Rheum 1
Endo 1
Rheum 2
Endo 2
Rheum 3
Endo 3
100
Although effective inflammatory agents in many rheumatologic diseases, these agents have numerous adverse side effects, including osteoporosis, immunosuppression, skin fragility, glaucoma, cataracts, weight gain, diabetes mellitus, and hypothalamic-pituitary-adrenal axis suppression.
- Although effective inflammatory agents in many rheumatologic diseases, glucocorticoids have numerous adverse side effects, including osteoporosis, immunosuppression, skin fragility, glaucoma, cataracts, weight gain, diabetes mellitus, hypertension, psychomotor agitation, osteonecrosis, and hypothalamic-pituitary-adrenal axis suppression.
100
Diabetes mellitus can be diagnosed by an abnormal result in any one of these three tests.
- Diabetes mellitus can be diagnosed by an abnormal result in one of the following screening tests: hemoglobin A1c, fasting plasma glucose, or 2-hour plasma glucose after a 75-gram carbohydrate challenge during an oral glucose tolerance test.
100
The most useful laboratory studies to aid in the diagnosis of rheumatoid arthritis (RA) are rheumatoid factor and these antibodies, which have a specificity of 95% for RA.
The most useful laboratory studies to aid in the diagnosis of rheumatoid arthritis (RA) are rheumatoid factor and anti–cyclic citrullinated peptide (CCP) antibodies; anti-CCP antibodies have a specificity of 95% for RA.
100
The American Diabetes Association recommends this drug class to slow progression of nephropathy and prevent cardiovascular disease in nonpregnant persons with diabetes, hypertension, a urine albumin-creatinine ratio over 300 and GFR under 60.
- The American Diabetes Association recommends an ACE inhibitor or an angiotensin receptor blocker as first-line therapy to slow progression of nephropathy and prevent cardiovascular disease in nonpregnant persons with diabetes, hypertension, a reduced estimated glomerular filtration rate (<60 mL/min/1.73 m2), and an elevated urine albumin-creatinine ratio (≥300 mg/g creatinine).
- Treatment with an ACE inhibitor or angiotensin receptor blocker is not recommended for patients with diabetes who have a normal blood pressure, a urine albumin-creatinine ratio level less than 30 mg/g creatinine, and an estimated glomerular filtration rate level greater than 60 mL/min/1.73 m2.
100
This agent is the "anchor drug" in treatment of rheumatoid arthritis, and can be used as monotherapy or as a component of combination therapy when treating RA.
Methotrexate is the anchor drug in rheumatoid arthritis; it is used as monotherapy and as a component of combination therapy.
Of patients with RA taking methotrexate alone, 30% to 50% achieve remission or low disease activity.
100
Patients with type 2 diabetes should have an eye examination at this timepoint in relation to diagnosis.
Patients with type 2 diabetes should have an eye examination at the time of diagnosis.
200
Radiographic features of this rheumatologic condition include asymmetric joint-space narrowing, subchondral sclerosis, osteophytes, and bone cysts.
Radiographic features of osteoarthritis (OA) include asymmetric joint-space narrowing, subchondral sclerosis, osteophytes, and bone cysts; however, these changes may not be present in early disease, and symptoms may correlate poorly with imaging findings, even in established OA.
200
All patients with adrenal incidentaloma should be evaluated for subclinical Cushing syndrome and this condition.
- All patients with adrenal incidentaloma should be evaluated for pheochromocytoma; those with hypertension or hypokalemia should also be evaluated for primary aldosteronism, and all patients should be evaluated for subclinical Cushing syndrome.
