Duchenne Muscular Dystrophy
Spinal Muscular Atrophy
Orthopedic Conditions
Spinal Conditions
Torticollis and Plagiocephaly
100
Primary Impairments, Activity Limitations, and Participation Restrictions
Primary Impairments: muscle weakness, may have cognitive impairment (most common in congenital forms)
Activity Limitations: walking, stairs, sports
Participation Restrictions: Navigating school/home environment
100
Pathology
Degeneration of anterior horn cells (spinal cord and brainstem
Atrophy and progressive weakness
Those with SMA lack SMN1 (produced full length SMN) gene, severity of disease depends on SMN2 (encodes small amount of protein) gene
100
Torsional Conditions
In-toeing: (concern after age 5 if > -5 deg)
Causes: femoral anteversion, internal tibial torsion, metatarsus adductus
Natural Progressions: tripping, pain
Out-toeing: (concern if >20 deg)
Causes: ER of hip, femoral retroversion (rare), external tibial torsion (can be from W-sitting), calcaneovalgus
Natural Progressions: pain, difficulty with gait
100
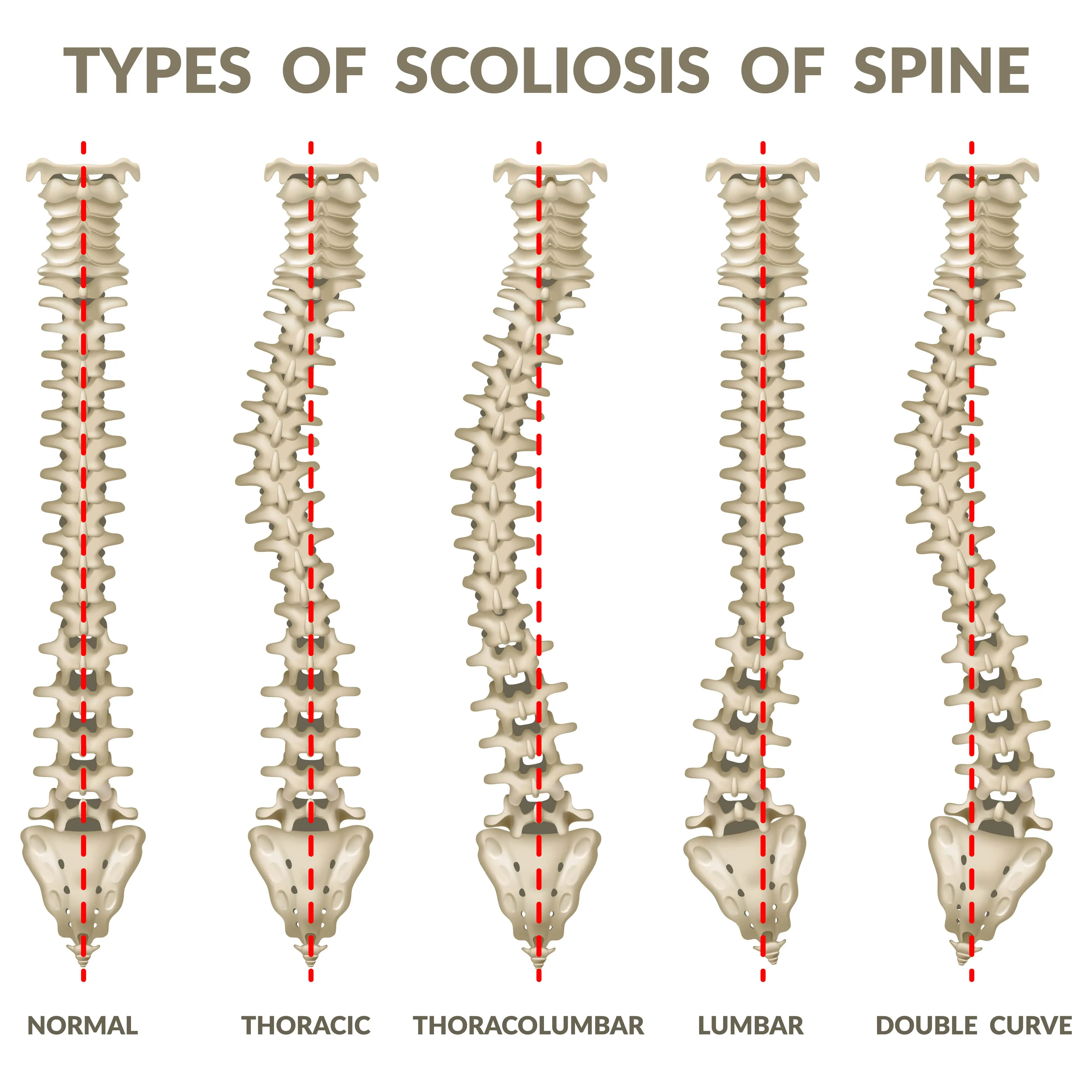
Definitions of Scoliosis + Clinical Exam
Idiopathic Scoliosis: coronal plane curvature with vertebral rotation; infantile -- birth - 3 years --> least common; juvenile -- 4-9 years; adolescent --10 years old - maturity --> most common
Neuromuscular Scoliosis: Associated with neuromuscular disease at any age, rapid progression
Congenital Scoliosis: vertebral anomolies durin in-uterp development, often coincid with other organ abnormalities, may lead to scoliosis, kyphosis, lordosis; may be stable or require surgery
Clinical Exam: Adam's forward bend test, postural assessment, leg length, x-rays (determines location, type, magnitude and skeletal age
100
Etiology and Pathophysiology
Etiology: Research inconclusive, likely multifactorial
Pathophysiology: unilateral shortening of SCM, cervical lateral flexion toward involved side, cervical rotation away from involved side
200
Medical Management Options
Gene Therapies: Dystrophin gene replacement, exon-skipping drugs (abnormal exon is removed and replaced with normal cells)
Pharmacological: Corticosteroids -- improve strength and pulmonary function, prolong walking up to 3 years; Creatine -- improve strength, endurance, and reduce stiffness
Surgery: tendon lengthening, spinal fusion
200
Types of SMA
SMA Type 1 -- Acute 60-70% of cases, onset 0-4 months old, recessive, rapidly progressive
SMA Type 2 -- Childhood onset, 20-30% of cases, onset 6-12 months old, recessive, slowly progressive
SMA Type 3 -- juvenile onset, 10-20% of cases, onset 1-10 years old, recessive, slowly progressive
200
Angular Conditions
Genu Valgum: (concern after age 7-8)
Causes: obesity, significant femoral anteversion, pathological (CP, OI, osteochondrodysplasia, Rickets, growth plate injury due to trauma, congenital hemimelia)
Progression: Anterior knee pain, pes planus, PTF instability, difficulty running
Genu Varum: (concern after age 4)
Causes: Congenital tibial hemimelia, osteochondrodysplasia, partial physeal arrest due to trauma, Rickets, tibial vara (Blount's disease), excessive prenatal fluoride ingestion
Progression: Fracture risk, pain
Normal Progression of knee angle:
Newborn --> moderate genu varum (expect this before 1 1/2 years)
1 1/2 - 2 years --> legs straight
2 1/2 years --> physiologic genu valgum (expect at this age)
4-6 years --> legs straight
200
How to Describe Scoliotic Curves
R vs L: described based on side of convexity
Location: described based on which vertebrae are primarily affected by curve
EXAMPLE
200
Common Presentations of Torticollis
