Intro to Antimicrobials
Cell Wall Agents
100
A laboratory scientist was trying to find the amount to kill a particular microbe, but noticed that increasing the multiples of MIC did not kill the organism. List 4 organisms that the scientist could possible discover.
Beta-lactams
Vancomycin
Most macrolides
Tetracycline
"Be Very Mindful that Time matters.
Concentration dependent organisms which can be susceptible to increases in MIC include aminoglycosides and fluroquinoles. These 2 are also bacteriocidal
100
A 26 year old female presents with a strong, persistent urge to urinate, a burning sensation when urinating (dysuria), and passing frequent, small amounts of urine.
She is prescribed a medicine that acts on a slow, lactose fermenter. What is the MOA of the drug she is given?
F
Fosfomycin: inhibits synthesis of UDP-NAM from UDP-NAG by inhibiting MurA
Effective against Gram negative bacteria in the urinary tract.
The patient likely has Serratia but know the E.coli would be most common.
200
What drugs inhibit growth allowing host response to overcome?
Sulfonamides and ribosomal agents (except aminoglycosides)
300
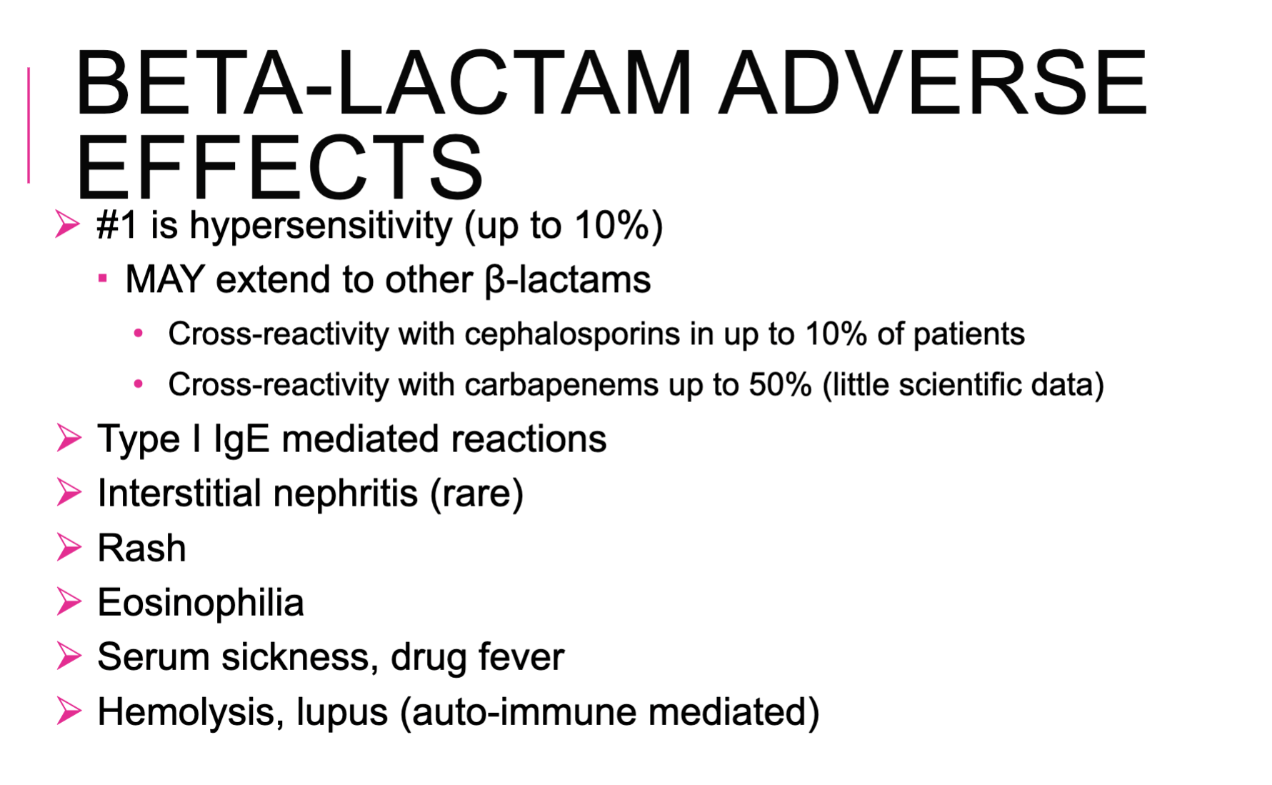
What are adverse effects common in antibiotics?
