"Eye" wanna pass my boards!
Global Warning
Grow some thicker skin
Dirty Bits
Hodgepodge
100

Dx and tx?
Dx: Hordeolum
Tx: Warm compress
100

8yr old boy bit by this snake 30 mins pta. Tx?
Answer: assurance, ensure tdap utd. King vs Coral


100

Mildly pruritic rash x 2 weeks, Dx?
Dx: Pityriasis Rosea
-Self limited
-4 to 8 wks
-May be preceded by flu-like prodrome
-Herald Patch/Xmas tree pattern
-Tx w antihistamines
100

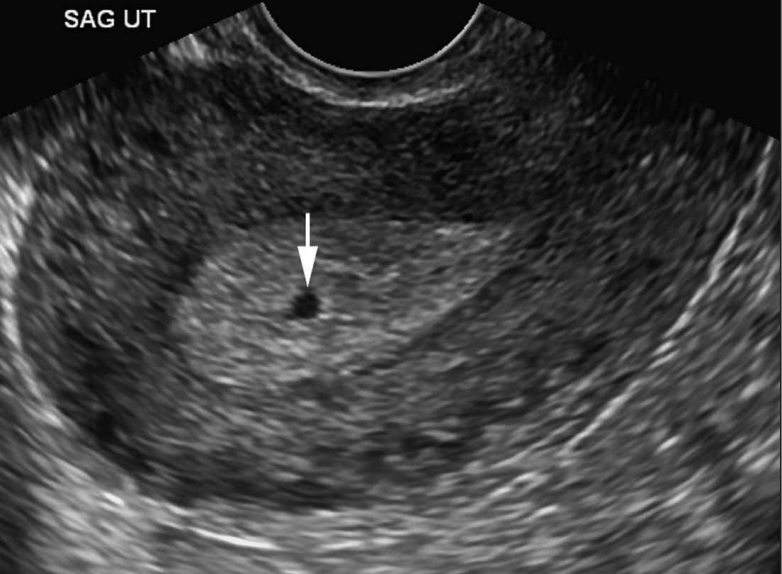
24yr female G1P0, 8 weeks intractable vomiting and spotting. HCG 125,000 mlU/mL. What is Dx?
Dx: Molar Pregnancy
-Abdominal pain and hyperemesis.
-HCG >expected
-Preeclampsia <24 wks
-Passage of grapelike clusters
-Uterus large for dates
-US: snowstorm appearance
100
6yr old with vomiting and diarrheax 1wk. Tx w abx. Stool initially watery, now bloody. Child ill appearing. Labs demonstrate wbc 8K, plt count 90K, BUN 35, Cr 1.6. Dx?
HUS: Hemolytic Uremic Syndrome
E coli 0157:H7
MAHA
+/- Fever
Anemia
Thrombocytopenia
AKI
200
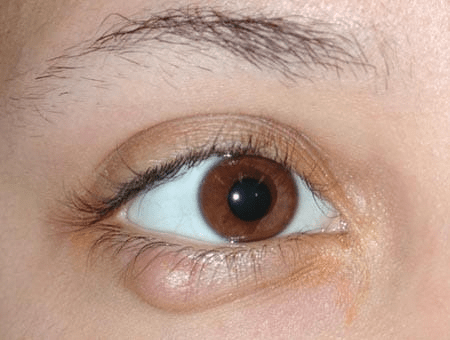
This painless condition is caused by subacute or chronic inflammaiton of the meibomian gland
Chalazion
200
Most common type of arrhythmia associated with following electrical injuries:
AC?
DC?
AC: V Fib
-household and commercial; explosive exit wounds; worse effects; tetanic contractures prolonged exposure
DC: Asystole
-industrial/batteries; discrete exit wounds
*High voltage >1000 Volts
200

Dx? Cause? Tx?
Dx: Impetigo
Cause: S aureus or Strep
Tx: Cephalexin vs Mupirocin
*Highly contagious. Nonbullous vs Bullous
200

