Donatello
Topochico
Shawshank
Yannetti Spaghetti
Patty Daddy
100
Why is fentanyl generally avoided as a continuous infusion in the OR?
Prolonged context-sensitive half-life
With prolonged infusion, the drug accumulates in peripheral tissues and re-distributes back to plasma, dramatically prolonging its duration of action and risking postoperative respiratory depression
100
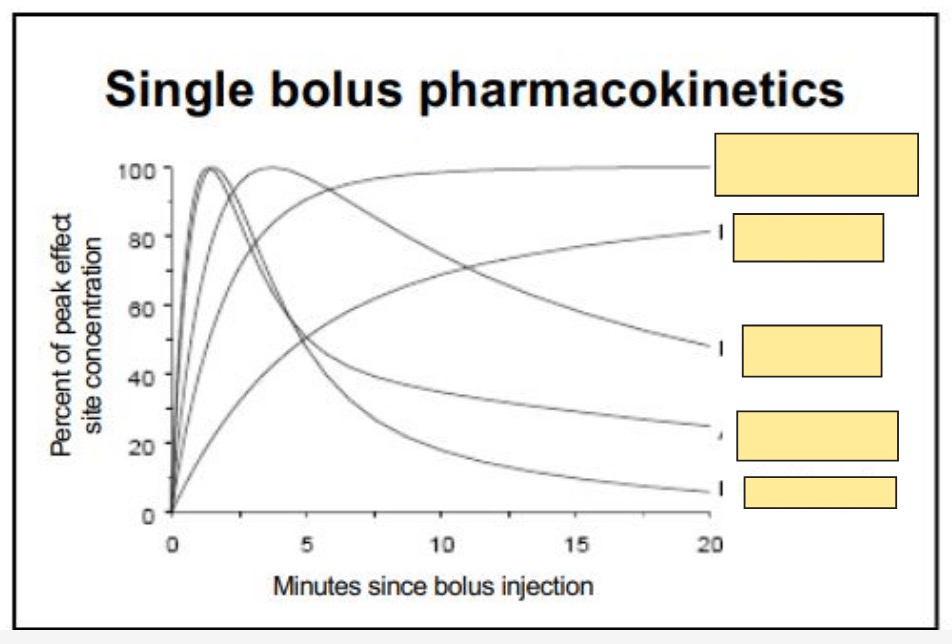
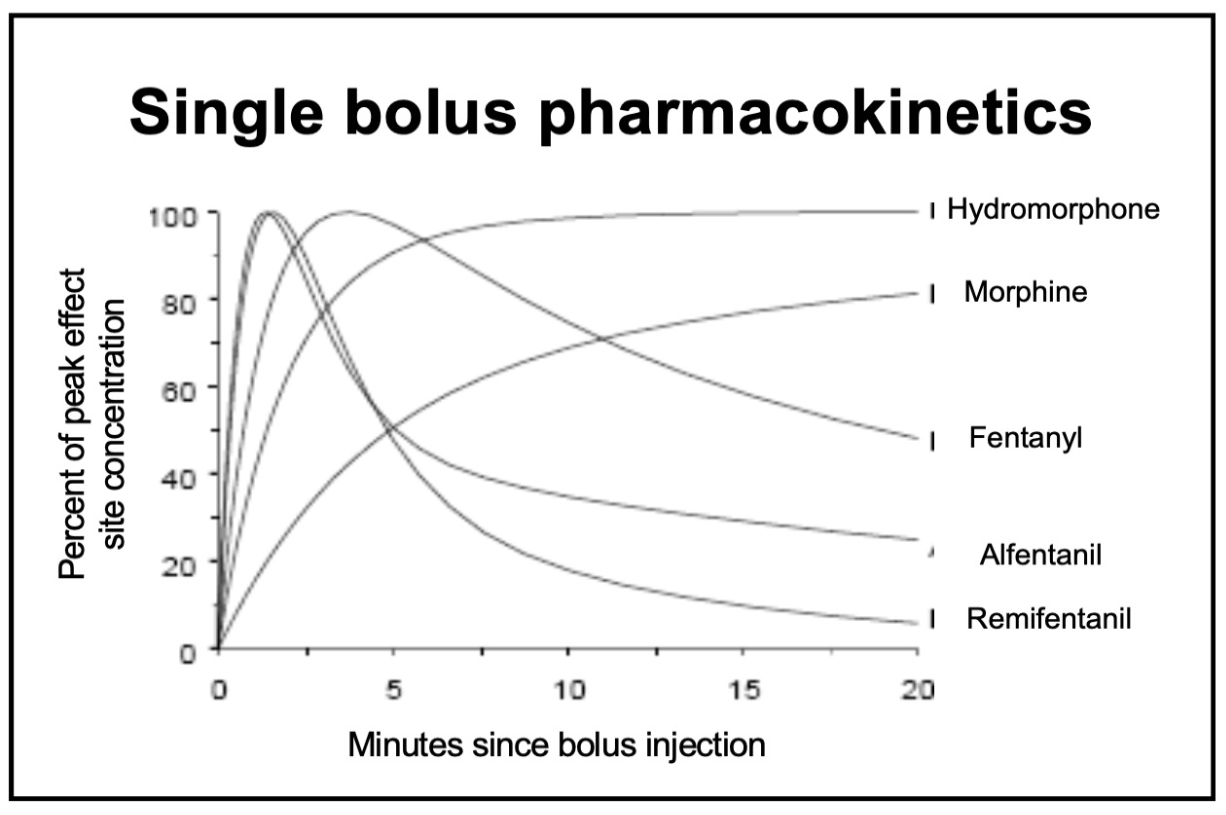
What is the peak onset time of IV fentanyl, and why is this clinically important during induction?
Fentanyl peaks in 3–5 minutes.
If administering fentanyl to blunt the sympathetic response to laryngoscopy, you must wait 3–5 minutes before proceeding — otherwise peak effect has not yet occurred.
100
What enzymatic pathway is responsible for remifentanil metabolism, and why does this make its half-life context-independent?
Plasma esterases metabolize remifentanil. Because this is a fixed, non-organ-dependent pathway, the drug is eliminated at a constant rate regardless of infusion duration — the half-life remains 5–10 minutes no matter how long the infusion.
100
Which opioid receptor subtype is primarily responsible for respiratory depression, and which subtype mediates supraspinal analgesia?
μ2 mediates respiratory depression
μ1 mediates supraspinal analgesia
100
