Hemorrhagic
Neurogenic/Obstructive
Distributive
Endocrine
100
In patient presenting with hemorrhagic shock, which factor has highest association with increased mortality risk?
Presenting lactate of >8
Failure to correct lactic acidosis in first 24h
Volume of estimated blood loss at scene
Failure to correct lactic acidosis in first 24 hours
100
MAP goal for patients with proven neurogenic shock
> 85 mmHg
100
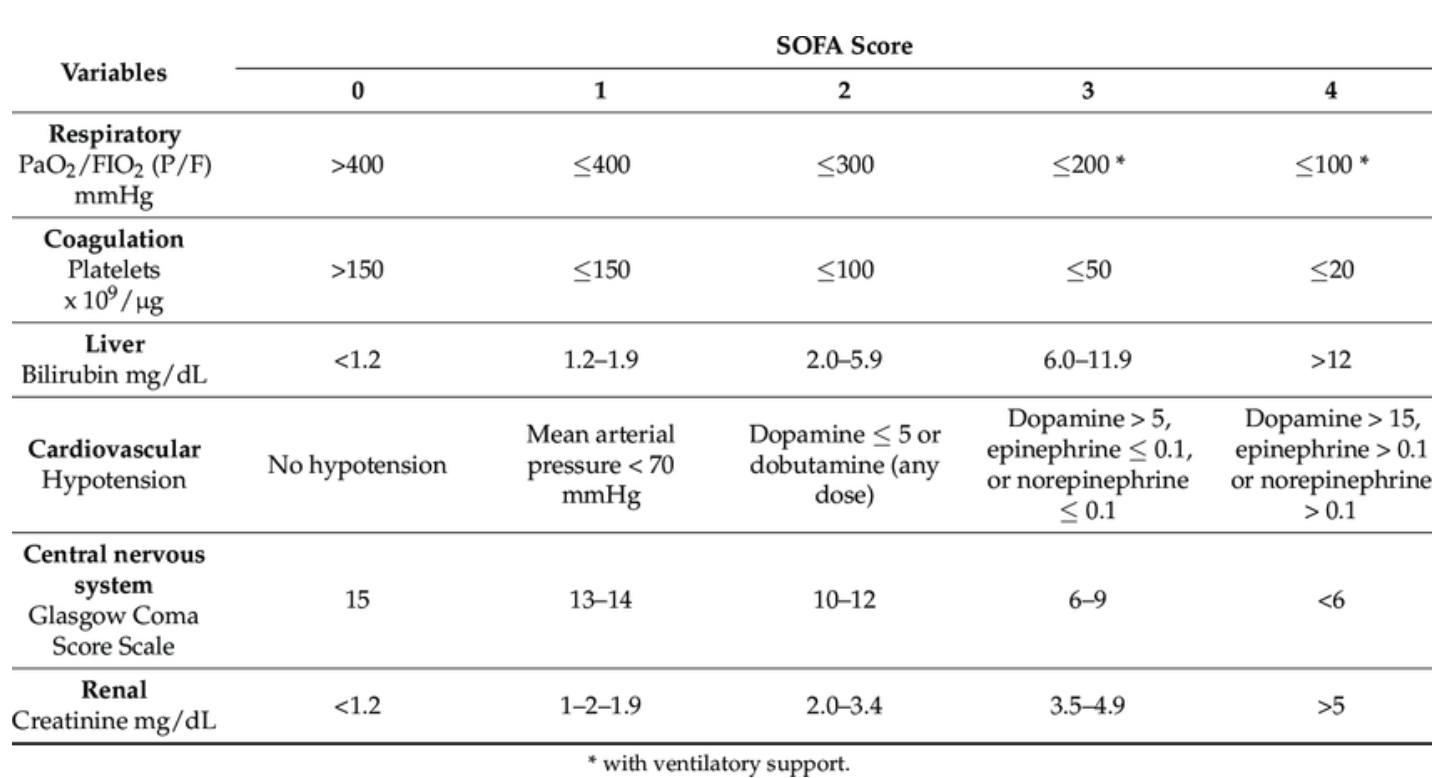
Scoring bedside assement tool used to predict poorer in-hospital outcomes in setting of sepsis/infection
SOFA/qSOFA
100
Name three effects of cortisol during stress response
gluconeogenesis, glycogen synthesis, protein synthesis inhibition, protein catabolism, and lipolysis; erythropoiesis; gastric acid stimulation; inhibiting vasopressin secretion and function; insomnia; and mediating catecholamine release