Dx and Tx?
Tx: reduction; if unable then dorsal slit
-Paraphymosis: inability to pull retracted foreskin over glans. EMERGENCY- call paramedics
-Phymosis: inability to retract foreskin
200
20 yr old syncope during soccer. Expected physical exam finding?
a) Triphasic pericardial friction rub
b) Systolic murmur that increases w Valsalva
c) Systolic murmur that decreases with standing
d) Hyperthermia and profuse diaphoresis
b) SEM inc w standing or valsalva
-dec with squatting
300
3 common causes of acute painless monocular vision loss
-retinal detachement
-CRAO
-CRVO
300

4 yr old boy bites household electrical cord and sustains burn to corner of mouth. What is potential complication?
Electrical lip burn.
Do not debride. Cleanse and apply petroleum-based abx ointment. Observe closely and refer to plastic or oral surgeon.
Complications include delayed hemorrhage from labial artery (10-15% pts) 3-14 days after injury when escar separates.
300

68yr old painful rash x 7 days. Dx? Management (be specific)?
Dx: Herpes Zoster (Shingles)
Management:
-Stain eye to rule out HZO!!
-Tx with: oral antivirals for immunocompetent pts. IV antivirals if immunocompromised or disseminated
-Steroids DO NOT decrease incidence of PHN
*Hutchinson Sign: V1, nasociliary, high likelihood ocular
*Ramsay Hunt Syndrome: Facial palsy (Bells) w vesicles in ear canal and pinna (VIII)
300
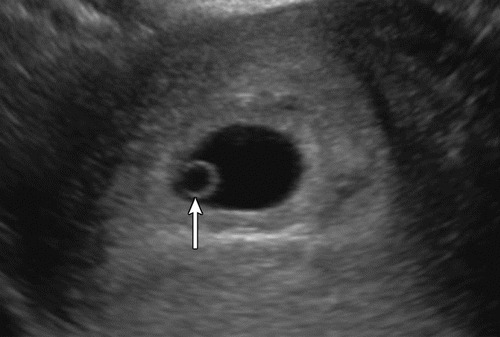
G2P1 5 wks by dates-abdom cramps and spotting. HCG 2,800. Hemodynamically stable. Dx and management?
Dx: First trimester vaginal bleeding
Management: Repeat HCG and US in 2 days. Rhogam?
300
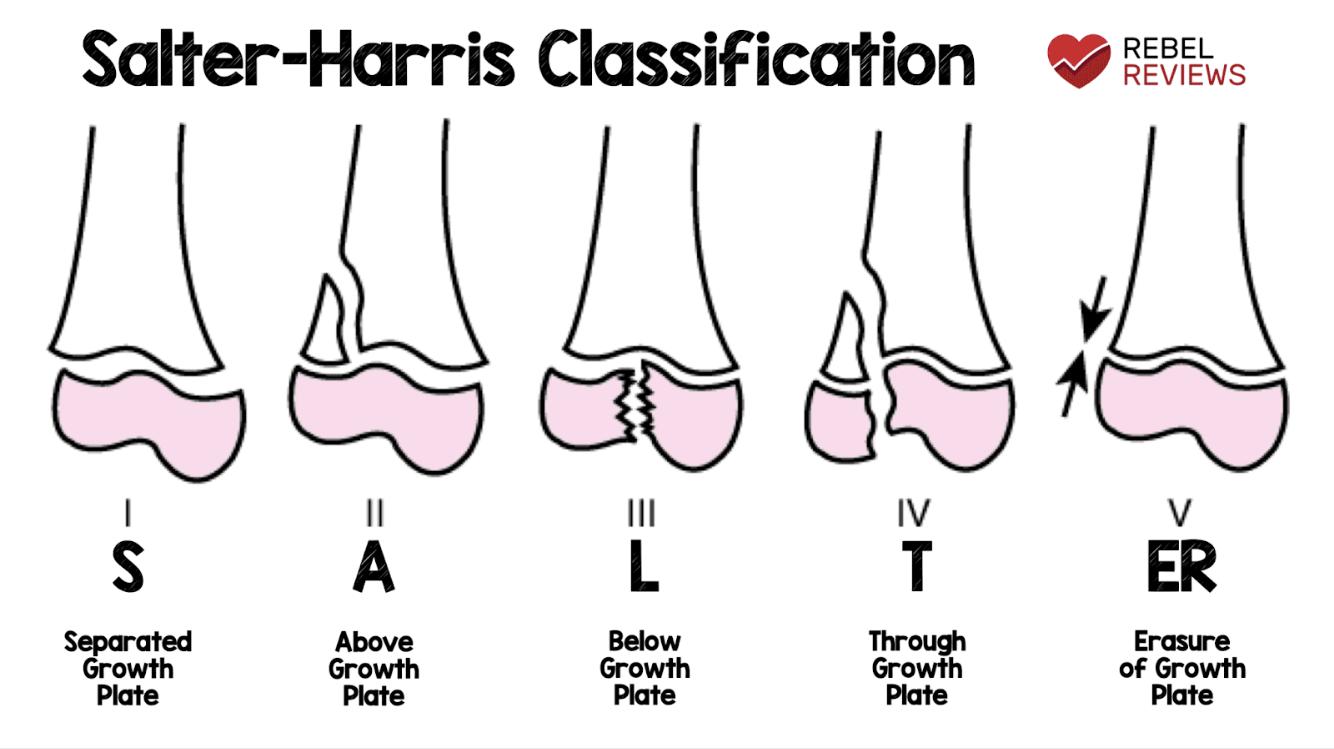
Describe the Salter-Harris Classification of epiphyseal fractures
400
 Pain, welling, redness x 5 days. Dec VA and pain w EOM's. Dx, etiology, and treatment?
Pain, welling, redness x 5 days. Dec VA and pain w EOM's. Dx, etiology, and treatment?
Orbital cellulitis 2/2 Staph, strep or H flu. Tx with iv abx (vanco + unasyn or vanc + rocephin/flagyl). Ophtalmology consult. Surgery if IOP>20
400
Dx and 3 Tx Modalities?
Dx: Osborne Wave 2/2 Hypothermia
Tx:
Passive External Rewarming
Active External Rewarming
Active Core Rewarming
Warm O2 (42 C)
Heated IVF (D5NS)
Lavage: gastric, bladder, thoracic
Extracorporeal: HD, CPB
400

