ABSITE Facts
Chemorads
Reconstruction/Palliation
M1
Advanced/Recurrent
100
How many nodes in N1 vs N2 rectal cancer.
1-3 or 4+
100
Ingredients for FOLFOX
5-FU
Leucovorin
Oxaloplatin
100
There are two drawbacks to pedicled omental flaps in the pelvis, name one.
No skin coverage
Lacks bulk
100
Most common site of rectal cancer metastasis
Liver
100
This is the definition of a T4b lesion in rectal cancer.
Tumor that invades or adheres to adjacent organs.
200
Preoperative workup of rectal cancer includes these four things (name at least 3).
Complete colonoscopy
CEA
CT Chest, Abdomen, and Pelvis
MRI Pelvis or ERUS
200
Standard neo-adjuvant cocktail for advanced rectal cancer.
5-FU
EBRT
200
This muscle can be used as a free flap for pelvic defects.
Latissimus dorsi
200
Metastases to these two organs can be treated with surgical resection.
Liver and Lung
200
These two modalities are used to determine clinical T stage.
MRI
ERUS
300
Spread through this plexus leads to spine mets in rectal cancer.
Batson's
300
Capecitabine is a prodrug of this.
5-FU
300
Flap supplied by this artery.
Vertical Rectus Abdominis Myocutaneous flap (VRAM)
300
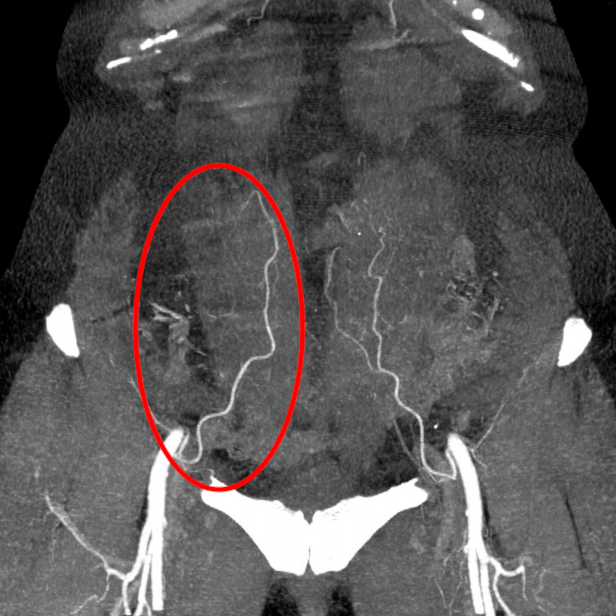
Your patient is 4 years s/p LAR and surveillance CT reveals the following. Estimated functional reserve is 20%. This is his surgical option.
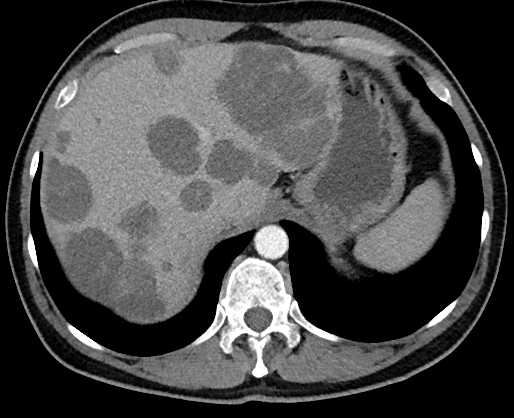
Liver Transplant
300
This operation is used when rectal cancer (especially recurrent) invades the surrounding pelvic organs.
Pelvic exenteration
400
Distal margin in rectal cancer (in cm)
2
400
The dose of Intra-Operative Radiation Therapy
10-15 Gy
400
Three palliative procedures in obstructing rectal cancer. (name two)
Diversion
Fulguration
Laser ablation
400
Median survival after metastastectomy
55 months
400
Lateral recurrence often requires ligation of this vessel for RO resection.
Internal iliac.
500
Criteria for transanal excision, name at least 4.
<30% circumference
<3cm
>3mm margin
Mobile, nonfixed
T1 lesion
500
Can locally recurrent rectal cancer be treated with additional radiation?
Yes
(Double or nothing if you know the dose)
500
The blood supply for this muscle.
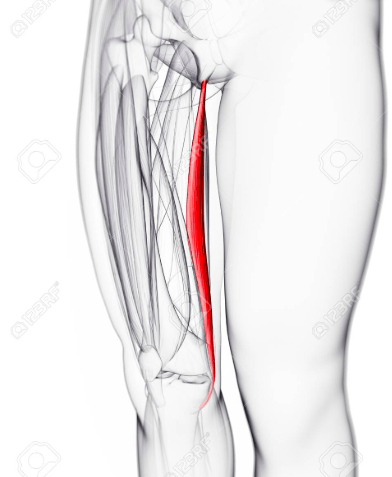
Medial circumflex artery
500
Patient presents with rectal mass. Pelvic MRI shows the mass invading the muscularis propria, with two suspicious mesorectal lymph nodes. Below is from the staging CT. What stage is her disease?
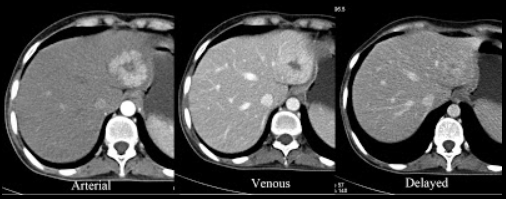
IIIA
500
Transection of the sacrum below this level generally limits GU morbidity.
S3