Risk Factors
Polyps
Diagnostics
Treatment/surveillance
Colon cancer
100
Where does CRC rank amongst other cancers for both males and females in morbidity and mortality in the US?
3rd highest morbidity and mortality among all cancers in the US for both males and females
Bonus Questions:
What recent cultural habits or environmental factors might contribute to such high rates?
What are the top 2 highest morbidity and mortality cancers for males and females in the US?
Why might knowing this information be important?
100
What is a colonic polyp? What are the two common types?
A mucosal protuberance into the colonic lumen
1. Neoplastic (adenoma- benign tumor of epithelial tissue with glandular origin) - There is uncontrolled, monoclonal growth.
2. Non-neoplastic (hyperplastic polyps) - No uncontrolled monoclonal growth.
Bonus: Which type has the higher potential to progress to cancer?
100
What are some of the screening options available for colorectal cancer?
Stool Test: Blood Occult
Visual Exam: Sigmoidoscopy, Colonoscopy, CT colonography
Bonus Questions:
1. What is the difference between a sigmoidoscopy vs colonoscopy?
2. What age should you perform screening?
3. What age if the patient has a family history of CRC?
100
A biopsy confirms the dx of colonic carcinoma in situ. The lesion was successfully resected and the patient underwent regular surveillance with follow-up colonoscopies.
Years later, a repeat colonoscopy and imaging revealed a mass in the sigmoid colon with involvement of regional lymph nodes. A biopsy confirmed stage 3 colonic adenocarcinoma.
How does the prognosis and treatment of the recurrent disease differ from the original diagnosis?
As the stage of colon cancer increases, there is poorer prognosis and more reliance on adjuvant chemotherapy.
For this stage 3 recurrence, the pt would undergo surgical resection with adjuvant chemotherapy.
Bonus: What is a defining trait of carcinoma in situ? Why does this stage of cancer (stage 0) not require chemo?
100
What is the ULTIMATE difference between benign and malignant neoplasm?
Malignant invades/metastasizes, benign doesn't
200
Knowing your patient is from which 2 ethnic groups might raise concern for CRC and prompt you to perform early screening?
Ashkenazi Jewish (highest rates in world) and Native American/Alaskan (highest rates in the US)
Bonus Questions:
What type of screening might you want to do?
What lifestyle changes would you recommend?
Imagine you are explaining the need for these lifestyle changes to a patient from one of these populations who doesn’t have any signs of cancer yet. What would you say?
200
Describe the chromosomal instability pathway that causes the development of a polyp all the way through to cancer
APC is a tumor supressor gene
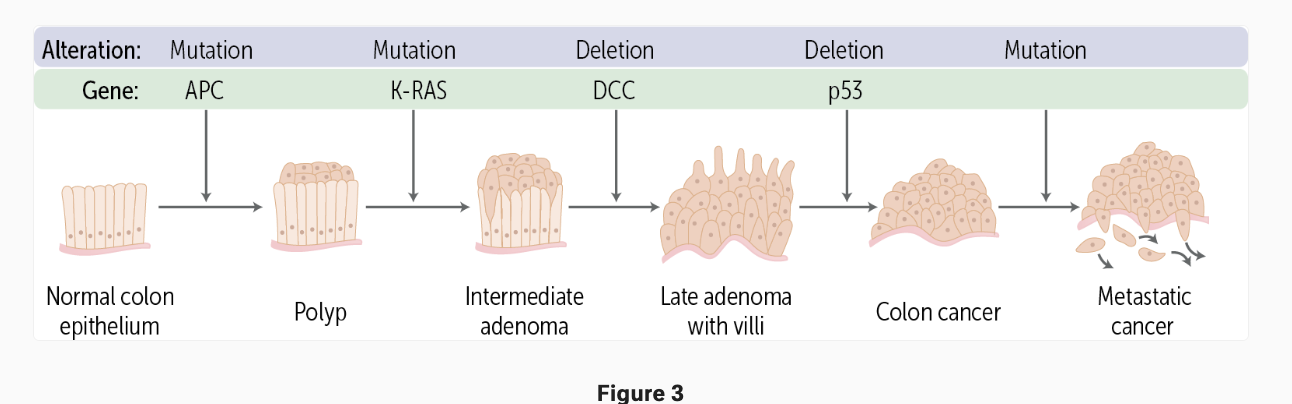
Bonus: Germline mutation of APC is known as part of which genetic syndrome?
