Snow Day
Biases
Obesity
Outpt GI
Doctors in Media
100
What is a nor'easter and why is it called that?
Coastal storm that moves up the East Coast, characterized by cold winds from the artic colliding with hot warm air in the atlantic creating large storms that travel north-east

100
According to our GR speaker, what population is experiencing increased implicit bias, while most biases appear to be decreasing?
Obese/overweight patients - 1 min less time spent in patient rooms, increasing biases seen on Harvard implicit biases test.
100
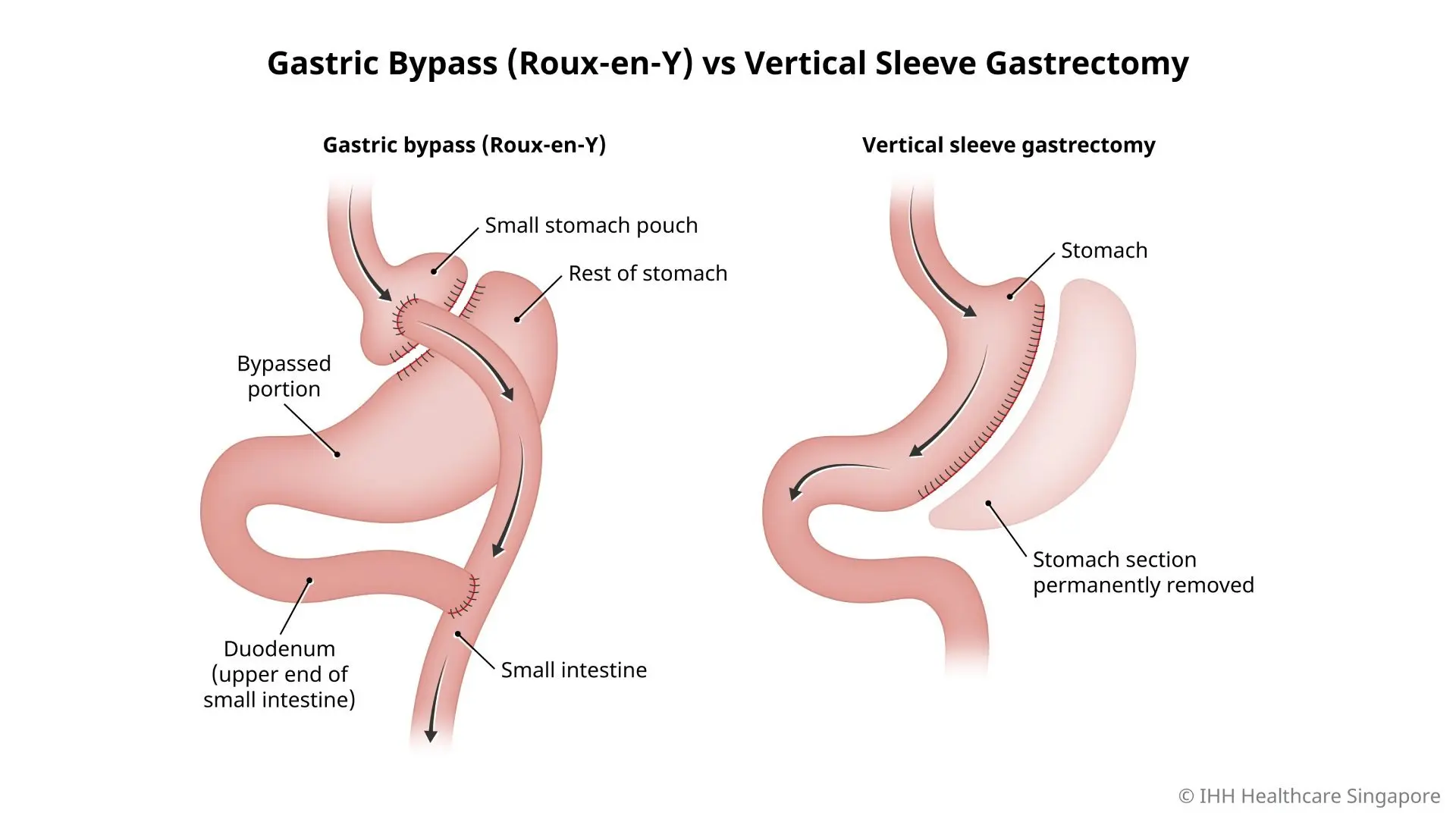
Draw the anatomy of a Roux en Y and Gastric Bypass surgery. Which usually causes more excess weight loss?
Roux en Y - 60 - 70% EWL
Sleeve - 50 - 60% EWL
100
How is a diagnosis of eosinophillic esophagitis established and what biologic is FDA approved for EoE?
EGD w/ biopsy w/ > 15 eosinophils per high power field.
