A
B
C
D
100
A 59-year-old man is evaluated for an increased serum creatinine level. He has hypertension. He reports no changes to his medication regimen (lisinopril) during the past year.
On physical examination, the patient is afebrile, blood pressure is 145/92 mm Hg, and pulse rate is 84/min. He has no alopecia, rash, or joint abnormalities. Cardiopulmonary examination is unremarkable.
Laboratory studies:
Creatinine (repeat specimen)
1.5 mg/dL (133 µmol/L)
H
Yesterday
1.3 mg/dL (115 µmol/L)
6 months ago
0.9 mg/dL (79.6 µmol/L)
Urinalysis
1+ protein
Results of a complete blood count are normal.
Ultrasound reveals normal-sized kidneys with increased echogenicity but no hydronephrosis.
Discontinue lisinopril and repeat serum creatinine measurement in 7 to 10 days
Obtain a 24-hour creatinine clearance
Perform iothalamate glomerular filtration rate scan
Schedule a kidney biopsy
100
A 50-year-old man is evaluated during a routine health examination. He has type 2 diabetes mellitus. Medications are metformin and semaglutide.
Physical examination findings, including vital signs, are normal.
Serum electrolyte levels and kidney function are normal.
Which of the following is the most appropriate screening test to perform next?
24-Hour urine protein excretion
Spot urine albumin
Urinalysis
Urine albumin-creatinine ratio
100
A 35-year-old woman is evaluated in the emergency department for a 1-day history of severe colicky flank pain radiating to the groin and hematuria. She has no other medical problems. Her only medication is a daily multivitamin.
On physical examination, pulse rate is 110/min; other vital signs are normal. The patient appears uncomfortable. Right-sided costovertebral angle tenderness is present. The remainder of the examination is unremarkable.
Laboratory studies:
Leukocyte count
9800/µL (9.8 × 109/L)
Creatinine
0.9 mg/dL (79.6 µmol/L)
Urinalysis
pH 7.0; 11-25 erythrocytes/hpf; no leukocytes
A noncontrast CT scan shows a 3-mm right kidney stone.
In addition to fluids, which of the following is the most appropriate treatment?
Allopurinol
Ketorolac
Morphine
Potassium citrate
Trimethoprim-sulfamethoxazole
100
A 67-year-old woman is evaluated during a follow-up visit 2 weeks after being diagnosed with minimal change disease by kidney biopsy. Since that time, she has had a 2.3-kg (5.0-lb) weight gain, worsening edema of the hands and lower extremities, and persistent periorbital edema. Medications are prednisone, high-dose furosemide, losartan, atorvastatin, calcium carbonate, and vitamin D.
On physical examination, vital signs are normal. The patient weighs 65.0 kg (143.3 lb). There is no ascites. There is 3-mm pitting edema to the thighs bilaterally, equal on both sides.
Laboratory studies:
Albumin
2.3 g/dL (23 g/L)
L
Creatinine
0.6 mg/dL (53.0 µmol/L)
L
Sodium
141 mEq/L (141 mmol/L)
Potassium
4.0 mEq/L (4.0 mmol/L)
Bicarbonate
24 mEq/L (24 mmol/L)
Urinalysis
3+ protein, no blood
Urine protein-creatinine ratio
8000 mg/g
Which of the following is the most appropriate management?
Intravenous albumin
Intravenous furosemide
Oral acetazolamide
Oral metolazone
200
A 54-year-old woman is evaluated for daily fatigue, decreased appetite, and lack of enjoyment in her usual life activities during the past several months. She has end-stage kidney disease due to hypertension and for the last 5 years has attended all hemodialysis sessions, maintained her job, and exceeded her monthly dialysis clearance targets. Her arteriovenous fistula is well functioning. She has not had any recent life or medication changes. She previously enjoyed a fitness class but has stopped attending. She spends most of each weekend sleeping. She feels sad and wonders if she should stop dialysis. Medications are amlodipine, lisinopril, metoprolol, sevelamer carbonate, calcitriol, and erythropoietin.
Physical examination findings, including vital signs, are unremarkable.
Laboratory studies:
Hemoglobin
10.5 g/dL (105 g/L)
L
Calcium
8.2 mg/dL (2.1 mmol/L)
L
Potassium
4.7 mEq/L (4.7 mmol/L)
Bicarbonate
24 mEq/L (24 mmol/L)
Phosphorus
4.2 mg/dL (1.36 mmol/L)
Parathyroid hormone
65 pg/mL (65 ng/L)
Increase erythropoietin-stimulating agent
Refer to hospice
Start sertraline
200
A 65-year-old man is evaluated during a routine follow-up visit 1 month after starting empagliflozin. He reports lower back pain, for which he has been taking celecoxib. Medical history is significant for well-controlled type 2 diabetes mellitus, hypertension, heart failure with reduced ejection fraction, and hyperlipidemia. Other medications are insulin glargine, insulin lispro, carvedilol, valsartan-sacubitril, and atorvastatin.
