AIRWAY & RESUS
ECGs
TRAUMA
PAEDIATRICS
TOXICOLOGY
100
What is the first-line oxygen delivery device for a critically hypoxic patient requiring maximal oxygen delivery before definitive airway management?
Non-rebreather mask at 15 L/min.
100
What electrolyte abnormality classically causes peaked T waves?
Hyperkalaemia.
100
What does FAST stand for?
Focused Assessment with Sonography in Trauma.
100
what is the ratio of chest compressions to breaths ACLS neonatal guideline
3:1
100
What antidote is used for opioid overdose?
Naloxone
200
What lactate level is concerning for significant shock?
Generally >2 mmol/L.
200
What is the first-line treatment for unstable broad complex tachycardia?
Synchronised cardioversion.
200
What are the components of the lethal triad
Hypothermia,
acidosis,
coagulopathy.
200
What is the first-line treatment for febrile seizures lasting less than 5 minutes?
Supportive care and antipyretics if needed.
200
What toxidrome is associated with dilated pupils, dry skin and urinary retention?
Anticholinergic toxidrome.
300
A patient becomes profoundly hypotensive after PEEP is increased. Why?
Reduced venous return causing decreased cardiac output.
300
Name 3 ECG features of atrial fibrillation.
Irregularly irregular rhythm, absent P waves, variable R-R intervals.
300
List the indications for activating a massive transfusion protocol.
major haemorrhage actual or anticipated need for 4 units in <4 hours + haemodynamic instability
+/- anticipated ongoing bleeding
shock index >1
300
Name 3 red flags in the febrile neonate.
Poor feeding, lethargy, respiratory distress, temperature instability, mottling, apnoea.
300
Name 3 ECG changes associated with tricyclic antidepressant overdose.
Wide QRS, terminal R wave in aVR, prolonged QT, tachycardia.

400
Name the 4 major categories of shock.
Hypovolaemic, distributive, cardiogenic, obstructive
400
List 4 causes of prolonged QT
Hypokalaemia, hypomagnesaemia, medications, congenital long QT, hypocalcaemia, myocardial ischaemia.
400
What are the types of trauma surveys and what do they consist of
•Primary survey
• initial assessment of a trauma patient, focusing on identifying and managing life-threatening conditions.
•Secondary survey
•Comprehensive head-to toe examination post primary survey to identify any additional injuries
•Tertiary survey
•Is a repeated head to toe examination preformed 24 hours after admission to identify ant missed injuries that may have been overlooked
400
List 4 features of impending paediatric respiratory failure.
Silent chest, reduced consciousness, exhaustion, cyanosis, bradycardia, poor respiratory effort.
400
what is the toxicological frame work commonly used
RRSIDEAD
Resuscitation, Risk Assessment, Supportive care, Investigations, Decontamination, Enhanced elimination, Antidotes, disposition
500
List the reversible causes of PEA arrest.
The Hs and Ts:
- Hypoxia
- Hypovolaemia
- Hydrogen ions (acidosis)
- Hyper/hypokalaemia
- Hypothermia
- Tension pneumothorax
- Tamponade
- Toxins
- Thrombosis pulmonary
- Thrombosis coronary
500
What are the ECG criteria for a STEMI
ECG features >/= 2 contiguous leads of;
>/= 2.5mm STE in leads V2, V3 (men <40yrs)
or
>/= 2.0 STE in leads V2, V3 (men >40yrs)
>/= 1.5 STE in leads V2, V3 in women
>/= 1.0 STE in all other leads
New LBBB meeting sgarbossa criteria
500
list the 6 killer conditions of trauma
• ATOM-FC
•Airway obstruction or disruption
•Tension pneumothorax
•Open pneumothorax
•Massive haemothorax
•Flail chest
•Cardiac tamponade
500
what are specific risk factors for children under 2 that are concerning for a clinically important traumatic brain injury

500
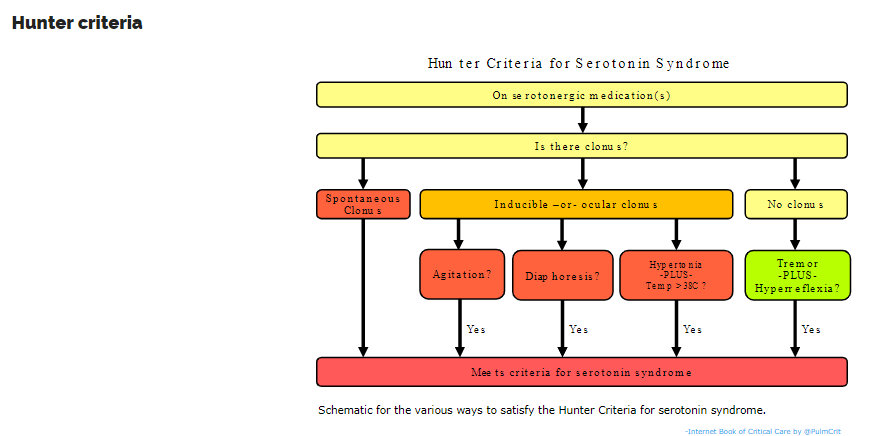
A patient presents agitated, hyperthermic and clonus-positive after taking SSRIs. What is the diagnosis and first-line management?
Serotonin syndrome. Stop serotonergic agents, supportive care, benzodiazepines, cooling.