Treat with dietary elimination and, if symnptomatic, PPI or oral topical corticosteroids
Dupilimumab (Dupixent) is anti-IL4 + IL-13
100
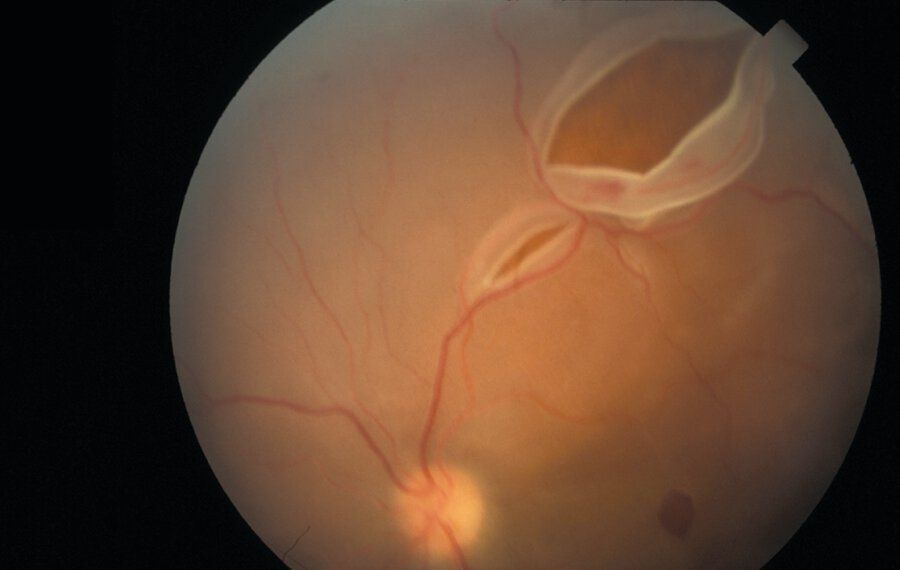
A 68-year-old woman is evaluated for reduced vision and flashing lights in her left eye that began this morning. This was preceded by floaters in her left eye, first appearing several days ago and now with increasing frequency. She has no other symptoms. Medical history is significant for myopia. She takes no medications.
On physical examination, she has an inferior visual field defect in her left eye. Visual fields in the right eye are normal. Pupils are equally round and reactive to light and accommodation. Visual acuity is 20/60 in the left eye and 20/20 in the right eye. Nondilated funduscopic examination is normal.
What would Glaucomaflecking diagnose? (WWGD)