-Superinfection
-Diarrhea
-GI upset
-Hypersensitivity: SJS/TENS, IgE mediated anaphylaxis
300
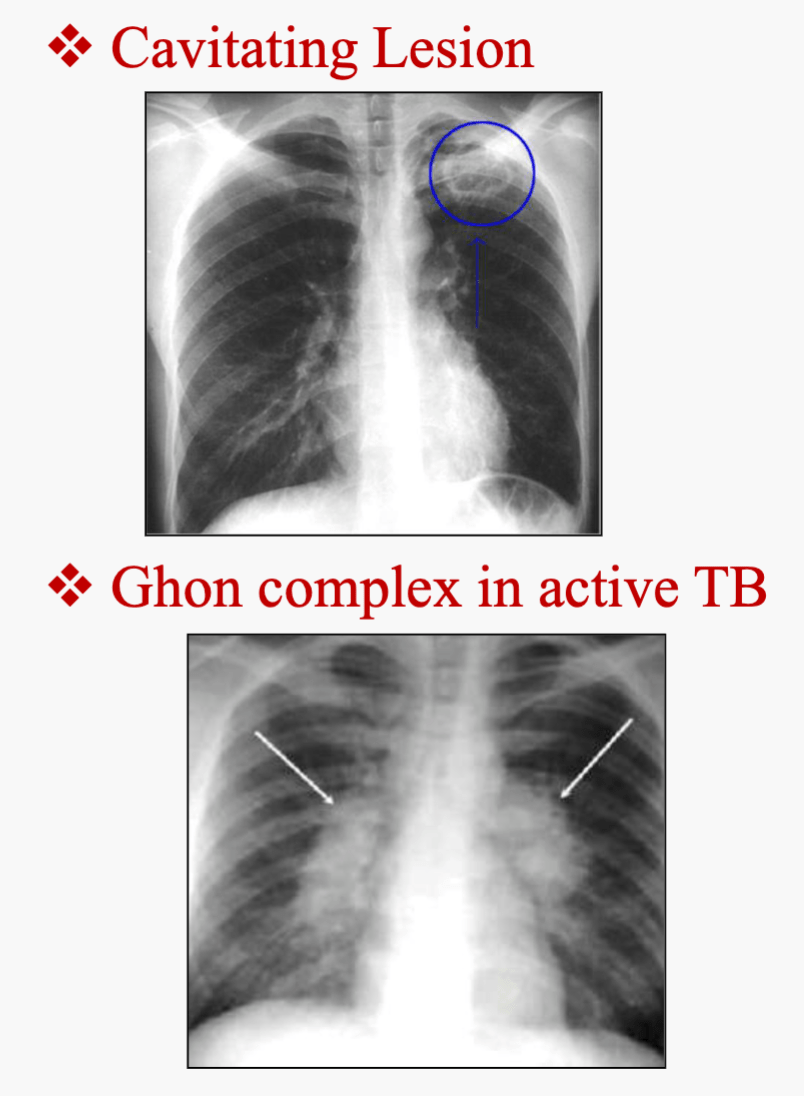
On a Ziehl-Neelson stain, a scientist isolated a facultative intracellular, aerobic, gram positive bacillus that is acid fast. This species produce niacin and it's ability to multiply within macrophages acts as it's main virulence factor.