18 month old with fever and rash x 48 hrs. Dx? Tx?
Dx: Staph Scalded Skin Syndrome
Tx: IV Abx (B lactamase/penicillinase resistant
PCN such as oxalacillin/nafcillin or first gen cephalosporin +/- vanco). No benefit with clinda. IV hydration similar to burn
*Exotoxin producing S aureus.
Mainly <6yrs. Tender erythema. Classic perioral then generalzied body w flaccid bullae <48 hrs. Minimal MM involvement. Nikolsky positive
400
Name 4 causes of genital ulcers
Syphilis (primary)-chancre
HSV
Chancroid-Haemophilius ducreyi
Lymphogranuloma Venereum-Chlamydia trachomatus
Granuloma Inguinale-Klebsiella granulomatis
Bechet syndrome
400

Name and describe this injury
**Monteggia Fx. Prox Ulna fx (prox ⅓) with radial head disslocation
Galeazzi Fx is fx of distal 1/3 of radius with dislocation of DRUJ
500

Sudden onset left sided headache and decreased vision w associated nausea/vomiting. Treatment ?
Prostaglandin analogs: Bimatoprost 0.03% 1 drop x 1
Topical B-blocker: 1 drop timolol 0.5%
Topical alpha agonist:1 drop apraclonidine 0.5%
Carbonic anhydrase inhibitor: acetazolamide 500mg po or iv
Mannitol 1-2gm/kg iv. **Topical pilocarpine 1-2%, no longer recommended in acute setting.
500

Diver unresponsive on surfacing. Dx and Tx?
Dx: Arterial Gas Embolism (pulmon, cardiac, cerebral)
Tx: ACLS and hyperbaric O2
Distinguish from DCS:
A. DCS 1
1) Cutaneous: skin bends
2) MSK: the bends; delayed and insidious (hrs/days)
B. DCS 2
1) Pulmon: chokes
2) CNS
500