Retinal detachment - painless visual field defect. Risk factors include age, myopia, and recent cataract surgery.
Urgent opthamology evaluation -
200
What is first line for Raynaud's phenomenon and what is one alternative agent?

1) Dihydropyridine CCB - nifedipine, amlodipine - vasodilation -> decreases frequency and severity (30-60%)
2nd line - sildenafil (good for 2nd Raynauds), topical nitrates, bosenten (good in SS for digital ulcers)
200
What is an upstander?
Upstander - you all: a person who chooses to intervene when witnessing bias/microaggressions
200
What infection should you consider screening gastric bypass candidates as a part of their evaluation?
H pylori
If positive, should undergo eradication with confirmatory testing prior to surgery.
increases risk of marginal ulcer formation post-operatively.
200
Which, if any, patients with normal AST/ALT and no documented steatosis on imaging should undergo screening for MASLD using FIB-4, according to AASLD?
All patients with TIIDM
Patients with >=2 metabolic risk factors (overweight/obese, HTN, dyslipidemia, pre-TIIDM, metabolic syndrome)
Should also screen those with steatosis on imaging or if you suspect MASLD
Mildly abnormal ALT does not mean auto-screen
200
This physician, known as the father of epidemiology, traced this pathogen to the Broad Street water pump in London in 1854, for which the mainstay of treatment to this day remains.
John Snow
Cholera
IVF or Oral rehydration therapy in low resource settings - mainstay of therapy
Tx doxy 300 x1 or azithro 1 g x1 - reduces duration of symptoms
300
A 22-year-old man is evaluated in the ED after being pulled from a lake. Immersion time is estimated to be 2 hours. He was found unresponsive, pulseless then intubated, and advanced life support was initiated. On arrival at the ED, pulse had returned and cardiopulmonary resuscitation was stopped. Mechanical ventilation was initiated, and intravenous fluids were administered. Wet clothes were removed.
On physical examination, blood pressure is 92/60 mm Hg. Temperature by an esophageal probe is 27.6 °C (81.7 °F). There are no signs of trauma. Glucose us 88, K 5.4, pH 7.28, CO2 36, PO2 110
What is the next best step in management?
Active internal rewarming
Cardiopulmonary bypass warming
Hemodialysis
Passive rewarming
The most appropriate treatment is active internal rewarming. This patient has severe hypothermia, defined by a core temperature of less than 28.0 °C (82.4 °F) in the setting of ongoing coma or cardiovascular collapse. If a severely hypothermic patient becomes pulseless and requires resuscitation, it is reasonable to continue cardiopulmonary resuscitation for a prolonged period until the patient can be rewarmed. Methods of internal rewarming include infusion of heated intravenous crystalloid solution as well as lavage of the peritoneal or pleural cavities with warm fluids. During active rewarming, core temperature should be monitored with an esophageal temperature probe, as rectal and bladder temperatures will lag behind the rising core temperature during the rewarming process.
Extracorporeal support, including cardiopulmonary bypass, is recommended for severely hypothermic patients in cardiac arrest because it maximizes the rewarming rate and can provide hemodynamic support.
Hemodialysis can be used for warming, depending on the clinical circumstances. Acid-base and electrolyte abnormalities are common in hypothermia. These values, along with markers of coagulopathy, will improve with rewarming but should be serially measured. The patient has metabolic acidosis and hyperkalemia, but neither is severe enough to warrant hemodialysis, and rewarming can be accomplished by other means.
Hypothermic patients who are shivering will passively rewarm themselves if given adequate insulation to prevent heat loss, but as hypothermia progresses, shivering stops. For core temperatures of 28.0 °C to 35.0 °C (82.4 °F to 95.0 °F), active external warming is usually sufficient. This consists of warming blankets and forced warm air. For temperatures less than 28.0 °C (82.4 °F) and for patients who fail to respond adequately to active external rewarming, active internal rewarming methods should be applied.
300
A 50-year-old man is evaluated for three episodes of hematochezia in the past 2 months. His last colonoscopy was 5 years ago, and the results were normal. His family history includes colon cancer in his father, diagnosed at age 55 years. The patient prefers to pursue a stool-based colon cancer screening strategy.
A stool-based test that is 95% accurate in diagnosing colon cancer in average-risk individuals is available. The accuracy and effectiveness of this test were established in a randomized controlled trial.
Which of the following best explains why the evidence does not support performing this stool-based test in this patient?
Impracticable number needed to screen
Lack of external validity
Low level of evidence
Presence of lead-time bias
Lack of external validity (generalizability) is the best explanation for why the stool-based test is not appropriate for this patient. External validity is the extent to which the study results can be applied to settings other than the study setting. In this situation, the presence of hematochezia and a significant family history increase the expected prevalence of colon cancer above what would be expected in an average-risk patient, limiting the ability to apply this test, which has acceptable performance in average-risk patients, to patients with a higher pretest probability. Specifically, a negative test result in this high-risk patient cannot reliably exclude the presence of colon cancer as well as it could in an average-risk patient.
The number needed to screen is the number of patients who would need to undergo a screening test to prevent one death or adverse event. It is calculated as the reciprocal of the absolute difference in deaths in the screened versus unscreened (or other comparator) population. This statistic is not applicable to situations in which diagnostic testing is indicated.
The strongest experimental design is the randomized controlled trial. However, the level of evidence is not relevant in this situation because the fundamental flaw is the inappropriate use of a screening test in a population for which it is not intended.
Lead-time bias is an artifactual increase in survival due to earlier diagnosis of disease from a screening test. Lead-time bias has no bearing on why a stool-based colon cancer screening strategy is inappropriate for a high-risk patient.
300
Define excess body weight, total body weight, and ideal body weight
EBW = Total body weight - ideal body weight (BMI 25)
Ex - 5'6 person IBW about 150
if they weigh 250 and lose 50 lbs they have lost 50% of EBW, but only 20% of TBW
300
Name 5 alarm symptoms that warrant EGD evaluation for malignancy in patients with a new or chronic diagnosis of GERD
Dysphagia/oodynophagia, weight loss, GI bleed, IDA, persistent vomiting, anorexia, new onset >50
300
This fictional doctor is rumored (sadly not true) to be based off Jory Goldberg at PMPMC and would advise one of his patients with SLE and nephritis who is desiring pregnancy that this/these medication/medications are safe to continue in pregnancy.