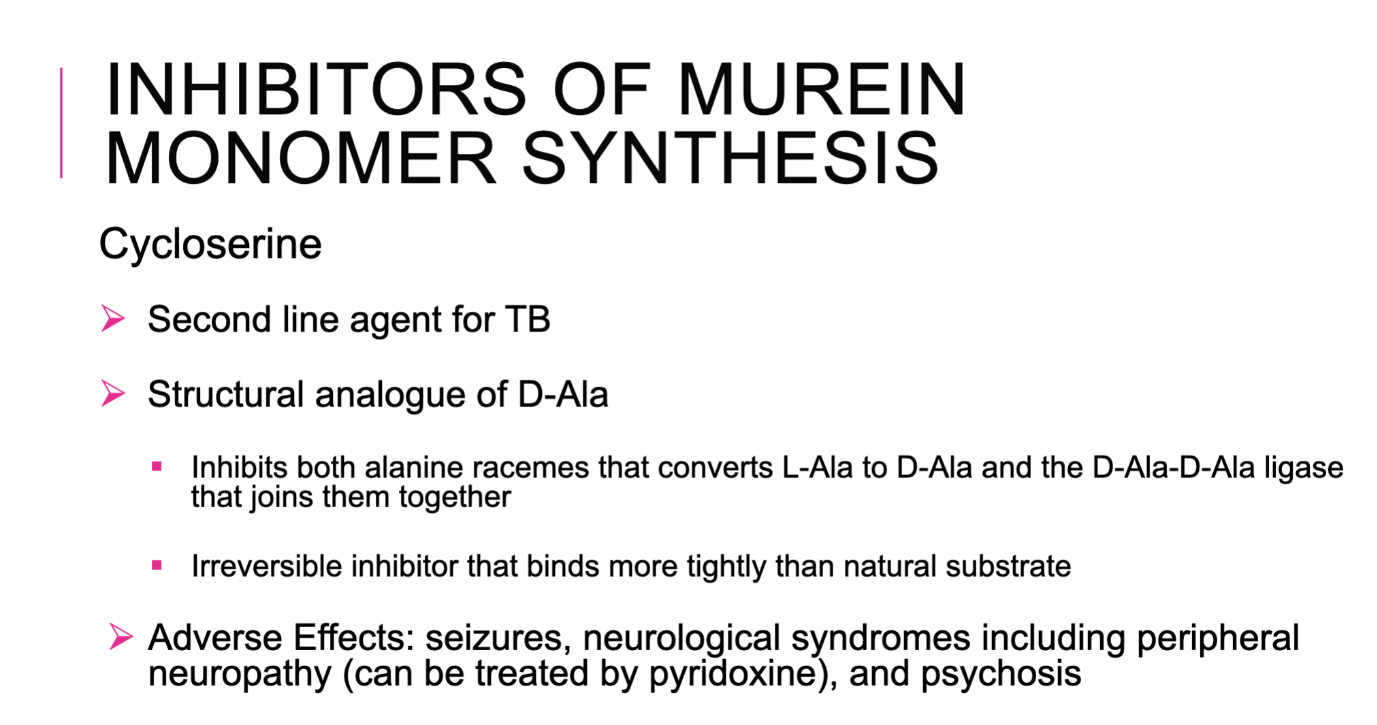
What is the drug given in second line therapy?