52 yr old female recently tx with bactrim for uti. Developed fever malaise, myalgias, arthralgias followed by abrupt onset of blistering rash that involves 35% TBSA. Dx?
Dx: Toxic Epidermal Necrolysis (TEN)
SJS: <10% TBSA blistering plus widespread rash, MM involvement
SJS/TEN Overlap 10-30% blistering.
TEN >30% blistering
*Nikolsky positive
*NSAIDs, PCN, Sufla, Allopurinol
*D/C cause, supportive care, IVIG for TEN
500
Visibly pregnant woman presents to ED in cardiac arrest. Correct management of this pt includes:
Continue CPR on backboard, intubate, use ACLS drugs and protocols, place IO, resuscitative hysterotomy in 4 minutes.
Continue CPR w manual displacement of uterus, intubate, use ACLS drugs and protocols, place IO line, resuscitative hysterotomy in 4 minutes.
Continue CPR w manual displacement of uterus, intubate, avoid ACLS drugs, place a IO line, resuscitative hysterotomy in 4 minutes.
Continue CPR with backboard at 30deg tilt, intubate, use ACLS drugs and protocols, place IO line, resuscitative hysterotomy in 4 minutes.
2. Continue CPR w manual displacement of uterus, intubate, use ACLS drugs and protocols, place IO line, resuscitative hysterotomy in 4 minutes.
500