Which metabolite of hydromorphone is capable of causing neuroexcitation? Does this metabolite provide any analgesia? Which patient population requires precaution?
Hydromorphone-3-glucuronide. No analgesia. Accumulation can become clinically relevant in renal insufficiency.
200
For what specific postoperative indication is meperidine most commonly reserved in modern anesthesia practice?
Treatment (and prevention) of postoperative shivering upon emergence. Typical dose: 12.5–25 mg IV.
200
You plan to give IV hydromorphone near the end of a case for post-op analgesia. How long should you allow before expecting peak effect?
Up to 15 minutes. Hydromorphone has a peak onset of 5–15 min IV.
Patience is required to avoid inadvertent overdose while waiting for full effect.
200
How does sufentanil differ from remifentanil in terms of context-sensitive half-life, and how does this influence its clinical use?
Sufentanil has some context-sensitivity (unlike remifentanil), meaning it accumulates with prolonged infusion.
This is desirable when a postoperative analgesic tail is needed. It is preferred for cases with significant intraoperative stimulation AND expected postoperative pain.
200
Methadone is supplied as a racemic mixture of 2 enantiomers, each one acting upon a distinct receptor.
What are these 2 receptors and how does the enantiomer act upon it (agonist/antagonist)?
L-methadone is an opioid (mu) agonist.