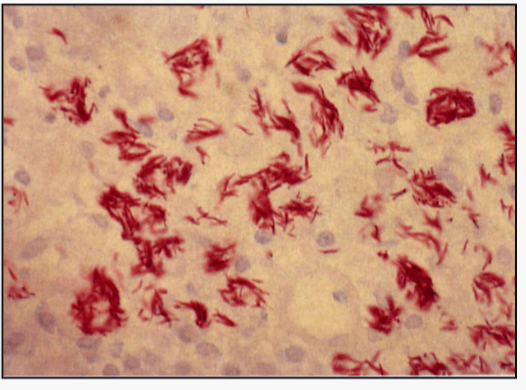
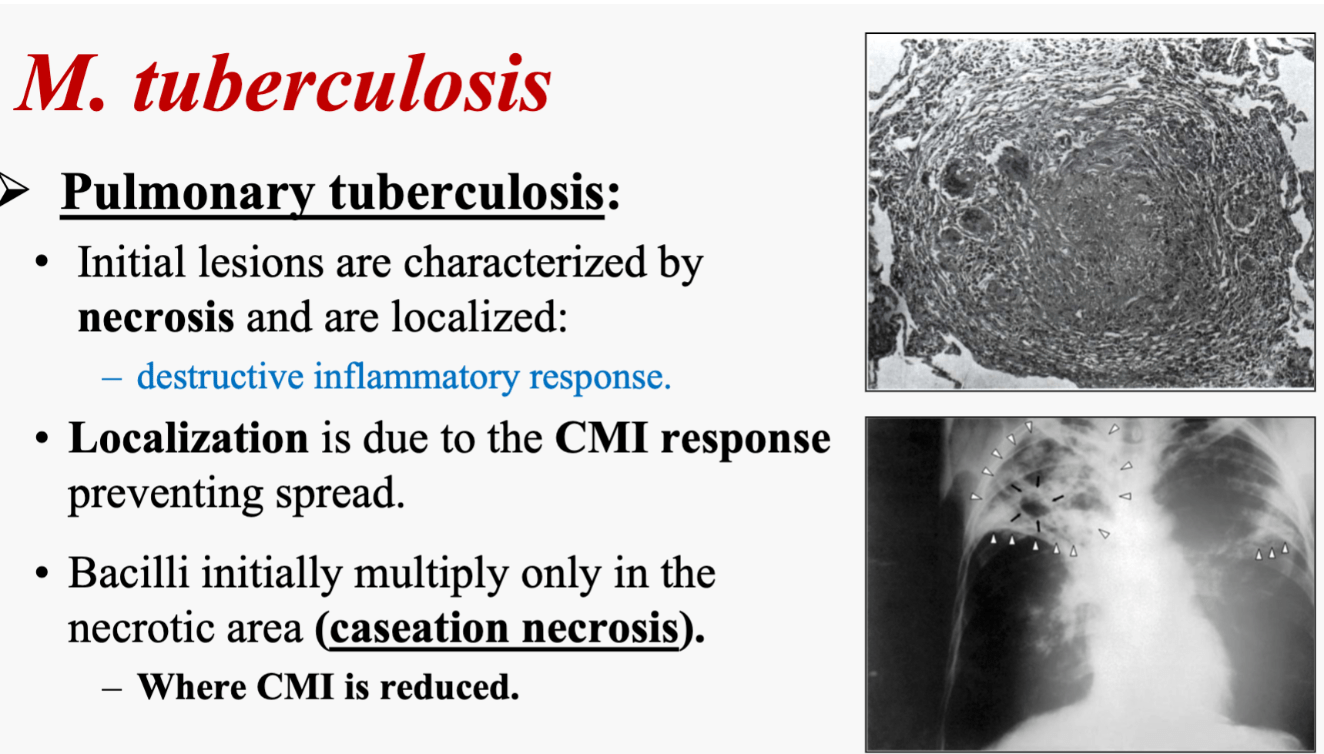
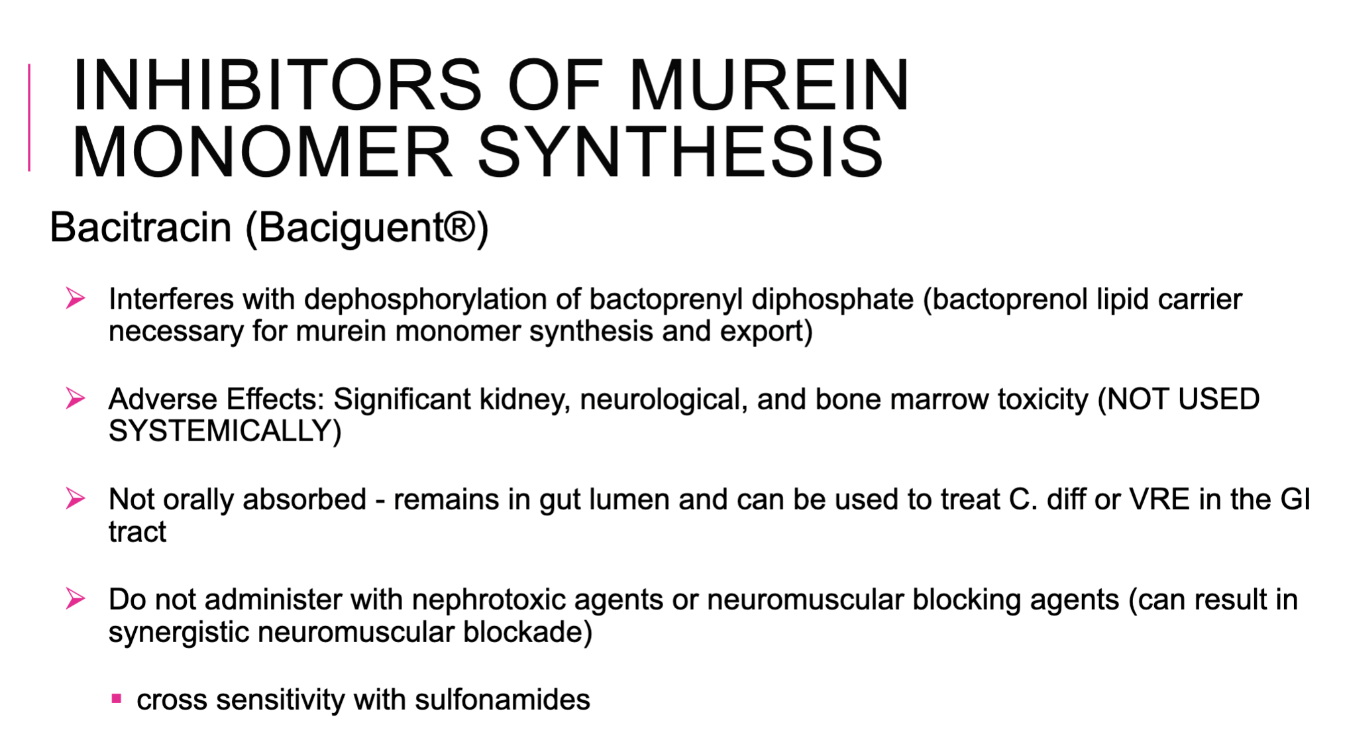
Cycloserine which inhibits the synthesis of murein monomer.
400
What is the Number One way to prevent drug resistance?
WASH Yo Hands
400
A patient presents with profuse, watery/mucoid green foul-smelling diarrhea after being treated with clindamycin and lincomycin anti-biotic that bind to the 50S subunit. Based on the presentations, you diagnose them as having pseudomembrane colitis. What is the side effect of the medicine you can use to tx the patient. AND what is it cross-sensitive with.
-Oral Vancomycin
-ADE: significant kidney, neurological, and bone marrow toxicity.
Cross-sensitivity to sulfonamides
What happens when you give vancomycin orally?
-Red man syndrome: flushing, itching, pruritus, erythematous rash involving face, neck, and upper torso.
500
Bacteria that causes neonatal meningitis:
GBS (S. agalactiae) + E.coli + Listeria + Klebsiella
"ELKS"
500
All drugs used for MRSA:
-IV Vancomycin
-Daptomycin
600
What 2 things determine the spectrum of activity for Beta lactams?
-ability to enter periplasmic space
-affinity for specific transpeptidases
Avoid if patient has anaphylactic level reactions.