Sternocleidomastoid Tumor: fibrotic mass in muscle belly (25-55% of cases) -- sometimes present bilaterally
Muscular Torticollis: No palpable tumor present, orthopedic concerns -- hip, foot/ankle, spine, postural asymmetries, functional/gross motor asymmetries, muscle imbalances, delayed motor milestones, cranial deformities (plagiocephaly)
Postural Torticollis: presents posturally as congenital Muscular Torticollis, but no SCM tumor or muscle tightness, causes can include -- postural asymmetry, asymmetrical muscle function, benign paroxysmal torticollis, congenital absence of 1+ cervical muscles or of transverse ligament, or contracture of other neck muscles
300
Timeline and Classifications of DMD
Timeline: Symptoms noticed around 3-5 years old --> walking lost 10-12 years old --> life expectancy up to the 3rd decade
Stage Classifications:
Early Ambulatory: diagnosis after delays in motor milestones noted
Transitional Late Ambulatory: some ability to walk -- gets more and more difficult -- increased muscle weakness and fatigue
Transitional Early Non-Ambulatory: lose ability to walk, wheelchair for mobility
Late Non-Ambulatory: Further decline in muscle function, can impact breathing and heart function
300
Expected Impairments, Activity Limitations, and Participation Restrictions
Expected Impairments: Weakness of proximal musculature (hands remain strong), difficulty breathing, sucking, swallowing, delayed milestones, impaired motor function, fatigue, spasticity, contractures, fractures, etc
Activity Limitations: Walking, stairs, sports
Participation Restrictions: Navigating school/home environments
300
Presentation and Bracing Options for Club Foot
Presentation: Forefoot adductus, hindfoot varus, ankle equinus, hypoplasia of the limb and small calf
Bracing/Surgical Options: Ponseti Method -- serial casing/bracing, corrects cavus deformity first, then equinus, most will then require achilles tenotomy followed by bracing, daily manipulations in French Method, complex surgery for rigid club foot; stretch the foot in eversion and DF directions (vertical and out)
300
Treatment Options for Idiopathic Scoliosis
Non-Surgical: serial casting --> short-term, early onset forms, orthotic devices --> most common treatment, curve 25-45 deg, wear 23 hours/day, prevents progression only, spinal orthoses -->TLSO, CTLSO, exercise, Schroth method
Surgical: posterior spinal fusion, -- for curves >45 deg, wait util near skeletal maturing to maximize growth and pulmonary development, growing rods available, acute PT - body mechanics education, log roll, transfers, gait, mobility
300
Grades of Severity of Torticollis
Grade 1: Early mild -- Age 0-6 months - ROM differences < 15 deg
Grade 2: Early Moderate -- 0-6 months - ROM difference 15-30 deg
Grade 3: Early Severe -- 0-6 months - ROM difference >30 deg (or with SCM mass)
Grade 4: Later Mild -- 7-9 months - ROM difference < 15 deg
Grade 5: Later Moderate -- 10-12 months - ROM difference < 15 deg
Grade 6: Later Severe -- 7-9 months - ROM difference 15-30 deg + OR 10-12 months with ROM difference 30 deg
Grade 7: Later Extreme -- 7-9 months with SCM mass OR 10-12 months - ROM difference 30 deg +, SCM mass
Grade 8: Very Late -- > 12 months, postural, muscle tightness, OR SCM mass
400
PT Management
Submaximal exercise and strength
If initiated early -- focus on abdominals, hip extensors, abductors, knee, extensors
Cycling, swimming, walking for early/transitional phases
Ask about dark urine following exercise
Standing activities 2-3 hours daily
Monitor strength
Contracture prevention/management
Respiratory Function
Functional Mobility
Education
400