- Initial tests for pheochromocytoma include measurement of plasma free metanephrine levels or 24-hour urine fractionated metanephrine and catecholamine levels; certain medications can affect results and need to be discontinued at least 2 weeks prior to testing -- psych meds, stimulants, and Tylenol
200
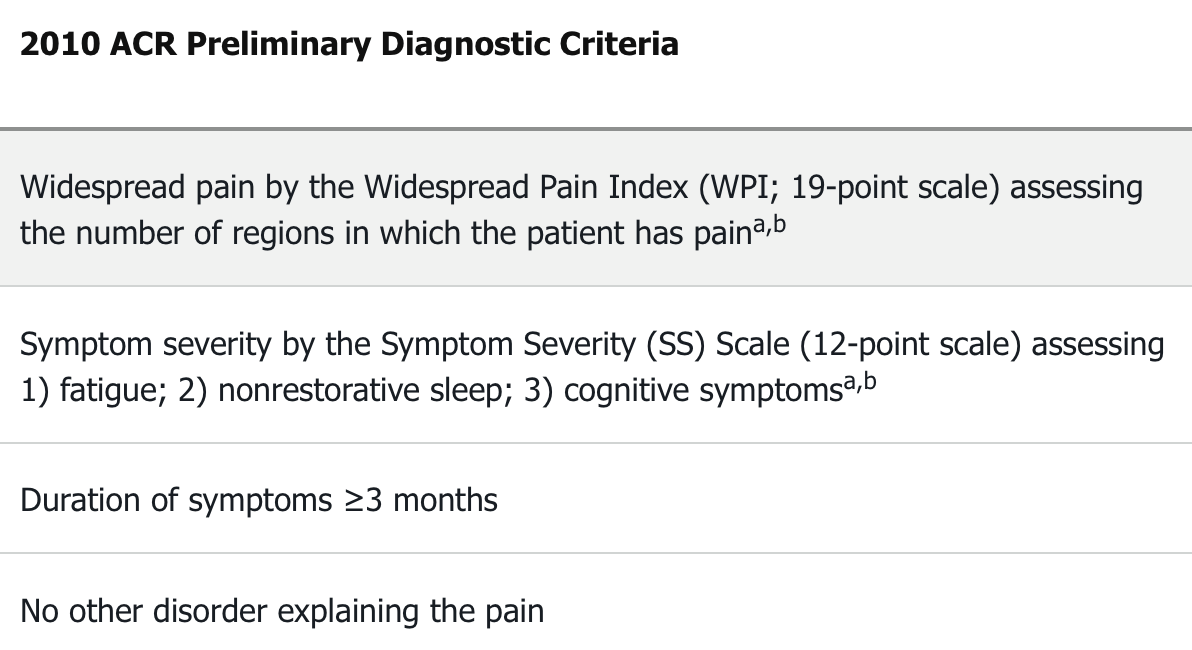
The characteristic features of this complex disorder are widespread chronic pain, fatigue, and sleep disorders. Diagnosis is no longer based upon physician examination findings but rather on a careful characterization of symptoms using a validated scoring tool.
- The characteristic features of fibromyalgia are widespread chronic pain, fatigue, and sleep disorders, which are frequently accompanied by impaired cognitive function, mood disorders, and symptoms such as headache, gastrointestinal symptoms, and paresthesia.
200
Initial tests for Cushing syndrome have similar diagnostic accuracy and include these three diagnostic tests.
- Initial tests for Cushing syndrome have similar diagnostic accuracy and include measurement of 24-hour urine free cortisol, serial late-night salivary cortisols, and the 1-mg overnight dexamethasone suppression test.
- The evaluation of Cushing syndrome involves (1) initial testing followed by confirmatory testing for Cushing syndrome; (2) determining Cushing syndrome as adrenocorticotropic hormone (ACTH)-independent or -dependent; and (3) localizing the source of ACTH in ACTH-dependent disease or confirming the presence of adrenal mass (or masses) in ACTH-independent disease.
200
In patients with spondyloarthritis, this genetic marker is positive in many patients, although it cannot independently confirm or exclude a diagnosis.
In patients with spondyloarthritis, rheumatoid factor and other autoantibodies are typically absent; HLA-B27 is positive in many patients, but it cannot independently confirm or exclude a diagnosis.
HLA = Human Leukocyte Antigen
200
The distinction between primary hyperparathyroidism and this condition can be made by a 24-hour urine collection for calcium and creatinine, which will establish the amount of kidney calcium excretion and will allow evaluation of the calcium-creatinine clearance ratio.
- The distinction between primary hyperparathyroidism and familial hypocalciuric hypercalcemia can be made by a 24-hour urine collection for calcium and creatinine, which will establish the amount of kidney calcium excretion and will allow evaluation of the calcium-creatinine clearance ratio.
300
If antinuclear antibody testing is positive, autoantibodies specific to SLE should be obtained to further characterize the disease, including these two autoantibodies.
- If antinuclear antibody testing is positive, autoantibodies specific to systemic lupus erythematosus (anti–double-stranded DNA, anti-Smith, anti-U1-ribonucleoprotein (mixed connective tissue disease), anti-Ro/SSA, and anti-La/SSB) should be obtained to further characterize the disease.
300
The most common cause of primary hypothyroidism
The most common cause of primary hypothyroidism is autoimmune thyroid gland failure due to Hashimoto thyroiditis, typically associated with thyroid perioxidase antibodies.
300
This drug should be initiated in every patient with systemic lupus erythematosus who can tolerate it, because it can reduce disease-associated damage, prevent disease flares, and improve kidney and overall survival.
Hydroxychloroquine should be initiated in every patient with systemic lupus erythematosus who can tolerate it, because it can reduce disease-associated damage, prevent disease flares, and improve kidney and overall survival.
300
In a patient with suspected Myxedema coma, this medication is administered empirically before thyroid replacement hormone is initiated to treat possible concomitant adrenal insufficiency.
- In addition to aggressive supportive measures, stress-dose glucocorticoids (100 mg intravenous hydrocortisone every 8 hours) are administered empirically before thyroid hormone is initiated to treat possible concomitant adrenal insufficiency.
300
In ankylosing spondylitis, this drug class is recommended as first-line treatment and may help slow disease progression.
In ankylosing spondylitis, NSAIDs are recommended as first-line treatment and may help slow disease progression; physical therapy is the most important nonpharmacologic intervention.
300
For women with preexisting hypothyroidism, levothyroxine dosing can be empirically increased by this percentage when pregnancy is confirmed.
