massive blood
ventilator
pacemaker
pumps
accreditation
anything goes
100
This should be given early on with any non-GI bleed
TXA give within 3hours of start of bleed
100
with PAV
RR is usually higher than norm
volumes are usually ... than norm
lower
This is ok as long as the pt is alright- must be more than 4ml/kg IBW
100
under sense can lead to
overpace- R on T
100
Signs/Symptoms of L.A.S.T.: early
Early Signs: CNS: numbness/tingling around the lips, metallic taste, tinnitus, restlessness, and tremors.
Late Signs: Cardiac: tachycardia and hypertension THEN bradycardia and hypotension, leading to cardiac ventricular arrhythmia, seizures, respiratory arrest, and cardiac arrest.
100
After calling TGLN what are you to do with the number- 2 things
enter it into meditech AND document on kardex
100
SBAR stands for:
situation
Background
Assessment
recommendation
All calls to HCP should use this to provide focused information
200
This is to be given to all obs pts at the start of a MHP
Fibrogen
200
sign of brain death could be ( from the vent point of view)
not breathing above the vent anymore or apnea alarms
200
Pt has a pacemaker you can use the medical directive if:HR less than 40
and one of the following
SBP less than 80
Decreased LOC
Resp issues and ???
chest pain
200
with an epidural we check these with ice
dermatomes
both sides high/low dermatomes
200
> @ D/C are all examples of
do not use abbreviations
200
longer longer longer drop and start again is this type of heart block-
2degree type 1
Wenckebach phenomenon

300
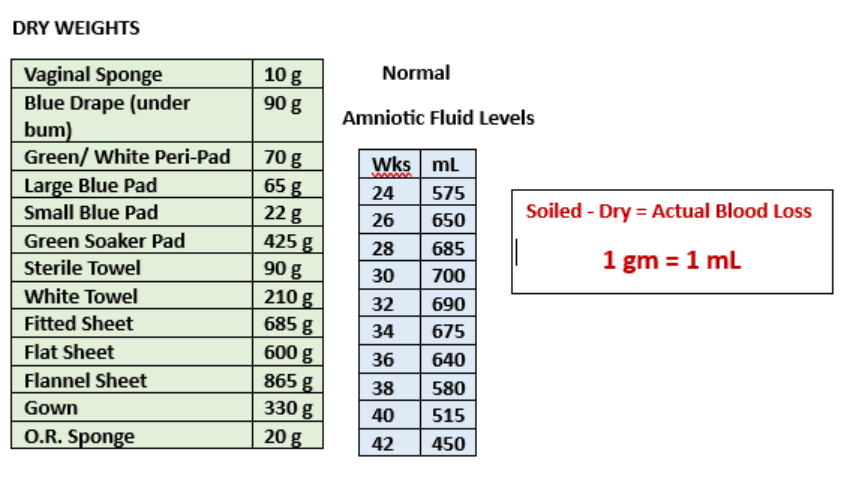
with OB patient .... of the blood soaked pads is essential
weighing
300
with the new anchorfastguard we should be moving the ETT side to side every:
4h
300
MV is also called
sense
300
3 Cardinal Signs of Epidural Hematoma:
- unexplained progression of motor +/- sensory block
- increasing diffuse back pain
- bowel or bladder dysfunction
300
What is the GIFT + stand for?
G- GCS 3 or grave prognosis
I- injured brain
F- family asking questions re organ/tissue
T time limited - ?one way extubation is being talked about
+- MAID pt
300
when you give blood products you are also giving?
citrate- prevents clotting in blood bags but bind Calcium - watch for hypocalcemia
400
with OBs pt the fundus should be
bone hard
400
recruitment maneuvers are done to open up de- recruited lung areas primarily in these pts:
ARDS
400
this must be updated to paced
on monitor- the little heart needs to be white
400
PRIMARY risk factor for epidural hematoma is
anticoagulant therapy
400
root cause analysis is the goal of:
quality reviews
NOT to assign blame
400
refeeding syndrome is when a malnourished person begins feeding again The major electrolyte involved with this is:
phosphate- will go very low
may also feature abnormal sodium and fluid balance; changes in glucose, protein, and fat metabolism; thiamine deficiency; hypokalaemia; and hypomagnesaemia
This kills if we do not look out for it
500
abd pressure monitoring is essential to pick up early signs of
compartment syndrome
500
persistent cuff leaks in an intubated pt may be a sign of
displace/mispositioned ETT
do not inflate with more air- call the RT
500
fibrin build up in the pacer lead can lead to loss of sense and
loss of capture
500
Local anesthetic systemic toxicity is a rare but known complication of epidurals - the kit is where?
The treatment is :
med room on top of pyxis cabinets
intralipids- NOT SMOF
500
it is essential that all admitted pts with existing open areas have this documented in
meditech- admission assessment
there is section where you can tick
if not then it counts as our wound
500
for CAP if there is a thought the pt may have atypical infection a urine will be asked to be sent for:
a: legionella
b: Chlamydia
c:Mycoplasma
Legionella- more common in summer with air conditioning- if thought to be atypical Azithromycin will be added
600
one item we can do from the start to prevent diamond of death complications?
keep pt warm- even if only over the legs
bairhugger
600
Twice a day we are to complete a ... assessment on all vented pts
SAT
600
balloon must be except during insertion
down and locked
600
tracing and labeling of every line is critical to prevent
accidental misconnects eg epidural to IV, feeds to epidural, IV to feeds
600
these infection rates are publicly reported
VAP
CLI
Cdiff
MRSA
600
The key for PCA/epidural is ?
pyxis called key- put it back when used