Causes
Dx
Tx
T/F
Clinical cases
100
Endocrine disorder characterized by excess cortisol, central obesity, abdominal striae, and moon facies
Cushing's syndrome
*rare cause of resistant HTN but can screen w/ 23h urine cosrtisol, MN salivary cortisol or low dose dex suppression test if + cushingoid features
100
Diagnosing HTN: BP >= 130/80 averaged at least this many times over a period of weeks-months.
3
*single measurement okay if >= 160/100 and HTN related organ damage (high pre-rest prob in CKD, HF/LVH) OR BP >= 180/120
100
This medication is used as first line for primary hyperaldosteronism?
Spironolactone
*start low dose and CTM lytes closely in first months
*significant benefit regardless of pimary aldosteronism
100
You need to stop some medications when screening for primary hyperaldosteronism
You get the points no matter what :)
Do NOT need to stop ACE/ARBs. If possible, stop spironolactone x1m but can also test while on this. You may get a false negative but not many things that cause a false positive.
100
60 y/o with HTN, HLD, T2DM here for a f/u. His BP is 135/89 in clinic today. He is on max dose amlodipine, losartan, HCTZ. Is this resistant HTN?
a. no, he is w/in goal b. yes, BP is uncontrolled on 3 meds c. maybeeee
Will get points for a and c
BP still above goal 130/80 on 3 meds; make sure legs are uncrossed x 5m, empty bladder, no clothing over arm and correct cuff size! Confirm pt is taking meds (>80% of doses).
200
Kidney related cause of secondary HTN due to atherosclerosis in older folks or fibromuscular dysplasia in younger folks
RAS: renal artery stenosis
*suspect RAS in pts > 55 w/ atherosclerosis and new onset HTN
*suspect in young patients with HTN
200
Suggestive clinical features of RAS: elevated Cr (>= .5-1) after starting this medication(s)
ACEi or ARB
200
In a patient with aldosteronism producing adenoma, this is the definitive treatment to cure HTN
Adrenalectomy
*adrenal CT/MR if surgery is being considered, imaging has high false positive and false negative rate for active adrenal adenomas
200
You should be checking renin/aldosteronism levels in the PM
False; check in the AM (0800)
*both aldo and renin have a diurnal variation, peaking in the AM and declining in the day
*BP and therefore renin changes with position. When going from laying to sitting/standing, BP temp decreases so RAAS is activated.
200
42 y/o with BMI 40, chronic fatigue, and uncontrolled HTN on 2 antihypertensive agents who came in for a f/u appt. The partner tells you that the patient snores really loud. Next steps?
Sleep study; OSA is one of the most common causes of resistant HTN
300
Catecholamine secreting tumor that can cause secondary HTN
Pheochromocytoma
*rare, about 1/10,000, most common in middle-aged adults
*positive if metanephrines are >4x ULN
300
Pheochromocytoma triad
HA, sweating, palpiations
300
The ACC and AHA recommends considering revascularization for RAS in patients with:
a. resistant HTN b. rapidly declining renal fxn c. CHF d. all of the above
All of the above
*med management FIRST (ACE/ARB has mortality benefit)
*revasc second line if unable to tolerate meds/uncontrolled BP
*CORAL (2014 study) showed no difference in medical tx (ACE/ARB) vs stenting (not in FMD, flash pulm edema, AKI)
300
Majority of patients with primary hyperaldosteronism have an abnormal K
False -- 60% of patients with primary hyperaldosteronism have normal K so normal K does NOT r/o primary hyperaldosteronism
300
38 y/o who comes in for new PCP appointment. You notice their BP is controlled on 3 antihypertensive agents. They also take some OTC meds several times/week. Which OTC med might they be taking that could also be increasing their BP?
NSAIDs, decongestants (pseudoephedrine), OCPs, antidepressants (TCAs, SSRI), olanzapine, immunosupressants (tac), herbals (ginseng), prednisone; EtOH, cocaine
400
This adrenal disorder is the most common cause of secondary HTN in middle aged adults
Primary hyperaldosteronism (Conn's syndrome): excessive aldosterone
*about 8% of all pts w/ HTN and 20% of pts w/ resistant HTN
400
Best initial test for hyperaldosteronism?
aldosterone/renin
*positive if ARR >= 20, esp if aldosterone >15
*excellent sens/spec if ARR > 30 and PAC > 20 and hypoK
400
In CKD, thiazide diuretics lose efficacy at this eGFR
eGFR < 30
*switch to loop diuretics; salt restriction and diuretics are very effective
400
The severity of HTN correlates with severity of OSA in patients who have secondary HTN d/t OSA?
True
400
28 y/o with a PMH of MDD who was seen by another provider 3 weeks ago for a HA and palpitations. They ordered serum metanephrine which came back elevated (1xULN). Next steps?