200
Identify the imaging technique associated with the below images:
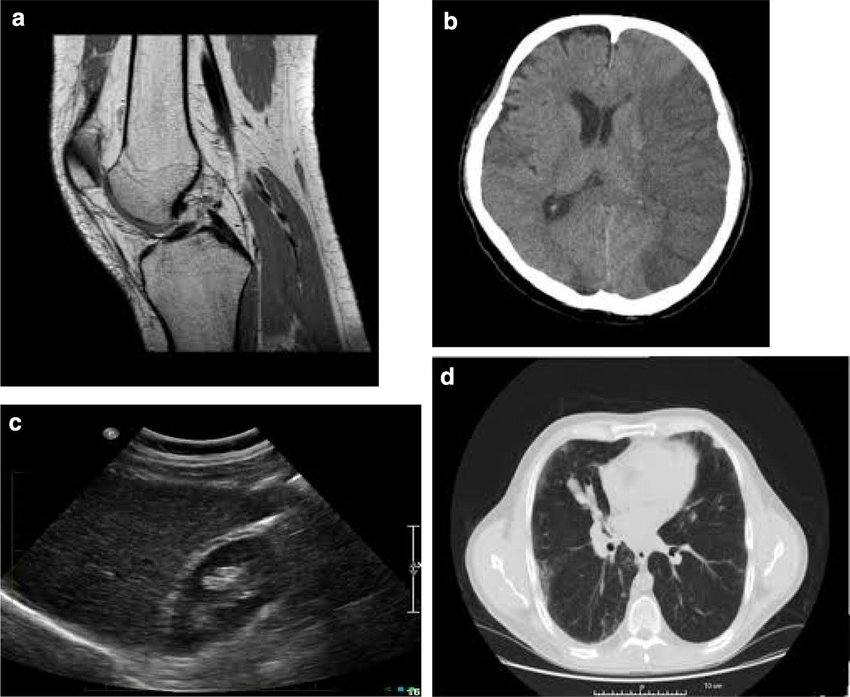
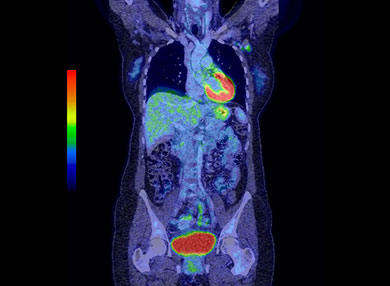
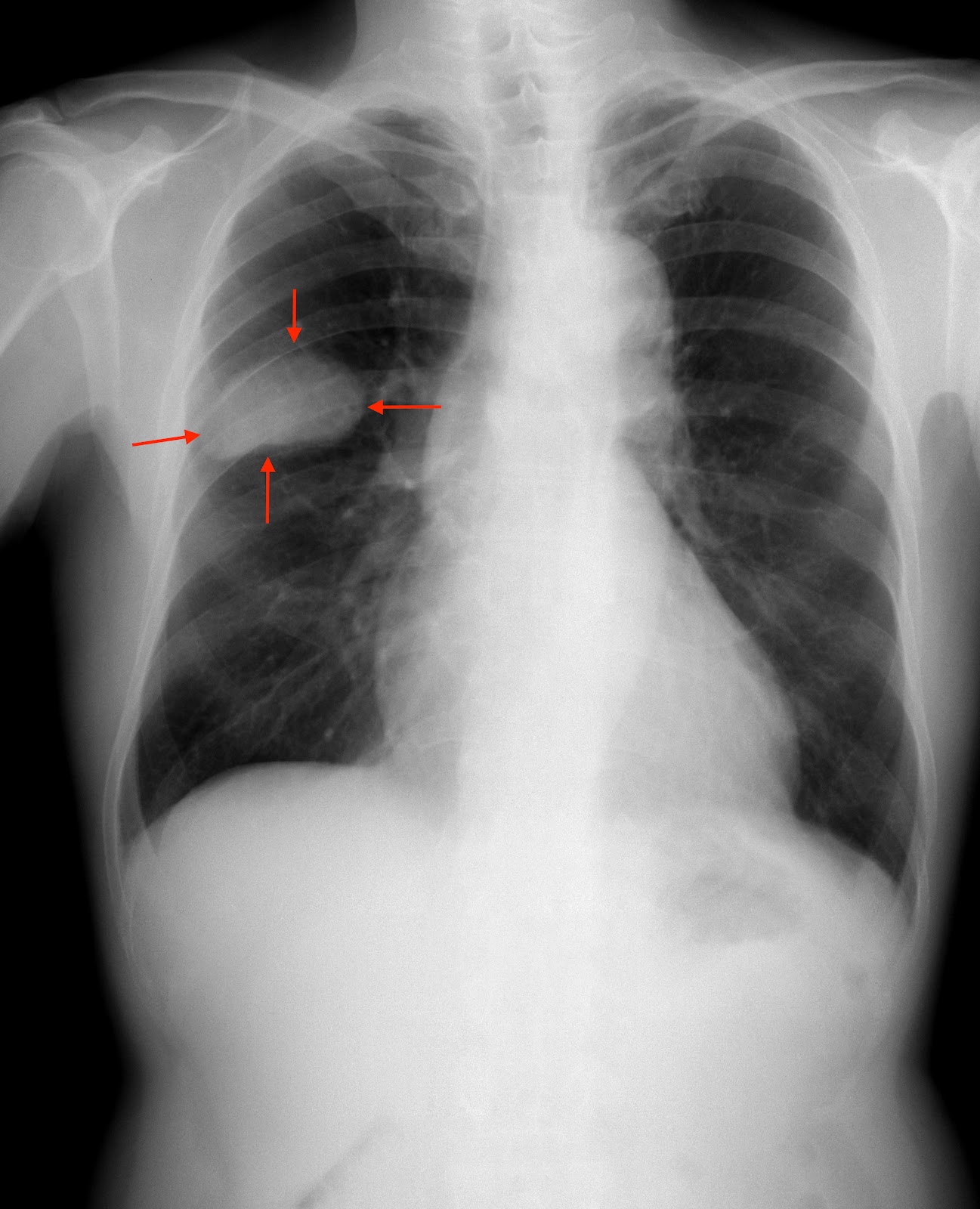
A: MRI, PET (non-colored), Ultrasound, CT, Full Body PET (colored), XRAY
Bonus Questions:
Describe what each type of imaging is meant to show.
What might our patient Derek’s PET look like?
What about other imaging techniques mentioned above?
What cancer red herrings could show up on a PET scan?
200
What is the stage of the following colonic adenocarcinoma:
The tumor has penetrated through the colonic wall with regional lymph node involvement and no evidence of distant metastasis.
T4N1M0
T1: invasion into submucosa
T2: invasion of the muscularis propria
T3: invasion of the subserosa
T4: invasion through all layers of the colon
Tis: carcinoma in situ
Tx: tumor unable to be assessed
N1: 1-3 regional lymph nodes are involved
N2: 4-6 regional lymph nodes involved
N3: 7 or more regional lymph nodes involved
Nx: lymph nodes could not be assessed
M1a: spread to 1 area
M1b: spread to 2 or more areas
M1c: metastasis to the peritoneal surface
Our patient:
T3N1aM0
- T3= tumor grown into the muscularis propria
- N1a = invasion of 1 regional lymph node
- M0 = no distant mets
Bonus: What is the difference between grading and staging?
200
A patient comes in for a routine colonoscopy, and the resident notices a mass on the imaging. What characteristics of the mass would lead you towards benign or malignant neoplasm?