Presentations and Functional Abilities
SMA Type 1: weak/absent fetal movement, weakness of proximal muscle of neck/trunk/pelvic girdle, often fatal by 1-21 months, early respiratory distress and us of abdominal to breathe, scoliosis, contractures, may be intubated or have tracheostomy
SMA Type 2: Weakness greatest in hip and knee extensors and trunk, may learn to sit, even stand, course of disease varies widely, median age of death >10 years
SMA Type 3: Proximal LE weakness, postural compensations with resulting contractures, increased lumbar lordosis, Trendelenburg gait, sometimes PF contractures and scoliosis, No significant UE weakness, may live into adulthood
400
What to Rule Out When Considering Idiopathic Toe-Walking
Rule Out: Neurological/Sensory Processing Conditions - Autism, Tethered cord, hereditary spastic paraplegia, muscular dystrophy, Charcot-Marie-Tooth, spina bifida, SCI
Exam: Rule out neuro, measure ROM, gait assessment, gross motor skills/balance/coordination
Treatment: PROM/AROM, functional activities, orthotics and/or serial casting, stretching, gait training
400
Treatment Options for Neuromuscular Scoliosis
Non-Surgical: Regular Screening, bracing typically does NOT prevent progression, but helps provide trunk support, custom molded seat
Surgical Treatment: Goals - improve pulmonary status, trunk balance, transfers, longer instrumental to prevent recurrent deformities, longer healing times (3-9 months)
400
PT Interventions
Prone/tummy time
Positioning/Repositioning --> car seat, baby carriers sleeping
Warm-up exercises --> shoulder depression, trunk stabilization, spinal stretch, bilateral AROM, neck stretches, hip stretches --> for older baby (>20-22 months, strength and development
500
How to Manage Contractures
Stretching: gastrocs, hamstrings, TFL
Night Splints: and stretching leads to longer duration walking
Standers -- Later stage
ROM
500
Interventions
SMA Type 1: Positioning = KEY, supine on wedge --> improve respiration, side-lying --> promote midline head position and hand to midline, NO PRONE (too much effort to lift head and compromises respiration), supported sitting (focus on good spinal alignment to prevent respiratory compromise; support head/trunk), ROM to prevent contractures, AVOID FATIGUE, encourage active reaching with lightweight toys
SMA Type 2: TLSO --> trunk control, molded seating/positioning, standers/standing frames, short therapy session to avoid fatigue, developmental skills, aquatics, KAFO's for standing, wheelchairs (power vs. manual)
SMA Type 3: Stretching/ROM --> decrease contractures, selected strengthening, power scooter for longer distances, LE bracing as needed, AD for walking --> good UE strength
500
Differential Diagnosis of Limping at Different Ages
Birth - 5 years: osteomyelitis, septic arthritis, transient synovitis, fractures, tumors
5-10 years: Legg-Calve-Perthes Disease, Discoid Lateral Meniscus, Sever Disease, Growing Pains
10-15 years: Slipped Capital Femoral Epiphysis (SCFE), Osgood-Schlatter, Osteochondritis Dissecans (OCD)
500
Compare/Contrast Causes and Treatment of Kyphosis
Congenital: surgery
Scheuerman's Disease: exercise, possible CTLSO brace, and surgery
Postural Roundback: exercise, possible bracing
500
Discharge Criteria and Goals
Full PROM bilateral cervical rotation and lateral flexion
Full and symmetrical bilateral cervical rotation and lateral flexion AROM without compensation
Symmetrical and age-appropriate head and trunk righting
Maintains head/neck posture in midline 90-95% of the time in all developmental positions
Symmetrical gross motor skills
HEP --> continue up to 3-6 months