D-methadone is an NMDA receptor antagonist.
This dual mechanism contributes to methadone's utility in chronic pain and may reduce opioid tolerance.
200
Which opioids are known to cause histamine release?
Bonus: Clinical importance aside from patient discomfort?
Morphine and meperidine (TL: Hydromorphone)
Itching, hypotension, and bronchospasm — relevant particularly in patients with reactive airway disease or hemodynamic instability
Histaminergic reaction is less common with Dilaudid.
Still a phenanthrene opioid (morphine-like structure) though.
The phenylpiperidines (fentanyl and friends) don't cause a histamine response.
300
In what specific intraoperative scenario is a bolus of alfentanil most useful?
For brief, intense periods of stimulation — e.g., local anesthetic injection by the surgeon during a MAC case, Mayfield head pins, or retrobulbar block.
Its ~90-second onset and brief duration make it ideal.
300
What is the typical sufentanil infusion dosing strategy, and when should it be turned off before the end of surgery?
Divide case into thirds: 0.3 → 0.2 → 0.1 mcg/kg/h. Turn off 15–30 minutes prior to end of surgery.
Note: dosing is mcg/kg/hour (not per minute like remifentanil)
300
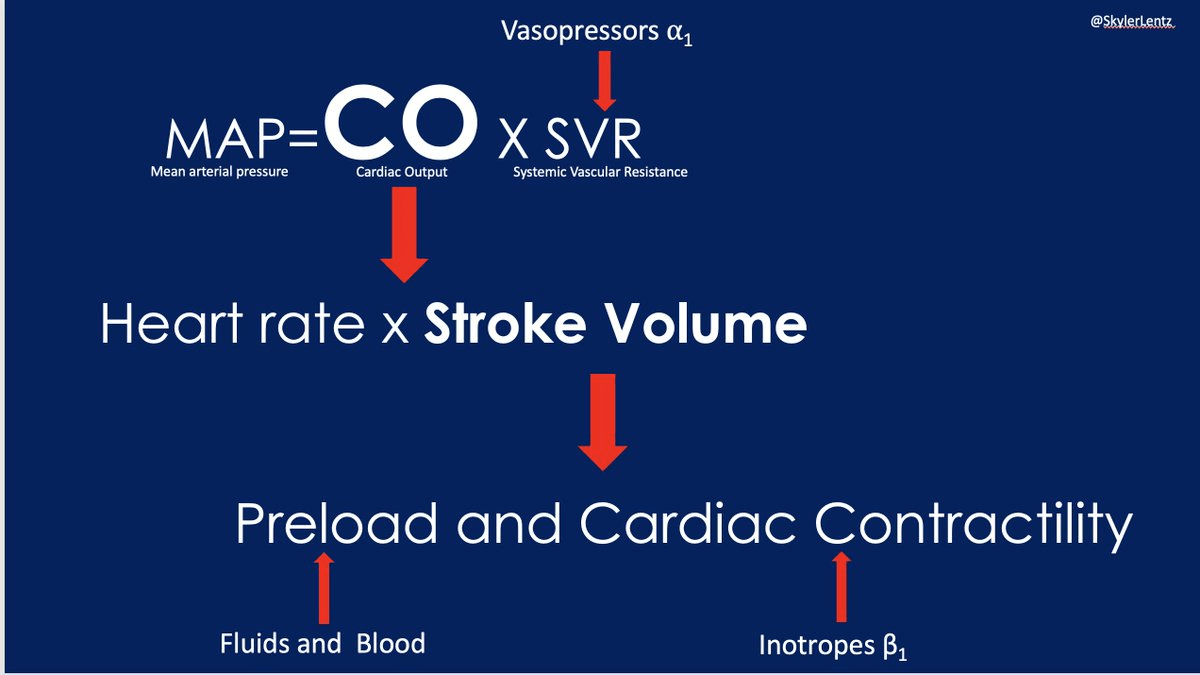
Opioids are considered hemodynamically stable when given alone. What hemodynamic changes (3) occur when they are combined with other anesthetics?