Physical examination findings, including vital signs, are unremarkable.
Laboratory studies:
Creatinine
1.4 mg/dL (123.8 µmol/L)
H
3 months ago
0.9 mg/dL (79.6 µmol/L)
Potassium
5.0 mEq/L (5.0 mmol/L)
Urinalysis
Specific gravity 1.010; 2+ protein; no blood, leukocyte esterase, or nitrites
Which of the following medications should be discontinued first?
Atorvastatin
Celecoxib
Empagliflozin
Valsartan-sacubitril
200
A 19-year-old woman is evaluated during a new patient visit. She reports minor muscle weakness with occasional muscle cramps and states that these symptoms are worse some days than others. Her pediatric medical record notes chronic hypokalemia and hypotension. Family history is significant for hypokalemia. Her medical history is otherwise unremarkable, and she takes no medications.
On physical examination, blood pressure is 85/60 mm Hg, and pulse rate is 88/min. BMI is 21. Mucous membranes are moist. Skin turgor is normal. The remainder of the examination is unremarkable.
Laboratory studies:
Electrolytes
Sodium
140 mEq/L (140 mmol/L)
Potassium
3.0 mEq/L (3.0 mmol/L)
L
Chloride
100 mEq/L (100 mmol/L)
Bicarbonate
30 mEq/L (30 mmol/L)
H
24-Hour urine studies
Sodium
350 mEq/24 h (350 mmol/24 h)
Potassium
260 mEq/24 h (260 mmol/24 h)
Chloride
400 mEq/24 h (400 mmol/24 h)
Urine calcium
40 mg/24 h (1.0 mmol/24 h)
L
Which of the following is the most likely diagnosis?
Bartter syndrome
Gitelman syndrome
Gordon syndrome
Liddle syndrome
200
A 20-year-old woman is evaluated for a 3-day history of bilateral eye pain and blurry vision. She also reports subjective fever, headache, a 3.6-kg (8.0-lb) weight loss, and body aches during the past 2 weeks. Three weeks ago, she was treated with amoxicillin for an upper respiratory infection. She reports no sick contacts. She has no other medical problems and takes no medications.
On physical examination, blood pressure is 148/96 mm Hg; other vital signs are normal. Bilateral conjunctival injection is noted. The remainder of the examination is normal.
Laboratory studies:
Hemoglobin
11 g/dL (110 g/L)
L
Alanine aminotransferase
58 U/L
H
Aspartate aminotransferase
70 U/mL
H
C-reactive protein
5.0 mg/dL (50 mg/L)
H
Creatinine
2.8 mg/dL (247.5 µmol/L)
H
Rheumatoid factor
80 U/mL (80 kU/L)
H
Urinalysis
Specific gravity 1.010; trace protein; no blood or nitrites; positive leukocyte esterase; 5-10 leukocytes/hpf
Which of the following is the most likely diagnosis?
Acute tubular necrosis
Pauci-immune vasculitis
Postinfectious glomerulonephritis
Tubulointerstitial nephritis with uveitis
300
A 32-year-old woman is evaluated during a routine follow-up examination for migraine and hypertension. She is asymptomatic. She has no other medical conditions. Medications are topiramate, sumatriptan, and lisinopril.
Physical examination, including vital signs, are normal.
Laboratory studies:
Blood urea nitrogen
8 mg/dL (2.9 mmol/L)
Creatinine
0.7 mg/dL (61.9 µmol/L)
Electrolytes
Sodium
136 mEq/L (136 mmol/L)
Potassium
3 mEq/L (3 mmol/L)
L
Chloride
112 mEq/L (112 mmol/L)
H
Bicarbonate
16 mEq/L (16 mmol/L)
L
Urinalysis
Specific gravity 1.005; pH 5.0; no blood, protein, leukocyte esterase, glucose, or ketones
Which of the following is the most appropriate next step in management?
Discontinue lisinopril and start amlodipine
Discontinue topiramate and start venlafaxine
Measure serum aldosterone
Measure urine anion gap
Screen for laxative abuse
300
A 78-year-old man is evaluated during a follow-up visit for hypertension. He is asymptomatic. Medical history includes type 2 diabetes mellitus, hypertension, coronary artery disease, osteoarthritis, and stage G4 chronic kidney disease. Medications are carvedilol, lisinopril, hydrochlorothiazide, empagliflozin, and aspirin. He lives independently.
On physical examination, blood pressure is 138/84 mm Hg, and pulse rate is 64/min. The remainder of the examination is unremarkable.
Which of the following is the most appropriate management for this patient's hypertension?
