Who Dat!
Make it Count!
Let's Cool You Down!
I'm so Toxic!
Stop the Bleeding!
Understood the Assignment!
No Cap!
BASED OFF AORN STUDY GUIDE
BASED OFF AORN STUDY GUIDE
Did it for the Gram!
BASED OFF AORN STUDY GUIDES
BASED OFF AORN STUDY GUIDES
100
This is how often the scrub person should change gloves during a procedure?
Every 60-150 minutes and after contact with bone cement.

100
This is the name of what should be done before each case to ensure that ALL evidence from the previous patient and procedure has been removed.
The Room Survey.
100
During a MH crisis, after the first dose is given, this is the amount of Dantrolene that you would give the patient if their symptoms were not resolving.
After initial dose and if the initial symptoms re-occur, another full dose is given. If indicated, maintenance dantrolene should be continued as a drip (1mg/kg/dose every 4-6 hours).
100
This is the type of anesthetic used when making a skin incision or when administering nerve blocks.
Local anesthetics.
100
This protocol can be activated if the patient meets criteria for excessive bleeding.
Massive Transfusion Protocol (MTP).
100
This is the area of the gown that is considered sterile.
The chest to the level of the sterile field and the sleeves from 2 inches above the elbow to the proximal edge of the cuff.

100
This is how often horizontal surfaces in the OR should be damp dusted.
Before the first surgical procedure of the day

100
This is the type of sterile towel that would be considered a drape.

Impervious towel
200
Consent etiquette is required when filling out consents. These are some items that you must be sure to check.
No abbreviations, must include laterality and levels, must match the order in the EMR, must be signed by the patient/patient representative and surgeon PRIOR to leaving PREOP.
200
This is the correct sequence when performing closing counts, starting with the patient/surgical wound.
From the patient/surgical wound, to the mayo stand, to the back table, to the kick bucket, to the sponge bags, to off the field.
200
These are known to be triggering agents in an MH crisis.
Inhaled anesthetic agents or Succinylcholine.