False positives: venlafaxine, TCAs, adrenergic receptor agonists (decongestants, amphetamines)
500
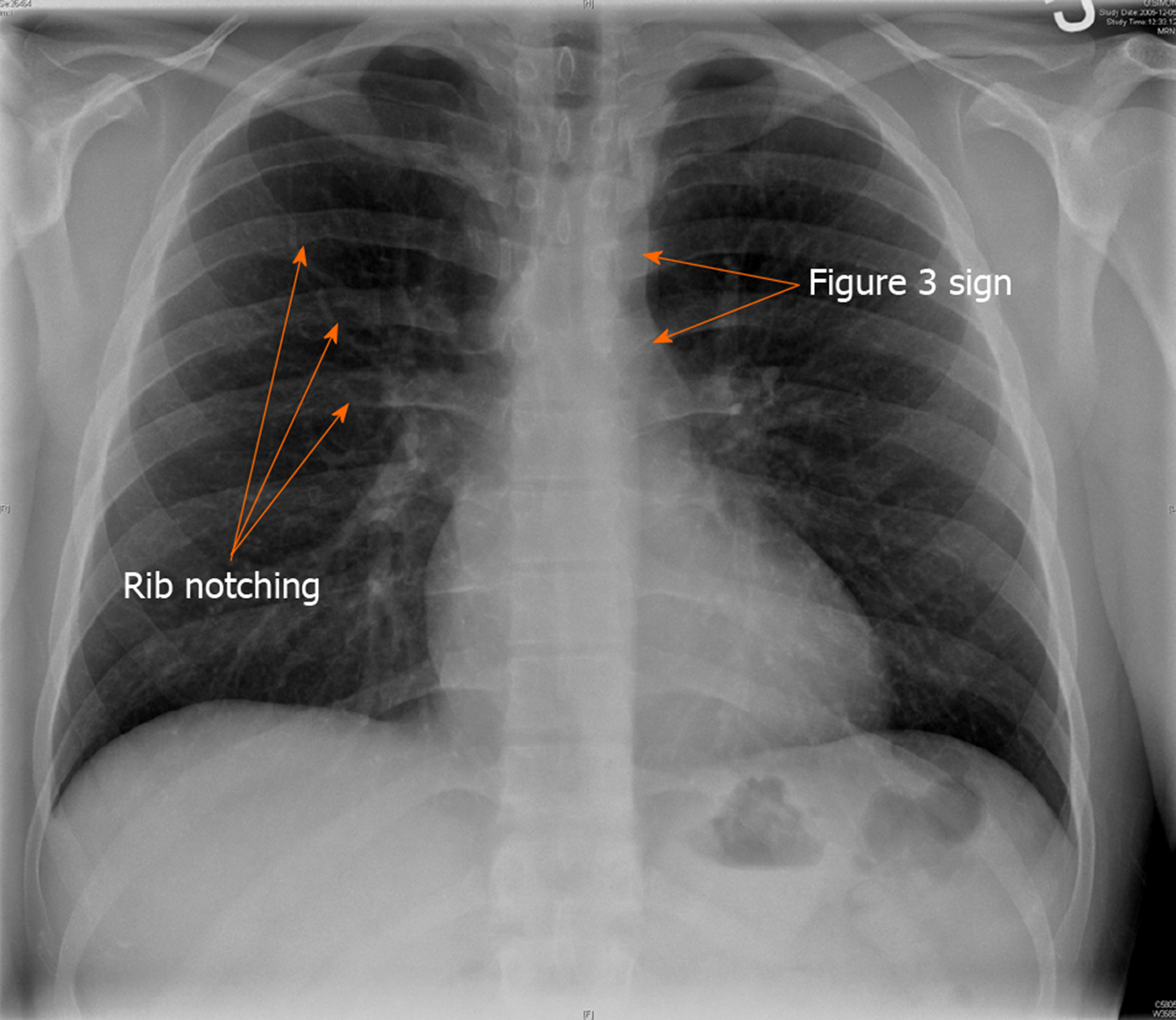
Patient w/ upper extremity HTN, delayed or decreased femoral pulses
Coarctation of the aorta
*common cause in children but may not be detected until adulthood because asx
*classic figure 3 sign or rib notching

500
Indications for further w/u of possible secondary etiology:
1. early or late onset HTN 2. severe accelerated course 3. resistant HTN
Resistant HTN is defined as BP above goal 130/80 despite being on how many antihypertensive agents
3
*max dose, different classes, if tolerated one of the 3 should be a diuretic
*RH inc risk of CV events by 50%+ compared to primary HTN
500
The use of CPAP been shown to help:
a. reduce BP b. reduce strokes c. reduce MIs d. all of the above
a. reduce BP
RCTs have not shown that CPAP reduces CV events (mortality, MI, stroke)
500
Approximately 30% of adults w/ HTN have a secondary cause
FALSE - 5-10% (AAFP)
500
65 y/o with PMH of obesity, CAD with new HTN and an abdominal bruit on physical exam. Next steps?
MRA or CTA; MRI > CT since it can determine degree of stenosis, CTA more sensitive for FMD
if MRI and CT angiography are CI, you can use duplex US (takes 2 h, challenging if larger habitus)
*med management FIRST; c/f RAS in patients > 55 with new onset severe HTN