The resident further confirms diagnosis by excising the mass for histological examination. What characteristics would lead you to believe it is benign or malignant?
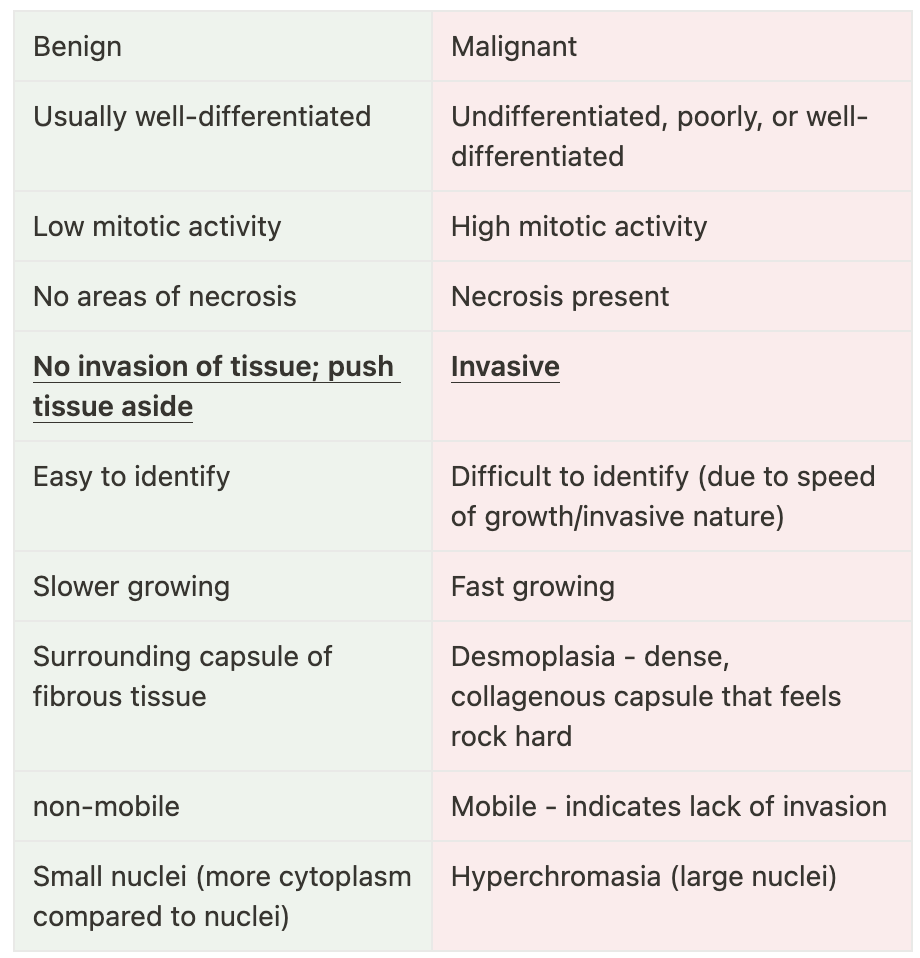
Bonus question: How do we differentiate benign and malignant tumors in terms of nomenclature?
300
What major risk factors of colon cancer do you see?
Patient Profile:
A 55-year-old male presents for a routine check-up. He has a history of obesity, hyperlipidemia, and a sedentary lifestyle. During the visit, he expresses concern about his increasing fatigue and occasional abdominal discomfort, particularly after eating.
Clinical Details:
The patient enjoys outdoor activities like fishing and gardening, but he tends to spend most of his weekends watching sports on TV. He mentions that he often opts for processed foods and sugary snacks while binge-watching his favorite shows. His family history reveals that his father was diagnosed with colon cancer at age 60, and his mother had type 2 diabetes.
Family history of colon cancer and type 2 diabetes, diet high in fats and refined carbs, obesity, hyperlipidemia
Bonus Questions:
What are some other risk factors associated with colon cancer?
What is the recommended screening age for someone without family history?