200
These are some skin complications that can arise from local anesthetic infiltration.
Petechaie, Bruising, Hematoma, Soft Tissue Injury, and LAST.
200
These individuals are able to "initiate" the order of MTP.
Advanced Providers, MDs, DOs, Surgical Residents.
200
This is the element of the fire triangle that a laser belongs in.
Ignition
200
This is how you should protect the sterile field IF you have set up, but the case is unexpectedly delayed.
*The sterile field can be covered with sterile cuffed drapes
*A portion of the back table that will not be used immediately can be covered
*Remember to prepare the sterile field as close to the time of use as possible
*Policy states a 2-hour limit.
200
This is how we can confirm the success of the biological indicator testing (BI).
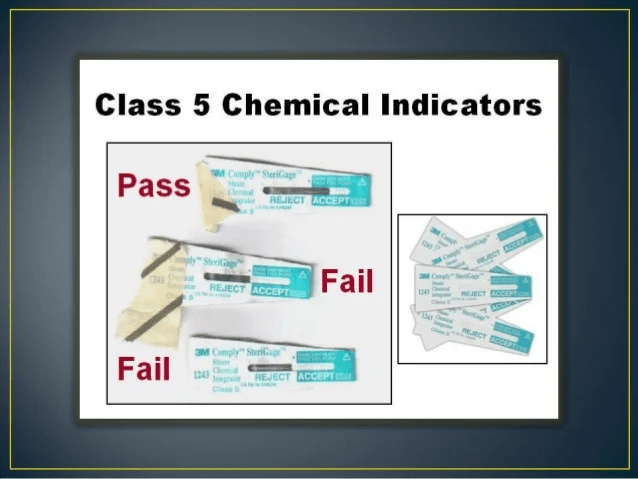
A BI vial that is unprocessed should produce a positive result after incubation.
300
This is how recent a history and physical must be updated for an inpatient surgical patient.
Within the last 24 hours.
300
This is what must be written on the white count board for any sponges being placed inside a cavity.
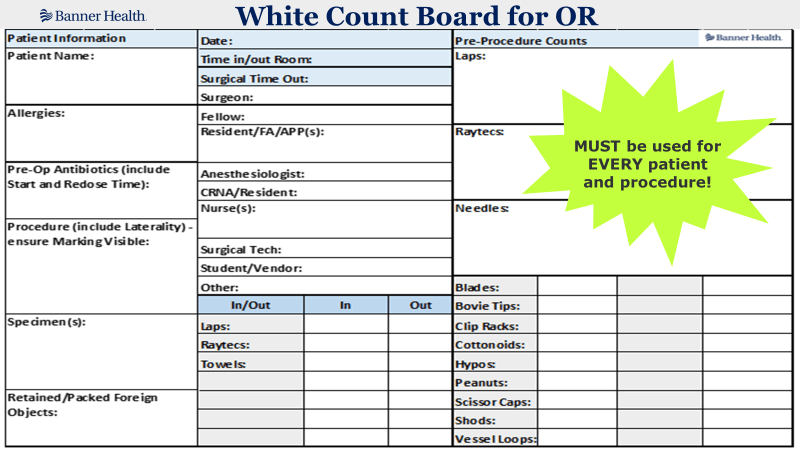
The number of items placed in the cavity and the number of items removed from the cavity. "Announce and Count"
300
This is an anesthetic agent that can be used in a patient with a history of MH.
Propofol.
300
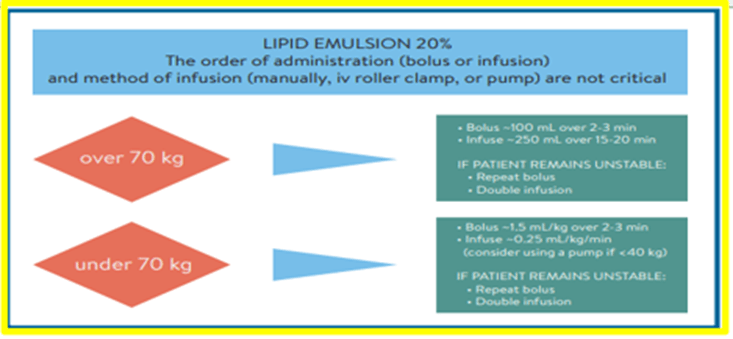
This is the reversal agent for Local Anesthetic Systemic Toxicity (LAST).
Intralipid 20%.
300
There are 3 different criteria that needs to be met in order to initiate MTP. Can you name one?
Administration of 8-10 units of RBCs to an adult in less than 24 hours.
Acute Administration of 4-5 units of RBCs in one hour.
Pediatric patients who are requiring blood products for resuscitation.
300
The best practice we taught you to do when you start your shift in the OR.
Best practice is to perform a First Scrub of the Day.

300
This is the definition of an Accountable Care Organization.
VOLUNTARY coordinated effort across health care specialties.
300
This is the type of risk factor for surgical patients who use Alcohol.
Exaggerated physiological stress response

400
This is what should be done before the patient's surgical site is marked.
Checking the physician's orders, checking the consent, asking the patient to verify the procedure, and checking imaging or radiologist's reports to confirm the procedure.
400
This is the name of the count that must be performed PRIOR to the patient entering the OR.

Initial or Baseline Count.
400
These are EARLY signs of MH. How many can you name?
Increased ETCO2.
Sinus Tachycardia.
Masseter (jaw) rigidity.
Muscle rigidity.
400
There are signs you may see/hear in a patient exhibiting symptoms of LAST. Can you name one?
Tinnitus, Blurred Vision, Dizziness or Lightheadedness, Tongue Paresthesia.
400
The MTP process outlines the protocol and what steps to follow. Can you remember any of the steps?
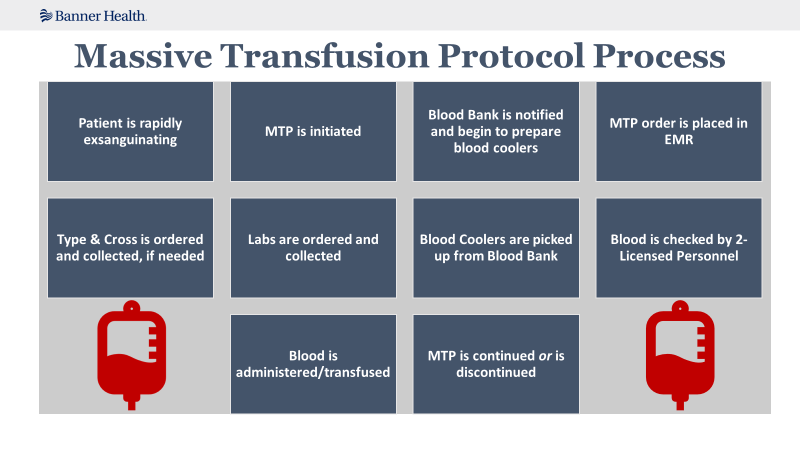
400
This is when we know it is safe for anesthesia to remove the ET or LMA?
When the patient is able to maintain their airway on their own.
400
This is how you would let your gown unfold if you were gowning yourself off the mayo.

