Benign GYN
L&D
Oncology
Contraception
Miscellaneous
100
What is the differential for abnormal uterine bleeding?
What is PALM-COEIN?
Structural vs Non-Structural
Polyps, Adenomyosis, Leiomyomas, Malignancy, Hyperplasia
Coagulopathy, Ovulatory Dysfunction, Endometrial, Iatrogenic, Not otherwise classified
100
A history of cesarian delivery followed by fever, uterine tenderness, and foul-smelling lochia
Bonus: what kind of bacterial infection is this and what antibiotics should be started?
What is endometritis?
Polymicrobial infection both gram-positive (Staphylococcus epidermidis and group B streptococci) and gram-negative (Gardnerella vaginalis) bacteria.
Treat with clindamycin and gentamicin
100
You have a high suspicion that your patient has a primary ovarian malignancy, what is your next step in diagnosis, biopsy vs surgical excision?
- Surgical biopsy
- Recommended for definitive diagnosis of ovarian cancer
- Should be performed in patients with clinical, radiographic, and/or laboratory findings that suggest ovarian cancer
- Laparoscopic removal is the preferred surgical procedure.
Fine-needle aspiration is absolutely contraindicated in potentially resectable ovarian tumors because it can directly spread tumor cells to the peritoneum.
100
A 22-year-old woman with no medical history wants contraception that will also reduce her risk of sexually transmitted infections. What method do you recommend?
What is a condom?
100
A 2-day-old infant is noted to have a continuous machine-like murmur and bilateral hearing screen failure. On fundoscopic exam, the infant has lens opacities. The mother reports she had a low-grade fever and rash during her first trimester.
What is congenital rubella syndrome?
Additional buzzwords blueberry muffin rash, hepatosplenomegaly, jaundice, microcephaly
200
Name the type of incontinence:
1. detrusor overactivity which results in involuntary leakage of urine
2. impaired detrusor contractility leading frequent involuntary loss of urine
3. loss of urine with physical stress such as coughing, sneezing, and laughing caused by urethral hypermobility
1. Urge incontinence
2. Overflow incontinence
3. Stress incontinence
200
The criteria for preeclampsia:
What is new onset gestational hypertension with proteinuria or end organ dysfunction
*three primary features of PREeclampsia are Proteinuria, Rising blood pressure (hypertension), and End-organ dysfunction*
200
itchy, erythematous, scaly rash on the areola

What is Paget disease of the breast?
200
What are contraindications to combined oral contraceptive pills?
Current or recent history (≤ 5 years) of breast cancer
age >35 years old AND smoking > to 15 cigarettes a day
Known cardiovascular risk factors (previous stroke, ischemic heart disease, hypertension)
migraines with aura
200
The single most accurate method of estimating the gestational age in the first trimester
What is ultrasonographic measurement of crown-rump length (CRL)?
300
Define ectopic pregnancy and its risk factors.
Ectopic pregnancy is characterized by implantation of the fertilized ovum outside the uterus.
Symptoms: amenorrhea, enlarged uterus, and lower abdominal pain, with or without vaginal bleeding. Ectopic pregnancies have the potential to rupture and cause hemorrhagic shock.
Risk factors include: prior ectopic pregnancy, hx of infertility, PID, acute appendicitis, prior tubal surgery, smoking, and advanced maternal age.
Incidence: 1 in 100 pregnancies
300
What is the criteria for a reactive Nonstress Test (NST)?
≥ 2 fetal heart rate accelerations that last for at least 15 seconds and are > 15 bpm above the baseline within a 20-minute period
300
A nulliparous patient with a history of late-onset menopause presents with a tender, enlarged, and erythematous breast, nipple flattening, blood-tinged nipple discharge, and axillary lymphadenopathy
What is inflammatory breast cancer?

300
What options are there for emergency contraception?
Current or recent history (≤ 5 years) of breast cancer
age >35 years old AND smoking > to 15 cigarettes a day
Known cardiovascular risk factors (previous stroke, ischemic heart disease, hypertension)
migraines with aura
300
A 24-year-old woman presents with fever, headache, nausea, and vomiting. Exam reveals a diffuse erythematous macular rash involving the palms, soles, and inner thighs as well as mucosal hyperemia. Blood pressure is 80/50 mm Hg. She reports being on her menstrual period.
What is Toxic Shock Syndrome?
400
Episodic lower abdominal pain shortly before menstruation in an adolescent with a normal physical exam
What is primary dysmenorrhea?
The most common gynecological complaint among adolescent females. The condition is most likely caused by an increased production of endometrial prostaglandin (PG) F2α. PGF2α causes dysrhythmic uterine contractions and consequently abdominal pain and uterine ischemia. The accompanying symptoms of primary dysmenorrhea (e.g., headache, diarrhea, fatigue, nausea) are also believed to be mediated by PGF2α.
1st line treatment: NSAIDs
2nd line: OCPs (MOA --> suppress ovulation)
400
The sudden increase in labor pains, hemodynamic instability, loss of fetal station, fetal distress, and a decreased amplitude of uterine contractions.
Which feature is most specific for this diagnosis?
What is uterine rupture and loss of fetal station?
400
Patient presents with adnexal mass and pelvic pain, you are concerned for ovarian cancer, what tumor marker(s) should you order?
- CA-125 levels are elevated in ∼ 80% of malignant epithelial ovarian tumors (and in certain germ cell tumors).
- Premenopausal women: Elevated CA-125 may indicate a benign process (e.g., endometriosis, pregnancy, pelvic inflammatory disease).
- Postmenopausal women: Elevated CA-125 (> 35 U/mL) raises concern for malignancy.
- Additional tumor markers:
- Germ cell tumor markers:
- βhCG, AFP, LDH
- Granulosa cell tumor: inhibin
- Also can consider CEA and CA 19-9
- Germ cell tumor markers:
400
A 24-year-old woman, 3 months postpartum, is exclusively breastfeeding. She desires highly effective contraception and prefers not to take daily pills. She has no medical comorbidities. Which method is most appropriate?
What is a progestin-only method (e.g., implant or IUD)?
Estrogen-containing contraceptives are avoided <6 months postpartum in breastfeeding due to effects on milk supply and increased VTE risk.
400
Name the ligaments