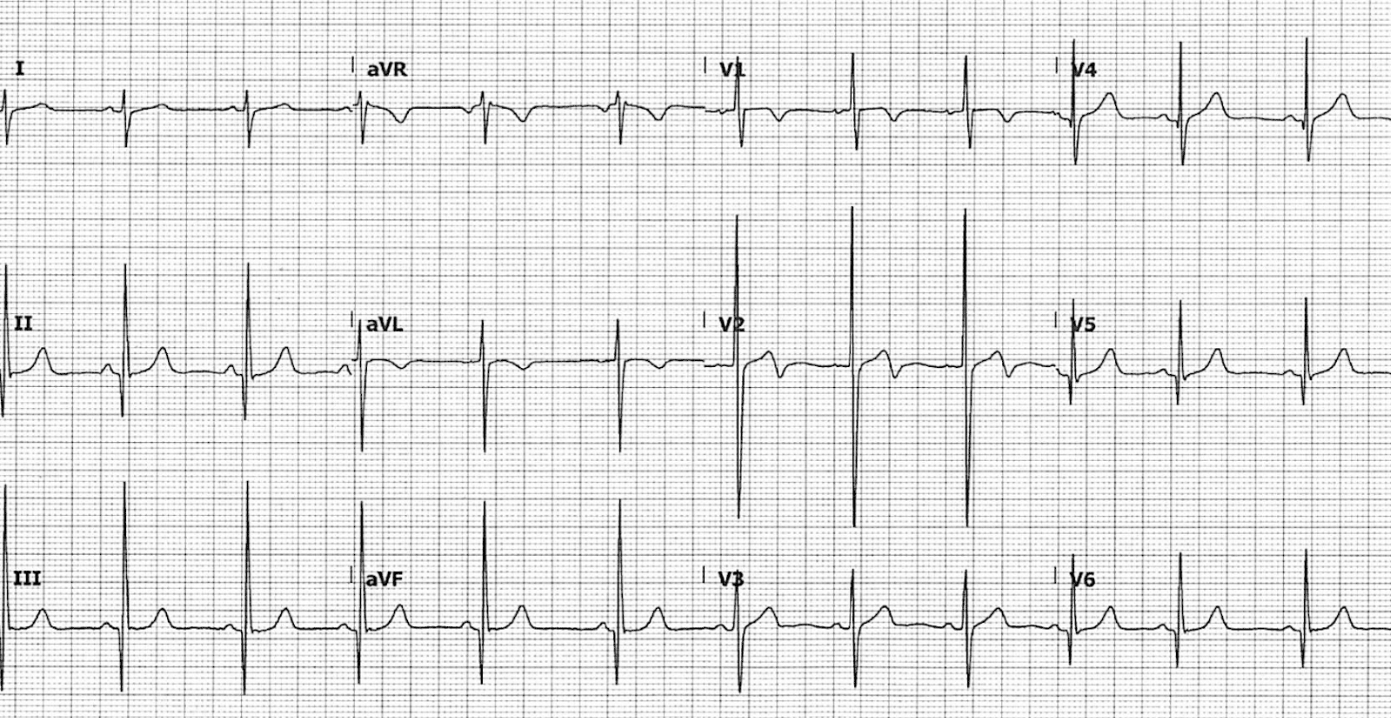
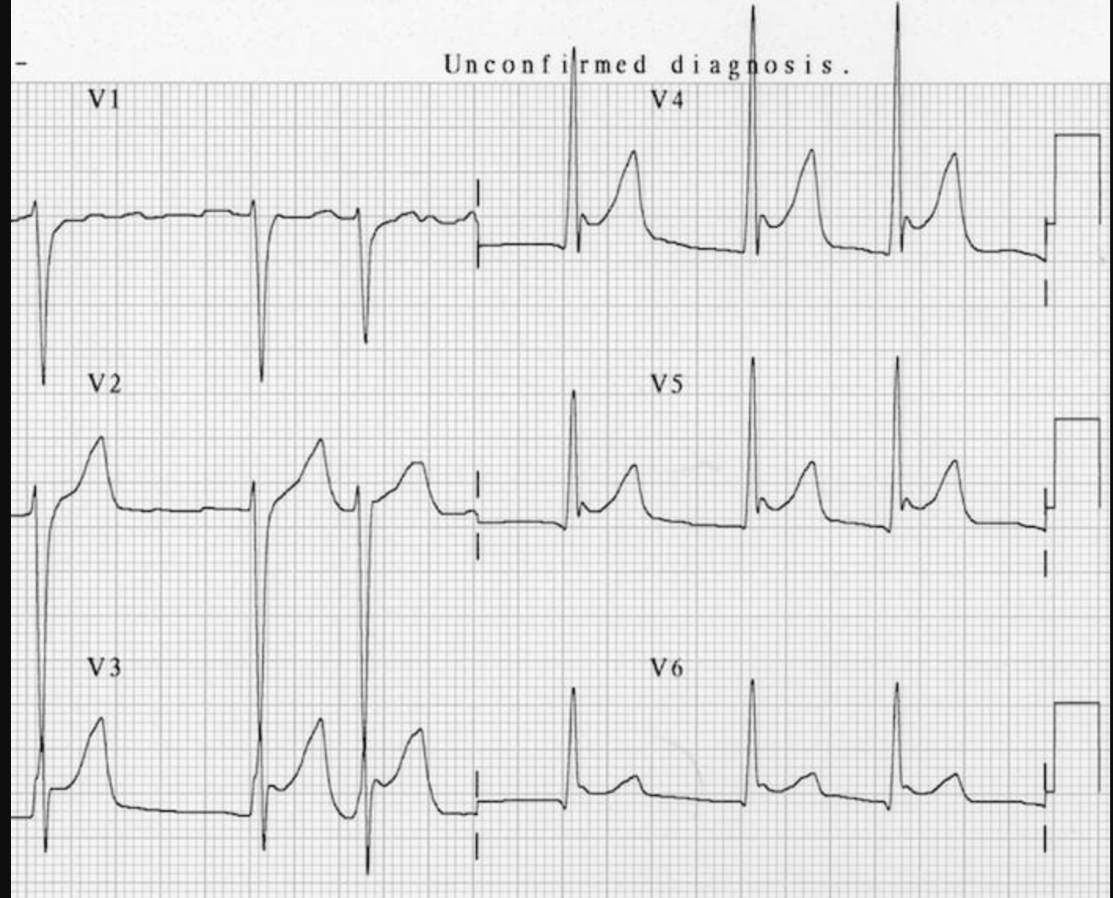
What does this indicate?
RV involvement. Careful with ntg.