Step back and allow the gown to unfold without contaminating. This is why we gown off the mayo or available side table instead of the back table.
400
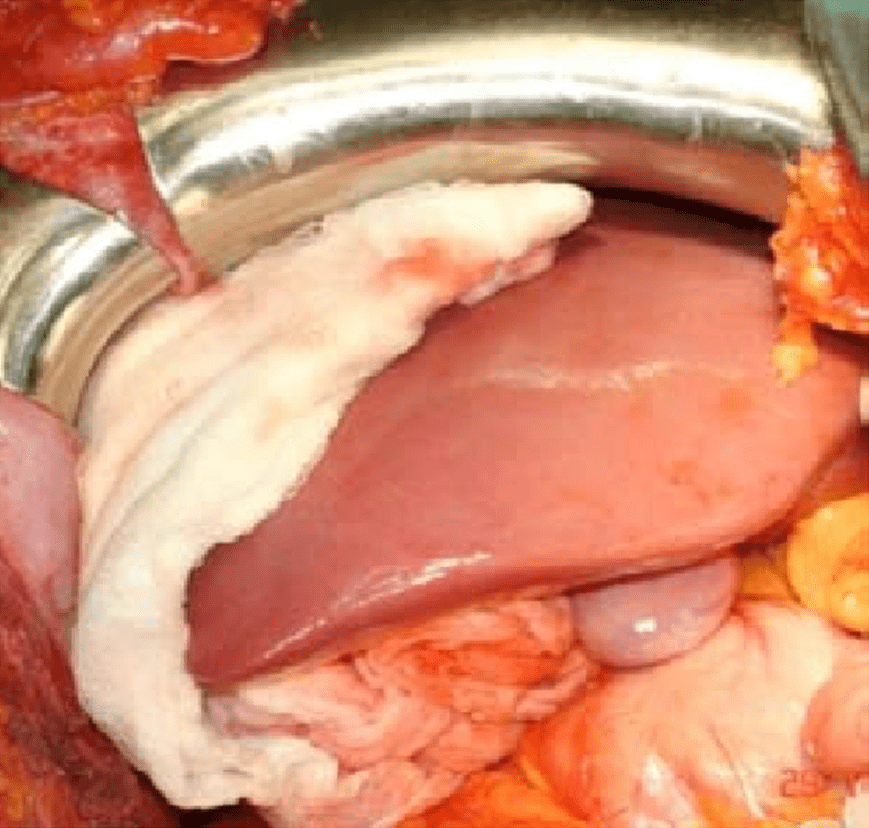
This is what should be documented after surgery regarding skin antisepsis if this is what your patient's skin looks like after surgery.

Hypersensitivity
500
This is the type of marking the surgeon should place on the patient's skin at the surgical site.
Their initials. The way the surgeon marks the patient should be a consistent mark used throughout the hospital (IR, ICU, ED or anywhere procedures are done).

500
This is the type of sponge/towel that MUST be used for intentional packing.
RFID sponge or towel.
500
This is the first thing you should do if your patient is showing signs and symptoms of an MH crisis AFTER stopping the triggering agent.
Call for help!!

500
This is where your Intralipid 20% can be found.
In the Lipid Rescue Kit, PYXIS, and in Pharmacy.
500
This must be completed after the administration of blood products to the patient.
Transfusion Record and EMR Documentation.
500
This is what could negatively affect the sterility of an instrument.