300
Describe the microsatellite pathway that explains how polyps and eventually colon cancer develops.
mutations or methylation in mismatch repair genes, which can cause some sporadic CRCs as well as Lynch syndrome
300
What is a stool blood occult and what does it check for?
A test to check the stool for blood or breakdown products of blood.
Bonus Questions:
Why is this type of testing needed?
Our patient Derek prefers to do this instead of a colonoscopy. What would you tell him?
What are 3 lab techniques for detecting occult blood after collection and how do they work?
For Fun: Why is it called a guaiac test
300
A 58-year-old male presents to the oncology clinic with a history of metastatic colorectal cancer (CRC). Despite undergoing surgery and standard chemotherapy, the patient’s disease has progressed. As part of his treatment plan, the oncologist prescribes bevacizumab in combination with chemotherapy. After a few months, there is a noticeable decrease in tumor size on imaging.
Bevacizumab is most effective in this patient because of its ability to:
A) Block the epidermal growth factor receptor (EGFR), preventing tumor cell proliferation.
B) Inhibit the enzyme thymidylate synthase, reducing DNA synthesis in tumor cells.
C) Bind to vascular endothelial growth factor (VEGF), preventing angiogenesis and limiting tumor blood supply.
D) Directly induce apoptosis of colorectal cancer cells by disrupting the cell cycle.
C) Bind to vascular endothelial growth factor (VEGF), preventing angiogenesis and limiting tumor blood supply.
300
What are the common locations for metastasis of colorectal cancer?
Liver, lungs, brain, peritoneum, and distant lymph nodes
Bonus question: What vasculature does colorectal cancer typically use?
400
Patient Profile: A 16-year-old girl visits the gastroenterology clinic for evaluation due to a family history of colorectal cancer. She recently joined the school’s debate team and enjoys painting in her free time.
Clinical Details:
The patient reports experiencing occasional abdominal pain but is otherwise asymptomatic. She loves baking and eats sweet desserts with every meal. A colonoscopy shows more than 100 adenomatous polyps.
What might you expect this patient to have? Why?
The patient is likely experiencing Familial Adenomatous Polyposis (FAP), which is characterized by the development of multiple adenomatous polyps, usually 100+
Bonus Questions:
What gene is involved with this condition and what chromosome is it on?
What is the likelihood that she passes the mutated gene to her child?
Assuming the mutation is passed on, what are the chances of her child having FAP?
400
By what 3 main mechanisms does dysplasia develop into colon cancer?
- Deregulation of cellular energetics by increasing glucose uptake and progression of aerobic glycolysis. Achieved by RTK’s inhibiting pyruvate kinase and causing a build up of glycolysis intermediates in addition to MYC upregulating glycolytic enzymes.
- Angiogenesis is the creation of new blood vessels so that the growing tumor may have access to sufficient glucose and other nutrients needed to grow rapidly. This is primarily accomplished via upregulation of VEGF.
- Replicative immortality is accomplished when cancer cells reactivate telomerase
400
You are doing a rectal exam on the patient and feel a mass in that region. What is in your differential?
Rectal adenoma, rectal carcinoma, hemorrhoids, colitis, prostatitis (males)
Bonus Questions:
You know that the patient has IBD, how might that affect your differential?
What are you more concerned about given this information and why?
400
A 62-year-old woman with metastatic colorectal cancer is undergoing chemotherapy that includes 5-fluorouracil (5-FU) and leucovorin. After several cycles, she shows a significant reduction in tumor size. The oncologist explains that leucovorin is being used alongside 5-FU for enhancement purposes.
What is the primary mechanism by which leucovorin enhances the action of 5-fluorouracil in treating this patient’s colorectal cancer?
A) Leucovorin stabilizes the binding of the 5-FU metabolite to thymidylate synthase, increasing inhibition of DNA synthesis.
B) Leucovorin increases the clearance of 5-FU from the bloodstream, reducing its toxicity.
C) Leucovorin acts as a direct chemotherapeutic agent by inducing DNA breaks in colorectal cancer cells.