Organisms that lack peptidoglycan cell walls are inherently resistant (mycobacteria, protozoa)
700
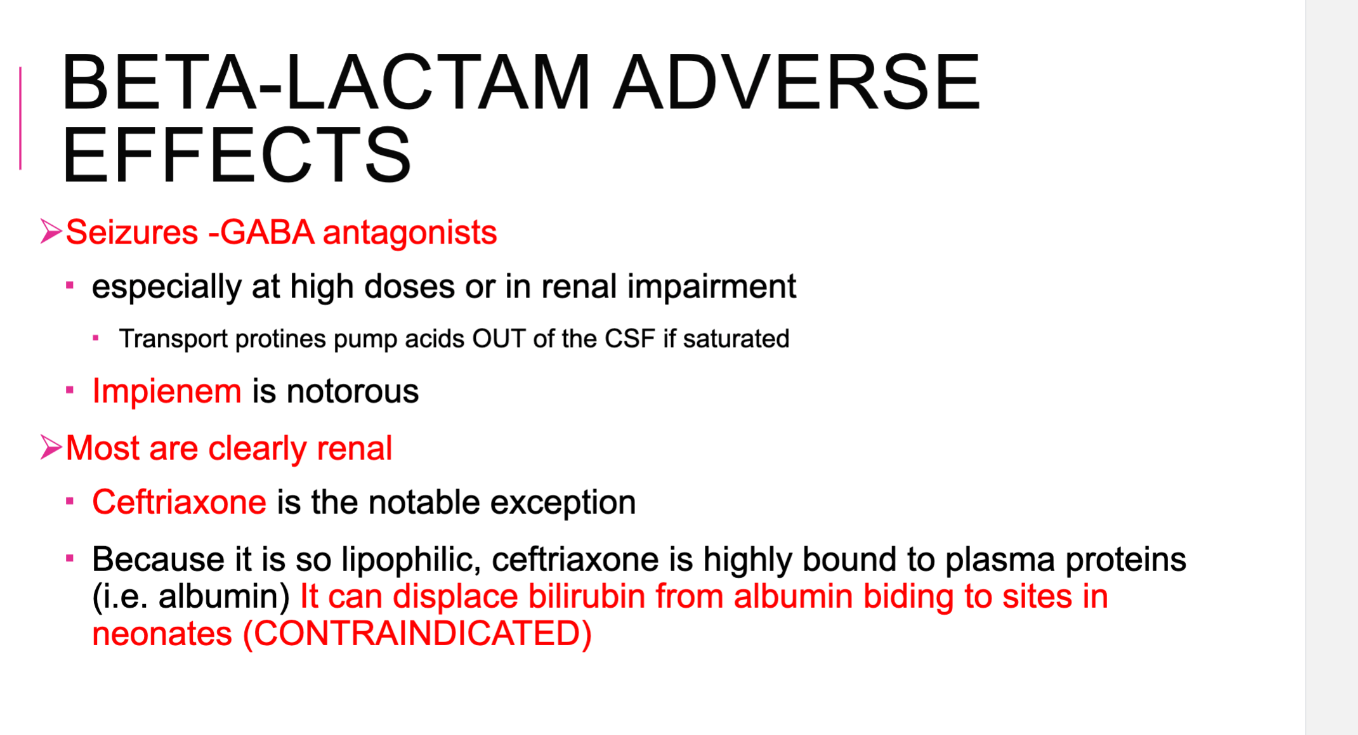
Why should ceftriaxone be avoided in neonates with a gram positive infection?
Ceftriazone, a B-lactam, should be avoided because it is so lipophilic that is remains highly bound to plasma proteins and can displace bilirubin from albumin binding to sites in neonates. It is the exception for Beta lactams since most are renally cleared.
800
If I was a bacteria with Beta lactam, how would I become resistant?
-By producing Beta lactamases
so, you can give B-lactam inhibitors with drugs
Beta lactam is the drug, the target is penicilin binding proteins that build the bacterial cell wall.
Beta-lactams--> bind PBPs --> stop cell wall synthesis --> bacteria dies.
Bacteria fights back by making B-lactamases that destory the Beta-lactam ring. Once broken, drungs can't bind PBPs.
If B-lactamse is present, give sulbactam, tazobactam, calvulanic acid as a Beta lactamase inhibitor.