200
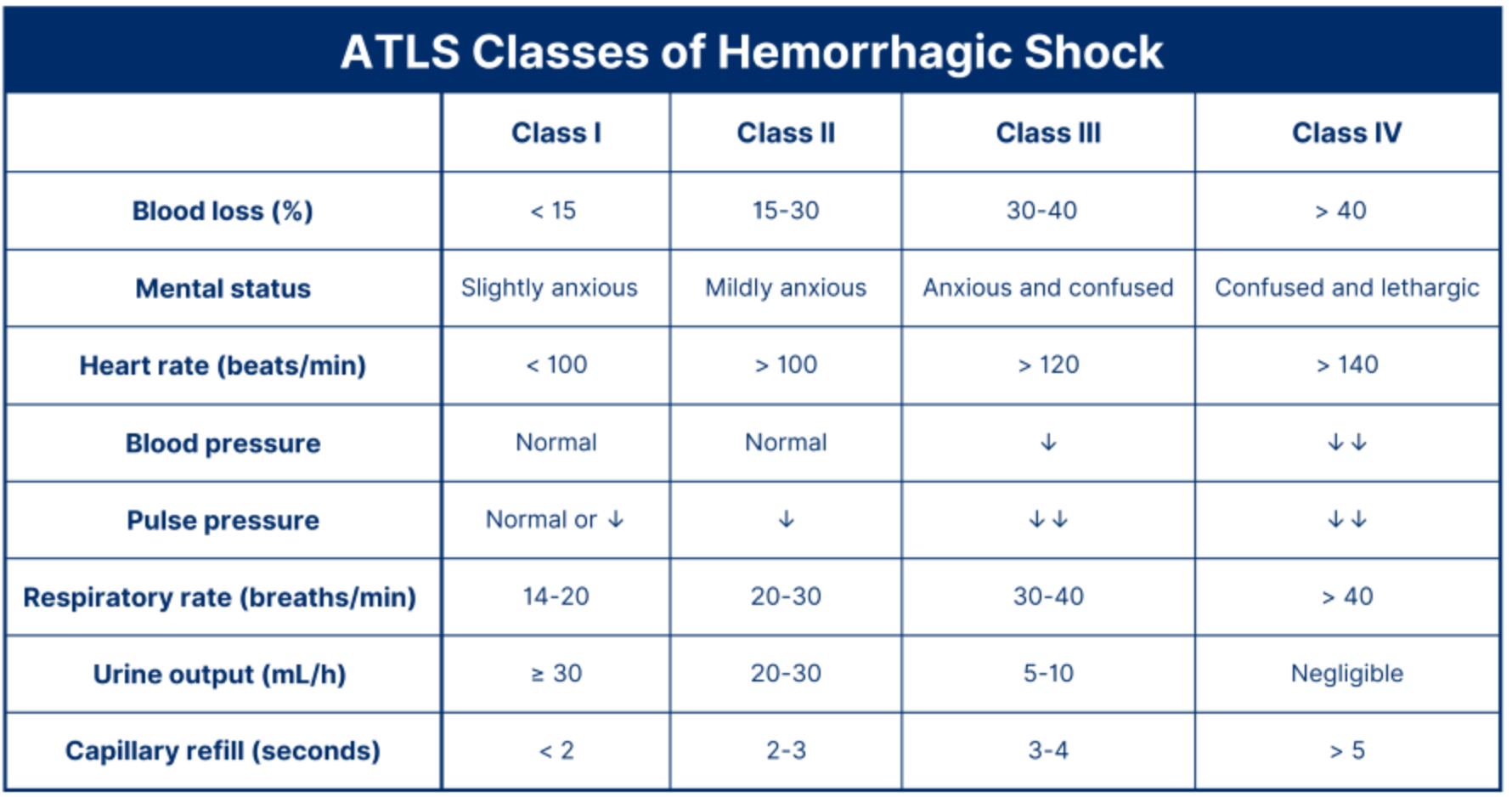
26 yo F in PACU following a C-section has a distended abdomen with sanguineous drainage from the wound site. BP is 86/58 mm Hg; HR is 126 bpm. She has cold clammy skin, and is anxious. She is suspected to have surgical site bleeding and is taken to the OR. What is her suspected percentage of blood volume loss?
30-40% blood volume loss
200
40 yo M presents to the ED after a motorcycle crash. He did not lose consciousness. On exam, he has bilateral lower extremity weakness and decreased sensation. His abdomen is distended, and he has midline thoracic spine tenderness. He is AOx3. BP is 80/50 mm Hg, and HR is 114 beats/min. What is the next step in management?