D) Leucovorin reverses the adverse effects of 5-FU by increasing the regeneration of normal cells.
A) Leucovorin stabilizes the binding of the 5-FU metabolite to thymidylate synthase, increasing inhibition of DNA synthesis.
Bonus question: Which drug does leucovorin actually result in the reverse effects of?

400
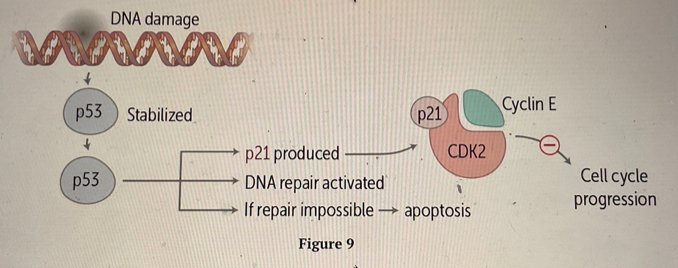
A 35-year-old female patient presents with a family history of multiple cancers, including breast and colon cancer. Genetic testing reveals a mutation in one allele of the p53 gene. What following steps would lead to highly increased risk for tumor formation for the patient? Explain your answer how you would say it to the patient who is very nervous.
Somatic mutation - explained by two-hit hypothesis
Bonus question: What is the pathway of p53 tumor suppression for apoptosis?
500
This syndrome is caused by a loss of function mutation in mismatch repair genes, leading to an increased risk of colorectal cancer
Lynch Syndrome
Bonus Questions:
1. What type of gene would this be?
2. What might the inheritance pattern look like?
3. What is mismatch repair?
500
A 32-year-old male presents to the outpatient GI clinic with abdominal pain and changes in bowel habits over the past few months. He reports episodes of loose stools alternating with constipation and occasional rectal bleeding, which he initially attributed to hemorrhoids.
Fhx: Father died of CRC at the age of 45
Physical Examination:
- Vital signs are stable
- Abdominal examination reveals no masses, tenderness, or hepatomegaly
Workup:
Colonoscopy:
- Numerous polyps (>100) are found throughout the colon, with the largest polyp measuring 1.2 cm in the descending colon. The polyps are consistent with adenomatous polyps
Histopathology:
- Biopsy results confirm the polyps are adenomatous with low-grade dysplasia
You plan to proceed with surgical intervention. In addition to this surgery, what would be another next step in this pt's workup/treatment?
Order genetic testing to check for Familial Adenomatous Polyposis (FAP). If
This is indicated given the pt's symptoms, relatively young age, high number (>100) of adenomatous polyps in the colon and Fhx of colon cancer.
Bonus: What is the surgical intervention indicated for people with polyps and FAP?
500
A patient is known to have 1 parent with a deleted APC gene. What genetic testing lab technique could you use to confirm this in your patient?
A: FISH
Bonus Questions:
How might this look if she does have the same mutation as her parents? Doesn’t?
What if her parent didn’t have an APC mutation but there is a clear family history of CRC, what other technique might you use?
You find genetic tests of all her immediate relatives and see that a different gene is mutated on each one. What might this pattern be?
500
Unfortunately, not every patient diagnosed with colon cancer is going to have a positive prognosis. Role play having a conversation with a patient who is diagnosed with a stage 4 adenocarcinoma.
1) Setting
2) Perception
3) Inquiry
4) Knowledge
5) Respond to emotions
6) Summarize; plan
SPIKES
500
Walk through the process of colon cancer intravasation
Downregulation of E-cadherin + upregulation of metalloproteases to break down E-cadherin
Tumor cells bind to laminin on basement membrane
Collagenase breaks down basement membrane
Angiogenic factors, such as VEGF, is released
Invasion of tumor cells into basement membrane
Basement membrane binds to fibronectin, promoting local spread
Tumor cells reach vasculature
Bonus question: What are the remaining steps for tumor cells to metastasize? What protein receptor specifically promotes increased metastasis after intravasation?