House

Hydroxychloroquine is safe and should be ALWAYS continued. Azathioprine is not routinely used but safer than others and good for flare prevention of nephritis. Steroids can be used for flares. Tacro also safe in pregnancy.
Avoid teratogenic therapies - mycophenolate, methotrexate and belimumab
Cyclophosphamide a/w infertility - avoid in those desiring pregnancy
400
What is the definition of a blizzard (4)?
Sustained winds or frequent gusts ≥ 35 mph (56 km/h)
Considerable falling and/or blowing snow
Visibility reduced to ≤ ¼ mile (400 meters)
Conditions lasting at least 3 hours
400
Define lead-time bias
Lead-time bias occurs when early detection artificially results in an increase in measured survival. The time between early detection and clinical diagnosis is mistakenly counted as survival time; however, only the measured time with diagnosed disease, not survival time, has increased
400
List all FDA approved indications for GLP-1 agonists.
T2DM: Ozempic, Rybelsus, Trulicity, Victoza, Byetta, Bydureon, Adlyxin, Mounjaro
Weight loss (obesity): Wegovy, Saxenda, Zepbound
CV risk reduction (with T2DM): Ozempic, Victoza, Trulicity
CV risk reduction (obesity w/o diabetes and established CVD): Wegovy
OSA in obesity: Zepbound
400
You get a patients first routine screening colonoscopy report back at age 45. He had 1 8 mm adenoma with villous pathology and low-grade dysplasia in the descending colon. It is recommended he repeat screening in 3 years.
He asks what does this mean for his children? When should they start getting CRC screening?
First-degree relatives of patients with advanced polyp (>10 mm, villous pathology or high grade dysplasia) should have CRC screening 10 years before the earliest CRC or advanced adenoma detected - at age 35 for his children
400
This physician/playright, for whom the literary trope of depicting a weapon only if it will be used during the story is named, died at 44 from this chronic infection which would be treated with which medication/s for what duration today?

Anton Chekhov
Checkhov's Gun
Isoniazid (INH) + rifampin (RIF) + pyrazinamide (PZA) + ethambutol (EMB) x2mo, followed by INH+RIF x4mo
500
A 63-year-old man is evaluated for an 8-week history of a spreading rash on the feet and legs, fatigue, and arthralgia.
On physical examination, vital signs are normal. The rash is shown. Some lesions are palpable. He cannot extend his left wrist. Findings on pulmonary, cardiac, and gastrointestinal examinations are unremarkable. There are no swollen or tender joints.

ESR 110, ALT 93, AST 89, C3 113, C4 undetectable, Cr 2.1, RF 118, CCP undetectable, UA 2/ 2+ blood, 2+ prot, dysmorphic erythrocytes
Cryoglobulinemic vasculitis - specifically Type II/III. Clonal/polyclonal immunoglobulins that precipitate in serum at < 37 - hence why they deposit in small/medium vessels and peripheral tissue.
Cryoglobulinemia include cutaneous involvement (90%) (palpable purpura, digital ischemia, ulcers, necrosis, and livedo reticularis), peripheral neuropathy, arthralgia, and glomerulonephritis (usually membranoproliferative).
Labs include depressed C4 complement and low CH50, as well as a positive rheumatoid factor result.
Strong Hep C association
500
Compare and contrast
Anchoring
Premature closure
Diagnostic momentum
Anchoring = Fixating on an initial piece of information. Disproportionate weighting of early data that influences the interpretation of subsequent information.
Premature closure - Stopping the diagnostic process too early. Accepting a diagnosis and discontinuing the diagnostic process before the data necessary to establish the diagnosis have been obtained.
Diagnostic momentum - Accepting a prior diagnosis without re-evaluation. A diagnosis is suggested early in the diagnostic process, and the diagnostic evaluation continues to move toward that diagnosis even if the data do not support it.
500
How did the 2022 guidelines from the metabolic and bariatric surgery change regarding candidates for surgery by BMI alone and by BMI with comorbid conditions?
BMI alone >40 changed to >35
BMI w/ metabolic disease >35 changed to >30
BMI thresholds in Asian population BMI > 27.5 with comorbities and > 30 for BMI alone
500
What does the American College of Gastroenterology recommend for the work-up of male and post-menopausal patients with iron deficiency anemia?
Celiac serology
H pylori testing
Bidirectional endoscopy (EGD + colonoscopy)
500
This 2025 Emmy winner of lead actor in this drama series holds the record for the longest run on a primetime medical series (ER, 1994-2005).
Noah Wyle - The Pitt