Decreased blood pressure, cardiac output, and stroke volume
300
A patient develops dysphoria and hallucinations after an opioid is administered. Which receptor subtype is most likely responsible?
The σ (sigma) receptor.
Agonists include pentazocine, nalorphine, and ketamine.
300
A patient on a prolonged high-dose remifentanil infusion (>0.15 mcg/kg/min) complains of severe pain postoperatively that does not respond well to additional opioids. What phenomenon explains this?
Bonus: What receptor is responsible for this phenomenon? What are prevention strategies?
Opioid-induced hyperalgesia (OIH). Prolonged high-dose remifentanil can cause central sensitization, resulting in paradoxical increased pain sensitivity that is less responsive to opioids and can persist days to weeks.
NMDA activation, not Mu opioid!
Prevention: Don't have the remi ripping at 0.3 mcg/kg/min, Incrementally downtitrating remi, NMDA antagonists (Ketamine, Mag, N2O).
400
Which reflex is inhibited by opioids? How can this be utilized to determine if the patient is snowed?
Pupillary light reflex. Opioid-induced miosis (pupillary constriction) serves as a clinical sign of opioid effect.
400
How should naloxone be dosed to reverse opioid-induced respiratory depression without precipitating acute pain or cardiovascular instability?
Dilute naloxone to 40 mcg/mL (10:1 dilution). Give 40–80 mcg IV increments (1–2 mL of diluted solution) and titrate until adequate ventilation is restored.
Avoid large bolus doses which can cause acute withdrawal, severe pain, and sympathetic surge.
400
What property of alfentanil allows it to cross the blood-brain barrier rapidly despite its high protein binding?
Alfentanil has a pKa of 6.5, which is close to physiologic pH.
This means a large fraction exists in the unionized (lipid-soluble) form at body pH, enabling rapid CNS penetration despite high protein binding.
400
Nalbuphine and butorphanol exert their analgesic effect primarily through which receptor subtype?
The κ (kappa) receptor, which mediates sedation and spinal analgesia.
Both are also partial mu antagonists.
400
______ is a metabolite of meperidine, and carries risk of causing ______ in patients with a history of ______
Normeperidine is a metabolite of meperidine, and carries risk of causing seizures in patients with a history of renal impairment
(due to renal excretion)
500
Name the active metabolite of morphine that is renaly excreted and has analgesic properties.
Clinical significance in patients with renal failure?
Morphine-6-glucuronide (M6G)
In renal failure, M6G accumulates and can cause prolonged respiratory depression and sedation
500
500
Morphine-6-glucuronide is a metabolte of morphine. Is it an active (analgesic) or inactive metabolite?
Does it's accumulation in patients with renal failure carry any risks?
Morphine-6-glucuronide (M6G) is an active metabolite with analgesic properties that is renally excreted.
In renal failure, M6G accumulates and can cause prolonged respiratory depression and sedation.
500
Codeine is a prodrug. What enzyme converts it to its active form, and what is the clinical implication for poor metabolizers?
Bonus: Do neonates have increased or decreased sensitivity to Codeine?
CYP2D6 converts codeine to morphine. Poor 2D6 metabolizers receive no analgesic benefit from codeine (or tramadol). This is why oxycodone is preferred over tramadol in known poor metabolizers.
Neonates have decreased CYP2D6 activity making them less sensitive to codeine than children. CYP2D6 levels begin to rise at 14d of age.
500
What tragic incident led to the creation of the Libby Zion Law? Explain the pharmacological mechanism and consequence.
What is the Libby Zion law?
Meperidine inhibits serotonin reuptake; combined with MAOIs it causes serotonin syndrome (agitation, hyperpyrexia, rigidity) or severe CNS/respiratory depression.
The Libby Zion Law (resident work hour restrictions) followed the death of an 18-year-old from this interaction.