Exposure to moisture.
500
This is the FIRST step in reprocessing surgical instruments after they have been used during a procedure.
Cleaning bioburden off instruments.
500
If an RN omits a section of the Surgical and Procedural Safety plan during the timeout because of an interruption, it is considered what type of error?
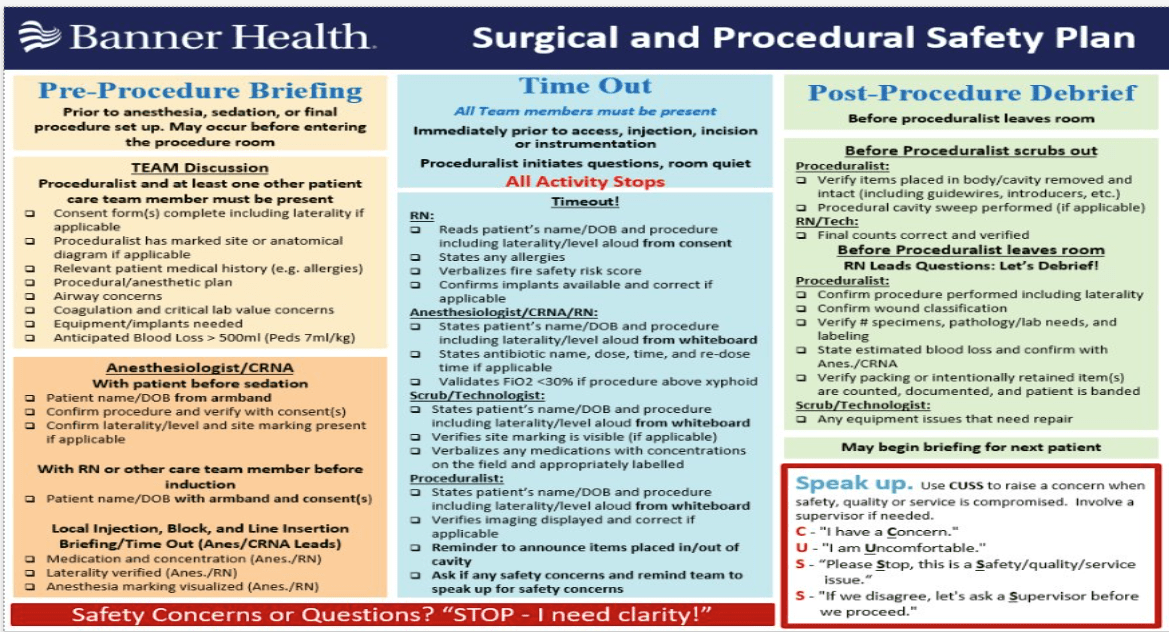
Skills-based error
600
This is how the surgeon should mark a patient who has a cast on and is scheduled for an ORIF of the left wrist.

Surgeon's initials on the anatomical diagram.
600
This is the first thing you should do if you have an incorrect count.
Recount! Notify the surgeon it is incorrect.
600
These are the carts that must be in the room if your patient is showing signs and symptoms of an MH crisis.
MH Cart and the Code Blue Cart!
Make sure you know where both are!
600
There are two available sizes of bags for Intralipid 20%. Can you name one?
250mL or 500mL. Please be sure you where and how much of this is kept at your facility.
600
This is who must be notified with either the continuation or the discontinuation of MTP.
Blood Bank.
600
This is one the most common complications we are concerned about when a patient is in the Trendelenburg position for an extended period.

Increased intraocular pressure.
600
This is when biological monitoring should never be used.