For women with preexisting hypothyroidism, levothyroxine dosing can be empirically increased by 30% when pregnancy is confirmed.
However, those at increased risk of thyroid dysfunction should be screened, which includes those 30 years of age and older; with known hypothyroidism and/or a strong family history of thyroid dysfunction; prior head/neck irradiation; prior neck surgery; positive TPO, TSI, or TRAb status; or other autoimmune disorders.
400
In patients with this rheumatologic disease, management of sicca is centered on preservation of moisture and relief of symptoms; extraglandular involvement is treated with immunosuppression.
In patients with Sjögren syndrome, management of sicca is centered on preservation of moisture and relief of symptoms; extraglandular involvement is treated with immunosuppression.
400
This drug is recommended by the American Diabetes Association for patients with diabetes and clinical atherosclerotic cardiovascular disease as part of the glucose control regimen.
Empagliflozin (Jardiance) or liraglutide (Victoza) is recommended by the American Diabetes Association for patients with diabetes and clinical atherosclerotic cardiovascular disease as part of the glucose control regimen.
400
Elevated creatine kinase and progressive, symmetric, proximal muscle weakness, without pain or tenderness, are characteristic of these two conditions. Unlike a related condition, these pathologies do not have skin involvement.
Polymyositis and dermatomyositis are characterized by progressive, symmetric, proximal muscle weakness, leading to decline in physical function; dermatomyositis is further defined by cutaneous involvement.
- Vs. Muscle tenderness should prompt consideration of infectious, thyroid, or drug-induced myopathies.
400
This bone disease may present with localized symptoms, but it is most commonly diagnosed in asymptomatic older patients presenting with elevated alkaline phosphatase levels or incidental radiographic findings.
- Although Paget disease of bone may present with localized symptoms, it is most commonly diagnosed in asymptomatic older patients presenting with elevated alkaline phosphatase levels or incidental radiographic findings.
400
Initial treatment for most inflammatory myopathies consists of this drug class, with additional immunosuppressives (most commonly methotrexate and azathioprine) often required to control inflammation.
Initial treatment for most inflammatory myopathies consists of glucocorticoids, with additional immunosuppressives (most commonly methotrexate and azathioprine) often required to control inflammation or serve as glucocorticoid-sparing agents.
400
Initial treatment of moderate to severe hypercalcemia is aggressive hydration to replete volume loss and increase kidney excretion of calcium; loop diuretics are not recommended unless one of these two conditions is present, in which case volume expansion should precede the administration of loop diuretics.
Initial treatment of moderate to severe hypercalcemia is aggressive hydration to replete volume loss and increase kidney excretion of calcium; loop diuretics are not recommended unless kidney failure or heart failure is present, in which case volume expansion should precede the administration of loop diuretics to avoid hypotension and further kidney injury.
500
Interstitial lung disease is currently the main cause of disease-related mortality in patients with this "systemic" rheumatologic condition.
Lung involvement in systemic sclerosis includes pulmonary arterial hypertension and interstitial lung disease (ILD); ILD is currently the main cause of disease-associated mortality.
ACE inhibitors can be lifesaving in patients with scleroderma renal crisis and should be titrated to control blood pressure even in the presence of rising serum creatinine.
500
In the initial evaluation of a thyroid nodule, patients with a suppressed thyroid-stimulating hormone level are evaluated with this test.
Patients with a suppressed thyroid-stimulating hormone level are evaluated with thyroid scintigraphy; those patients with normal or elevated thyroid-stimulating hormone are evaluated with ultrasonography.
500
Guidelines currently recommend a “treat-to-target” approach in gout, reducing the serum urate level to less than this value in patients without tophi.
The American College of Rheumatology and the European League Against Rheumatism both recommend a “treat-to-target” approach, reducing the serum urate level to less than 6.0 mg/dL (0.35 mmol/L) in patients without tophi and less than 5.0 mg/dL (0.30 mmol/L) in patients with tophi.
500
Glucocorticoids prescribed in greater than physiologic doses for this amount of time or longer should be tapered off to allow recovery of the pituitary-adrenal axis.
- Glucocorticoids prescribed in greater than physiologic doses for 3 weeks or longer should be tapered off to allow recovery of the pituitary-adrenal axis.
500
Basic calcium phosphate deposition can rarely cause this condition named for a midwestern city, an inflammatory arthritis and periarthritis of the shoulder occurring in elderly women that leads to progressive destruction of the rotator cuff and glenohumeral joint.
Basic calcium phosphate deposition can rarely cause Milwaukee shoulder, an inflammatory arthritis and periarthritis of the shoulder occurring in elderly women that leads to progressive destruction of the rotator cuff and glenohumeral joint; diagnosis is usually clinical.
500
When treating osteoporosis, a drug holiday can be considered after this many years of oral bisphosphonate therapy in post-menopausal women who are not at high fracture risk.
- A drug holiday can be considered in postmenopausal women who are not at high fracture risk after 3 years (intravenous) to 5 years (oral) of bisphosphonate treatment.