Adjust medications to target a systolic blood pressure <130 mm Hg
Discontinue hydrochlorothiazide
Shared decision making
Continue current management
300
A 28-year-old woman is evaluated for a blood pressure reading of 148/90 mm Hg measured at a recent work health screening event. Previous office blood pressure measurements have been normal. There is no family history of hypertension. She has no other medical problems and takes no medications.
On physical examination, blood pressure is 150/94 mm Hg, and pulse rate is 75/min. An abdominal bruit that lateralizes to the left side is present. The remainder of the examination is unremarkable.
Serum creatinine and electrolyte levels are normal. Urinalysis findings are normal.
Which of the following is the most appropriate diagnostic test to perform next?
Captopril renal scintigraphy
Plasma renin activity measurement
Renal artery CT angiography
Renal duplex Doppler ultrasonography
300
A 39-year-old man is evaluated for hypertension, proteinuria and elevated serum creatinine level, and a painful rash, as shown. Results of hepatitis C virus testing are positive.

Which of the following is the most likely diagnosis?
Cryoglobulinemia
Infection-related glomerulonephritis
Monoclonal gammopathy of renal significance
Systemic lupus erythematosus
400
A 28-year-old woman is evaluated for persistent microscopic hematuria without proteinuria. Family history is significant for end-stage kidney disease in her older brother, who underwent kidney transplantation at age 32 years, and in a maternal uncle, who started dialysis at age 30 years and underwent kidney transplantation. Her mother has microscopic hematuria but normal kidney function. Her younger brother and older sister have no known kidney abnormalities. The patient has no other symptoms or medical conditions and takes no medications.
Physical examination findings, including vital signs, are normal.
Laboratory studies:
Creatinine
0.7 mg/dL (61.9 µmol/L)
Urinalysis
2+ blood; no protein, leukocytes, or leukocyte esterase; and 10-20 erythrocytes/hpf
Kidney ultrasound shows normal-sized, echogenic kidneys with no cysts, masses, or stones.
Which of the following is the most appropriate diagnostic test to perform next?
Genetic testing
24-Hour urine collection
Kidney biopsy
Skin biopsy
400
An 18-year-old man is evaluated for a second episode of nephrolithiasis.
Urinalysis results are shown.
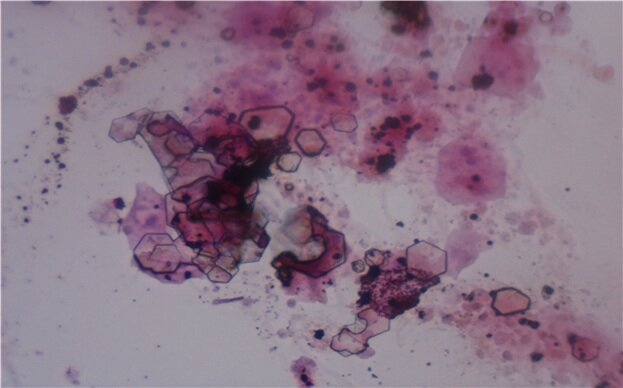
Which of the following is the most likely composition of this patient's kidney stones?
Calcium
Cystine
Struvite
Uric acid
400
A 33-year-old woman is evaluated during a prenatal visit. She is at 12 weeks' gestation. Home blood pressure measurements have averaged 150 to 160/85 to 95 mm Hg. She is asymptomatic. She has obesity but no other medical problems. Her only medication is a prenatal vitamin.
On physical examination, blood pressure is 150/95 mm Hg. She has a gravid uterus. The remainder of the examination is unremarkable.
Laboratory studies:
Urine protein-creatinine ratio
200 mg/g
H
Urinalysis
1+ protein; no erythrocytes or leukocytes
Which of the following is the most appropriate management?
Intravenous labetalol
Oral chlorthalidone
Oral lisinopril
Oral nifedipine
400
A 54-year-old man is evaluated during a follow-up visit for elevated blood pressure (BP). One month ago, he had an office BP measurement of 160/94 mm Hg. Subsequently, 24-hour ambulatory BP monitoring revealed an average BP of 152/92 mm Hg. He is asymptomatic. He smokes 10 cigarettes daily. There is no family history of hypertension. He has dyslipidemia and takes rosuvastatin.
On physical examination, BP is 158/94 mm Hg and pulse rate is 78/min. Other vital signs and the remainder of the examination are normal.
Serum creatinine, electrolyte, glucose, and thyroid-stimulating hormone levels are normal. Urinalysis findings and urine albumin-creatinine ratio are normal.
A 12-lead ECG is normal.
In addition to lifestyle modifications, which of the following is the most appropriate treatment?
Amlodipine-benazepril
Chlorthalidone
Metoprolol-hydrochlorothiazide
Nifedipine