What is (in clockwise order)
1. Ovarian ligament
2. Suspensory ligament
3. Broad ligament
4. Round ligament
5. Cardinal ligament
6. Uterosacral ligament
500
Patient presents complaining of vaginal discharge
Differential for infectious vulvovaginitis:

500
You have an HIV positive patient on L&D, at what viral load is a c-section indicated and what intrapartum medication should be given?
What is a viral load > 1,000 copies and intrapartum zidovudine is indicated to further reduce the risk of neonatal HIV infection.
500
This high-grade endometrial carcinoma subtype is not associated with unopposed estrogen exposure, often arises in atrophic endometrium, and is characterized histologically by papillary architecture, marked nuclear atypia, and psammoma bodies.
What is serous endometrial carcinoma?
500
A 39-year-old woman with a history of estrogen receptor–positive breast cancer treated 2 years ago seeks contraception. She has heavy, painful periods and desires long-term, highly effective contraception. Which method is contraindicated, and which method would be best?
Contraindicated: progestin-containing methods (systemic progestins can worsen breast cancer risk).
Best choice: copper IUD (safe in breast cancer, also provides long-term contraception).
500
Interpret this fetal heart tracing
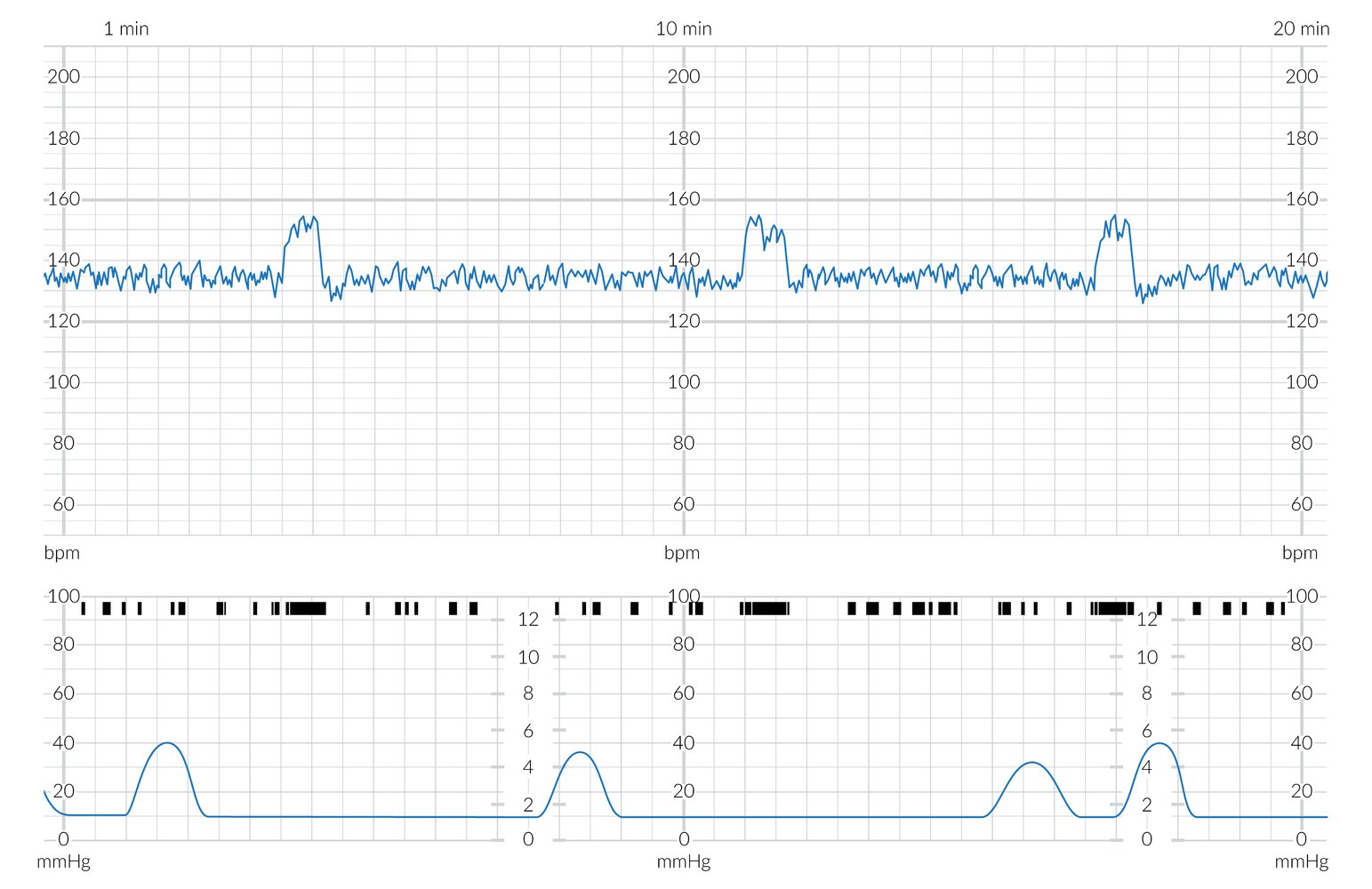
Normal findings

Baseline: 135 bpm
Variability: Moderate
Reactive?: Yes (2+ accels in 20 minutes)