In IUSS (Immediate Use Steam Sterilizers)
600
This is the stage of pressure injury if there is painful skin that is abraded, blisters, or has shallow crater.
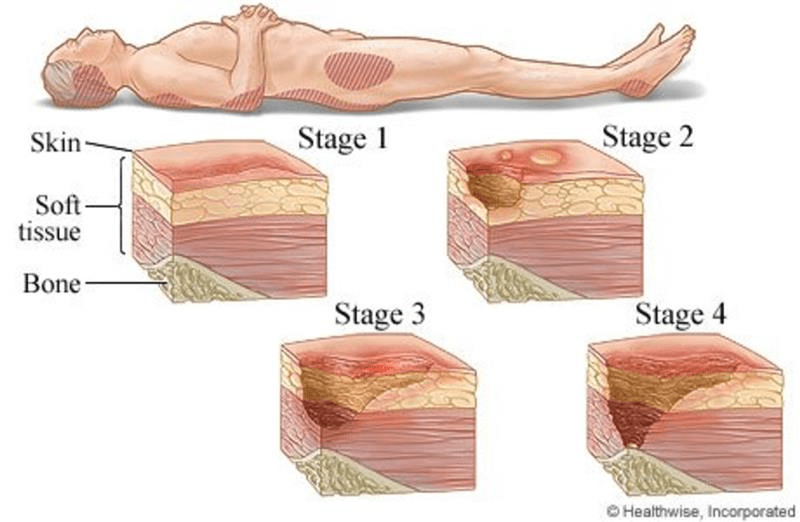
Stage 2
700
This is a characteristic of patient and family centered care. Name as many as you can!
Alliance between health care practitioners, the patient, and the patients support system
Focus on communication with everyone who is involved in the patient's care (patient and family)
Patient and family participation in care
700
There is a miscount. This is what must be done if the room and patient have been searched using the SurgiCount reader and the count is still off.
Intraoperative imaging MUST be taken.
700
This is the name of the professional organization you should also call during an MH crisis.
MHAUS
MHAUS Hotline
1.800.644.9737
1.800.mh.hyper
700
This is another name for Intralipid 20%.
Liquid Emulsion OR Fat Emulsion.
700
This is how often vitals are taken while the patient is receiving MTP.
Continuously via anesthesia monitoring and documented every 15 minutes during transfusion. More frequently if needed.
700
This is the most likely physical injury that can occur when a patient is in the lithotomy position.
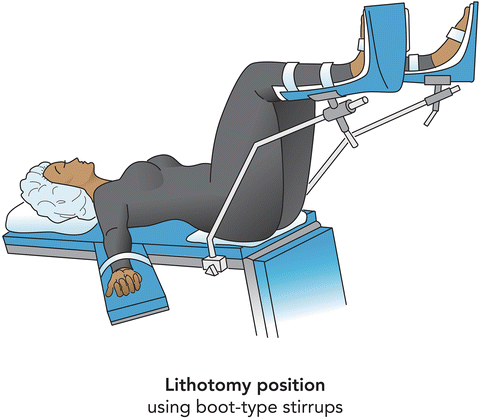
Hip dislocation.
700
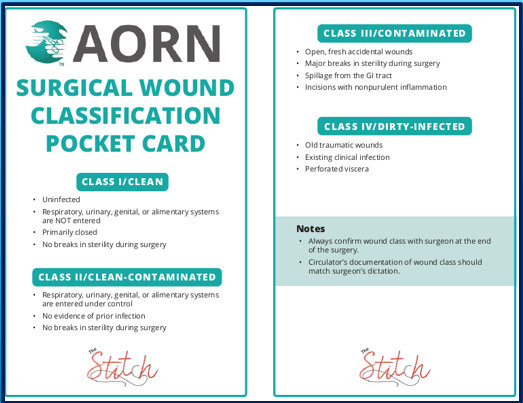
This is the wound class that you would document if you were in a laparoscopic appendectomy and the surgeon encounters purulent inflammation of the appendix.
Wound Class IV
700
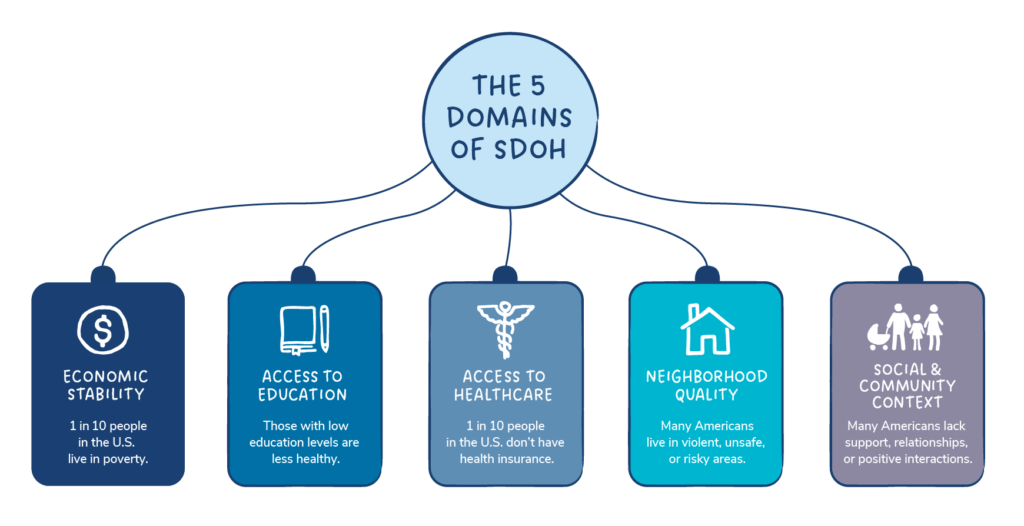
This is the Domain (SDOH) that associated with employment, food, housing and poverty.
Economic stability
800
This is what the OR RN should do if they are taking their patient to surgery, but the patient's site has not been marked AND there is also no Anatomical Diagram.
STOP and have it completed.

