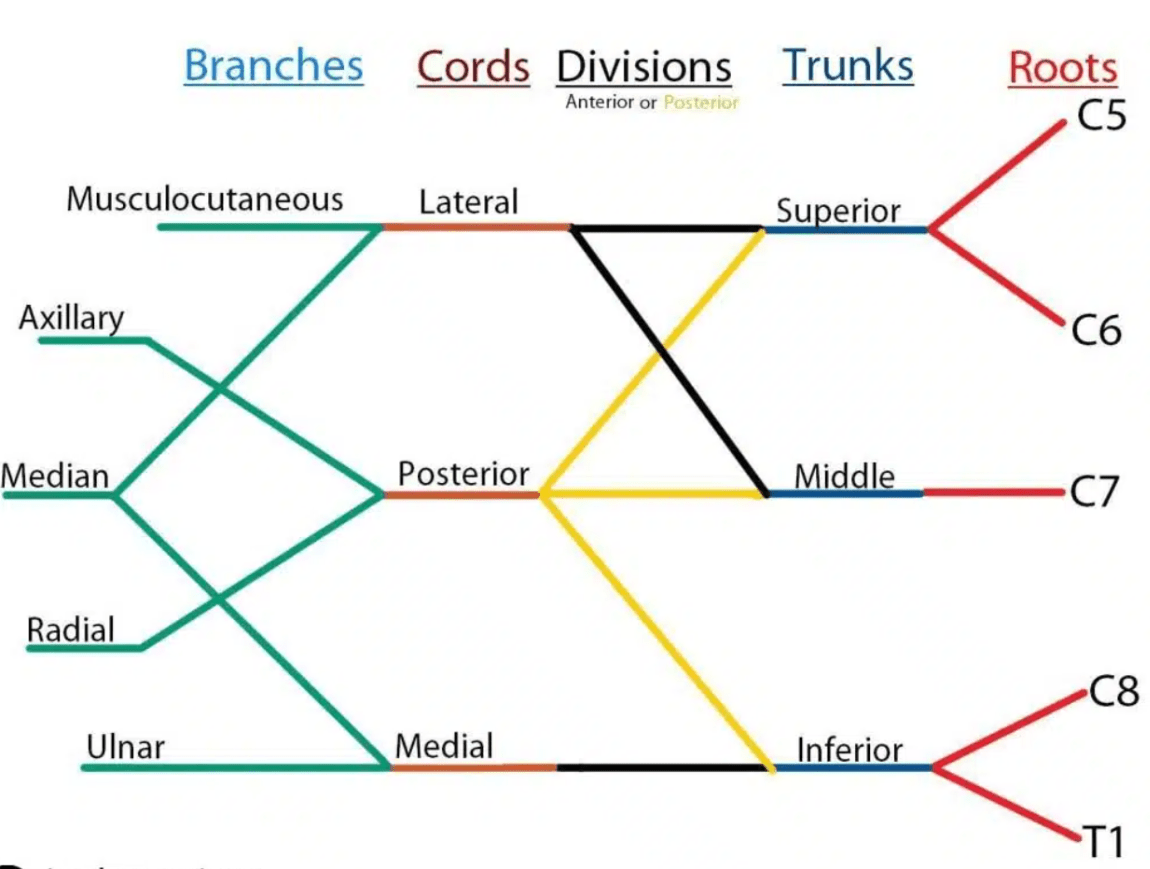
Injury to upper trunk; i.e C5-C6 roots
AKA Erb Palsy