Fluid resuscitation
Hypotension in trauma patient = hypovolemia/hemorrhage until proven otherwise. Neurogenic/spinal shock consideration after initial resus
200
An adult women develops fever, rigors, and increased abdominal pain POD4 after colon resection. WBC count is 18,000, T 39.2°C, HR 130. She develops hypotension that does not respond to initial fluid resuscitation. She is started on vasopressors and admitted to the ICU. Which hemodynamic parameters is most consistent with the early stages of her condition?
(Decreased or increased) ___ SVR
(Decreased or increased) ___ Cardiac index
Decreased SVR, Increased CI (initially as cardiac function attempts to compensate for decreased venous return)
200
A patient with pmh of lupus undergoes laparoscopic colectomy. Post-op course is complicated by persistent hypotension and diffuse abdominal pain. What additional lab abnormalities support the diagnosis?
HypoNa, HyperK, Hypoglycemia, azotemia
300
A patient with penetrating trauma presents to ED with tachycardia, hypotension, obvious arterial bleeding from right upper extremity. Along with MTP and tourniquet application, what therapy should be given early in resuscitation efforts?
TXA - 1g within 3 hours of onset of bleeding, re-dose in 8 hours
300
33 yo F s/p fall has a CT that demonstrates a C5 burst fracture with associated epidural hematoma with spinal cord impingement. She has persistent hypotension and bradycardia, despite 3L given. Hgb is 13 g/dL. Of the choices listed here, which would be the best treatment?
Albumin, corticosteroids, pRBCs, surgical fixation, phenylephrine
Phenylephrine - useful in lower thoracic neurogenic shock for pure alpha activity after initial resuscitation with persistent hypotension
300
82 yo M presents perforated diverticulitis with retroperitoneal abscess. They are febrile, hypotensive, tachycardic, and hypothermic. Lab results show WBC count 25,000, hgb 11 g/dL, pH 7.25, and lactate 5 mg/dL. They remain hypotensive after aggressive crystalloid resuscitation. What is the next step in management?
Initiation of vasopressors to Maintain MAP > 65
Initiation of abx within 1 hours of sepsis recognition
(IR drainage/source control important, but MAP goal and abx should be first)
300
35-year-old man is admitted to the ICU for hemorrhagic pancreatitis. He is hypotensive with a mean arterial pressure in the 40s (mm Hg). His hemoglobin is 6.6, given 4 L of crystalloid and 1 unit of PRBCs. Repeat hemoglobin is 8. With persistent hypotension, he is started on norepinephrine and vasopressin, but this does not improve his BP. What is the most appropriate treatment?
IV hydrocortisone
400
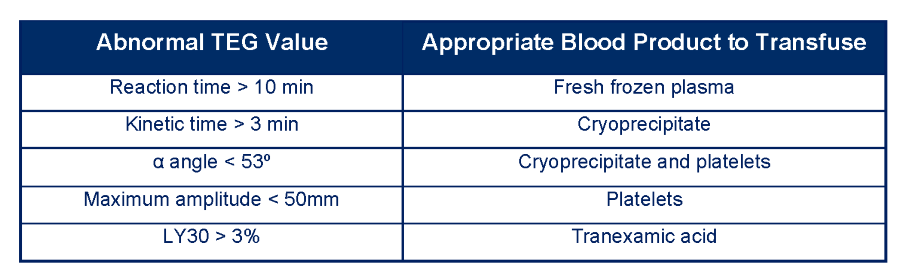
74 yo F is undergoing ex-lap following blunt trauma. She was hypotensive and tachycardic in the ED w/ positive FAST. In OR, TEG results are the following:
- Reaction time (R): prolonged
- Kinetics (K): decreased
- Angle (a): decreased
- Maximum amplitude (MA): decreased
- Lysis at 30 minutes (LY30): normal
Based on these results, in addition to hemorrhage control, what is the best resuscitative material to give?
Cryoprecipitate, platelets, and fresh frozen plasma
400
62 yo M presents to the ED with fevers, right upper abdominal pain, and jaundice. Temp 102.4ºF, HR is 118, BP is 95/58, RR is 18, and O2 saturation is 94% on RA. WBC is 22,000/µL, SCr 1.42 mg/dL, Plt 110,000, LA 3.2 mg/dL, Direct bili 2.8 mg/dL, AST 362 and AST 220, and alkaline phosphatase of 420. He is started on broad-spectrum antibiotics and IV fluids, but he remains hypotensive and becomes confused. Which hemodynamic profile is most consistent with this patient’s physiology?
CO __ HR ___ SVR ___ PAWP ___ MVO2 ___
Increased CO, increased HR, decreased SVR, normal PAWP, increased MVO2