800
This is what we do when someone interrupts the visual and audible counts between the circulator and the scrub.
Restart! Pause for the Gauze!
800
For Arizona Facilities: This is how many mg's are in a vial of dantrolene.
For Western Division: This is how many mg's are in a vial of ryanodex.
20mgs in Dantrolene
250mgs in Ryanodex
800
This is where your patient should be transferred to after an occurrence of LAST.
ICU or higher level of care.

800
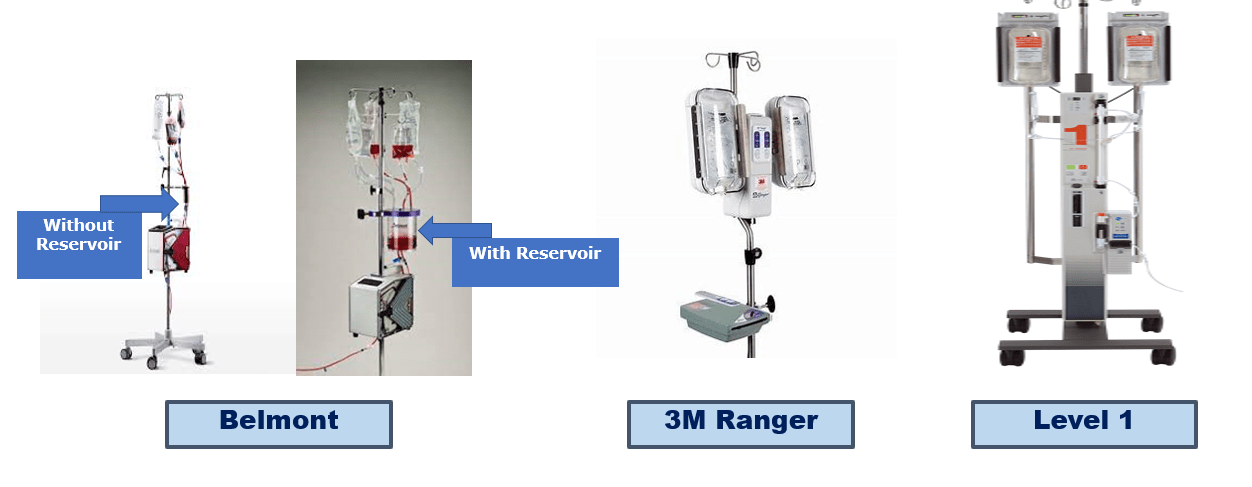
These are the names of the equipment that is used for rapid blood infusion.
Belmont, 3M Ranger, Level 1.
800
This is how to determine how long a wrapped item on the shelf in the core is sterile.

Sterility of wrapped items is Event Related for wrapped items and 5 years for heat-seal pouches and 3 years for self seal pouches.
Dropping it on the floor, moisture detected on the packaging, rips or tears in the packaging.
800
This is the phase of healing where hemostasis, phagocytosis and edema occur.
Inflammation.
800
This is a way to describe what health disparity means.

Higher burden of some populations.