Pathophysiology
Physical examination/ clinical manifestation
Labs/ Etiologies
Treatment
Imaging
100
Permanent enlargement of the terminal airspaces distal to the terminal bronchioles with no fibrosis
Emphysema
100
Hyperinflation. hyper-resonance to percussion,. Decreased or absent breath sounds, Barrel chest ) increased AP diameter), pursed lip breathing. Pink puffer appearance
Emphysema
100
Elevated sweat chloride test
Cystic fibrosis
100
first line treatment for symptomatic asthma
Albuterol
100

X-ray shows steeple sign
Laryngotracheitis ( croup)
200
3 components:airway hyperactivity, bronchoconstriction, and inflammation. Increased IgE binds to mast cells initiating an inflammatory response. Present at any age but initial occurence is most common in childhood
Asthma
200
Rales (crackles), rhonchi, wheezing, signs of cor pulmonale are seen ( peripheral edema, cyanosis). Blue bloaters
Chronic bronchitis
200
Cystic fibrosis mos common cause in US (50%) recurrent lung infections: Pseudomonas aeruginosa is he most common cause due to cystic fibrosis. H. influenzae is the most common cause if not due to cystic fibrosis
Bronchiectasis
200
Smoking cessation is the most important step in management as well as Oxygen therapy. They are both factors that reduce mortality
management of COPD
200
![]()
X-ray shows thumbprint sign
Acute epiglotittis
300
Mutations in the CFTR gene result in abnormalities of cAMP-regulated chloride transport across epithelial cells on mucosal surfaces leading to thick, viscous secretions of the lungs
Cystic fibrosis
300
Classical triad: dyspnea, wheezing, and cough (specially at night). Can present at any age but most commonly occurs in childhood.
Asthma
300
Parainfluenza virus type 1 most common cause
Laryngotracheitis (croup)
300
Lung transplant is the only possible cure
pulmonary fibrosis
300

Xray: shows diffused millet-seed like nobular lesions
Miliary TB
400
Chronic inflammation leads to mucus gland hyperplasia, goblet cell mucus production, dysfunctional cilia, and infiltration of neutrophills and CD8+ cells.
Chronic bronchitis
400
Hallmark is cough ( may be productive, present for at leasdt 5 days but usually last 1-3 weeks). Malaise, dyspnea, URI symptoms. Most commonly caused by viruses.
Acute bronchitis
400
H. influenzae B historically was the most common cause. If immunized suspect streptococcal species is the most common.
Acute epiglottitis
400
RIPE therapy: Rifampin, isoniazid, pyrazinamide, and ethambutol for 2 months followed by 4 month continuation phase with rifampin and isoniazid- 6 month total treatment duration
Tuberculosis treatment
400

X-ray: Pleural plaque thickening or calcification of the lower lobes. "shaggy heart" sign
Abestosis
500
Exaggerated T-cell response to a variety of antigens or self- antigens, leading to central immune system activation, granuloma formation, and peripheral immune depression
Sarcoidosis
500
Highly contageous in children. Severe paroxymal coughing fits with inspiratory whooping sound after coughing fits. Often last 2-4 weeks.
Pertussis
500
Cystic fibrosis mos common cause in US (50%) recurrent lung infections: Pseudomonas aeruginosa is he most common cause due to cystic fibrosis. H. influenzae is the most common cause if not due to cystic fibrosis
Bronchiectasis
500
Genetic disorder that leads to pancinar emphysema, hepatomegaly, and cirrhosis. Management: IV pooled alpha-1 antitrypsin and lung transplant.
Alpha-1 antitrypsin deficiency
500
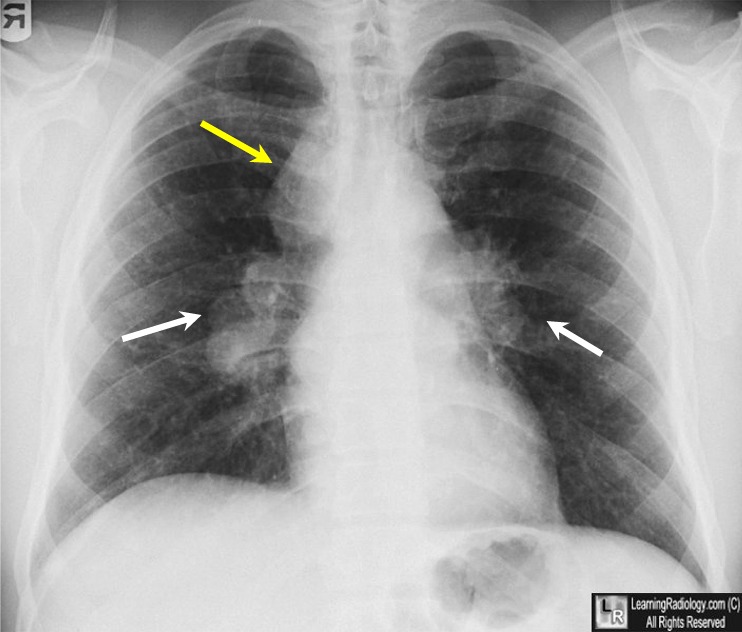
X-ray: Bilateral hilar lymphadenopathy classic
Sarcoidosis