IPV
Editorials
Photo Quizzz
Cochrane
ITE
100
A patient discloses IPV but says they are not ready to leave the relationship. Which of the following is the most appropriate response consistent with trauma- and violence-informed care?
A. “You need to leave right away. It’s unsafe for you to stay.”
B. “Why haven’t you told anyone sooner? You could have gotten help earlier.”
C. “I hear you. I'm here to support you whenever you’re ready to talk more or take the next step.”
D. “I will need to document this in the chart and notify social services immediately.”
Correct Answer: C. “I hear you. I'm here to support you whenever you’re ready to talk more or take the next step.”
Explanation:
A trauma-informed approach prioritizes safety, trust, collaboration, and patient autonomy. Patients may stay in relationships due to complex factors (finances, custody, safety concerns). Forcing action or expressing judgment is harmful and disempowering.
100
A 60-year-old woman without a uterus presents for a routine exam. She has no symptoms but read that hormone therapy may help prevent chronic conditions like osteoporosis and diabetes. She asks about starting estrogen therapy. What is the USPSTF's current recommendation regarding menopausal hormone therapy for primary prevention of chronic disease?
A. Recommend combined hormone therapy for all postmenopausal women without contraindications
B. Recommend estrogen-only therapy for primary prevention in women without a uterus
C. Discourage hormone therapy for chronic disease prevention regardless of formulation
D. Prescribe transdermal estrogen as it is safer than oral estrogen for prevention
E. Use MHT selectively in women under age 65 for cardiovascular protection
Correct Answer: C. Discourage hormone therapy for chronic disease prevention regardless of formulation
Explanation:
The USPSTF 2022 guidelines state:
Grade D recommendation: Recommends against using MHT (combined or estrogen-only) for primary prevention of chronic conditions (e.g., heart disease, osteoporosis, dementia) in postmenopausal women.
This is due to lack of net benefit and risk of serious harm.
Although estrogen may slightly reduce diabetes and fracture risk, the overall harm outweighs benefit.
The formulation or route (oral vs. transdermal) does not change the recommendation.
100
A 28‑year‑old woman presents with sharply demarcated, thick, scaling plaques on her knees and elbows. She reports occasional joint stiffness in her fingers in the morning. Which of the following diagnoses is most consistent?
A. Psoriasis Vulgaris
B. Eczematous Dermatitis
C. Lichen Planus
D. Tinea Corporis

Correct Answer: A. Psoriasis Vulgaris
Explanation:
Psoriasis vulgaris typically causes well demarcated, thick plaques with silvery scale on extensor surfaces (elbows, knees), often nail findings, possible psoriatic arthritis (joint stiffness).
Eczematous dermatitis is less sharply demarcated, more pruritic, often in flexural areas, with less thick scale.
Lichen Planus has violaceous, flat‑topped papules, often with Wickham striae, and mucosal involvement; scale is thinner, not thick, scaly plaques.
Tinea corporis (ringworm) has annular, scaly edges, central clearing; less likely thick scale over bilateral symmetric extensor surfaces with joint symptoms.
100
During a well-child visit, a family physician encounters a parent who is hesitant to vaccinate their child with the MMR vaccine. The parent has a college degree and cites concerns they read on social media. According to recent data, which of the following strategies is most appropriate to address their concerns?
A. Dismiss the parent from the practice to protect herd immunity
B. Emphasize that unvaccinated children are not accepted in most schools
C. Provide evidence-based resources and explore the parent’s specific concerns
D. Encourage the parent to wait until adolescence to decide about vaccination
Correct Answer: C. Provide evidence-based resources and explore the parent’s specific concerns
Explanation:
CDC guidelines recommend that clinicians listen actively to vaccine-hesitant parents and provide evidence-based information to help guide decision-making. The article notes that hesitancy is more common among educated parents who rely on social media, making empathetic, educational dialogue crucial. Dismissal (A) is not first-line and can backfire. Delaying vaccination (D) is contrary to public health guidance, and while school requirements (B) may be discussed, they’re not the best starting point in addressing parental concern.
100
A 30-year-old pregnant woman presents to the clinic for a health maintenance visit. When asked about tobacco use, she reports she has smoked a half a pack of cigarettes per day since she was a teenager and has continued to do so in pregnancy. Which of the following interventions is the best approach to address tobacco use in this patient?
A Electronic cigarettes
B Health education and counseling
C Nicotine replacement patches
D Varenicline
Correct Answer ( B )
Explanation:
The United States Preventive Services Task Force (USPSTF) strongly recommends screening for tobacco misuse in all adult patients, including those who are pregnant. Patients who smoke should be advised to quit. Physicians can assist smoking cessation through behavioral intervention and, in nonpregnant patients, through the use of FDA-approved pharmacotherapy. There is insufficient evidence to support the use of FDA-approved pharmacotherapy during pregnancy, as it remains unclear whether the benefits of pharmacologic treatment outweigh its potential harms. Therefore, smoking cessation interventions should encompass those that help to change behaviors, including health education and counseling.
The American College of Obstetricians and Gynecologists (ACOG) recommends that health education include specific information on the harmful effects of smoking for mother and baby. For instance, pregnant patients may be advised of the strong links between smoking and fetal abnormalities (e.g., intrauterine growth restriction and cleft lip or palate). Research shows health education without counseling is not an effective strategy. Therefore, a counseling program should be implemented. The USPSTF identified successful programs as those that tend to be more intensive and tailored to the individual.
200
A 34-year-old transgender woman comes to your clinic for routine care. You want to assess for IPV in a sensitive, evidence-based manner. Which screening tool is best validated and most appropriate for use in this situation?
A. Partner Violence Screen
B. Extended-HITS
C. Women Abuse Screening Tool (WAST)
D. Danger Assessment-5
Correct Answer: B. Extended-HITS
Explanation:
The Extended-HITS is validated, concise, and includes questions about physical, emotional, and sexual IPV, making it suitable for diverse populations including transgender individuals, who have 2–3x higher risk for IPV than cisgender individuals. The Danger Assessment-5 is useful when risk of homicide is suspected but is not a primary screening tool. WAST lacks clear cutoffs and is less standardized.
200
A 17-year-old male with no history of substance use presents with a tibial fracture after a sports injury. He is discharged from urgent care with a 3-day opioid prescription. According to AAP guidelines, what is the best next step?
A. Counsel the patient on safe storage, but do not coprescribe naloxone unless there is a substance use history
B. Coprescribe naloxone, as it is recommended universally when opioids are prescribed to adolescents
C. Extend the opioid prescription to 5–7 days to prevent return visits
D. Recommend OTC naloxone purchase only if parents express concern about overdose
E. Avoid opioids entirely and manage with NSAIDs alone, even if inadequate for pain control
Correct Answer: B. Coprescribe naloxone, as it is recommended universally when opioids are prescribed to adolescents
Explanation:
The AAP guideline recommends universal naloxone coprescribing when opioids are prescribed to adolescents, even in the absence of substance use history. This is because:
Adolescent overdose deaths are rising, driven in part by illicit fentanyl
Naloxone is safe, effective, and increasingly easy to prescribe
Proactively prescribing naloxone may reduce mortality even when prescription opioids are not the direct cause of overdose
A is incorrect: No risk factors are needed for naloxone coprescription—it is universal.
C is incorrect: A longer course is not recommended for most acute pain situations.
D is incorrect: OTC purchase is helpful, but coprescription is stronger guidance.
E is incorrect: Avoiding opioids entirely may lead to undertreatment of pain, which the guideline cautions against.
200
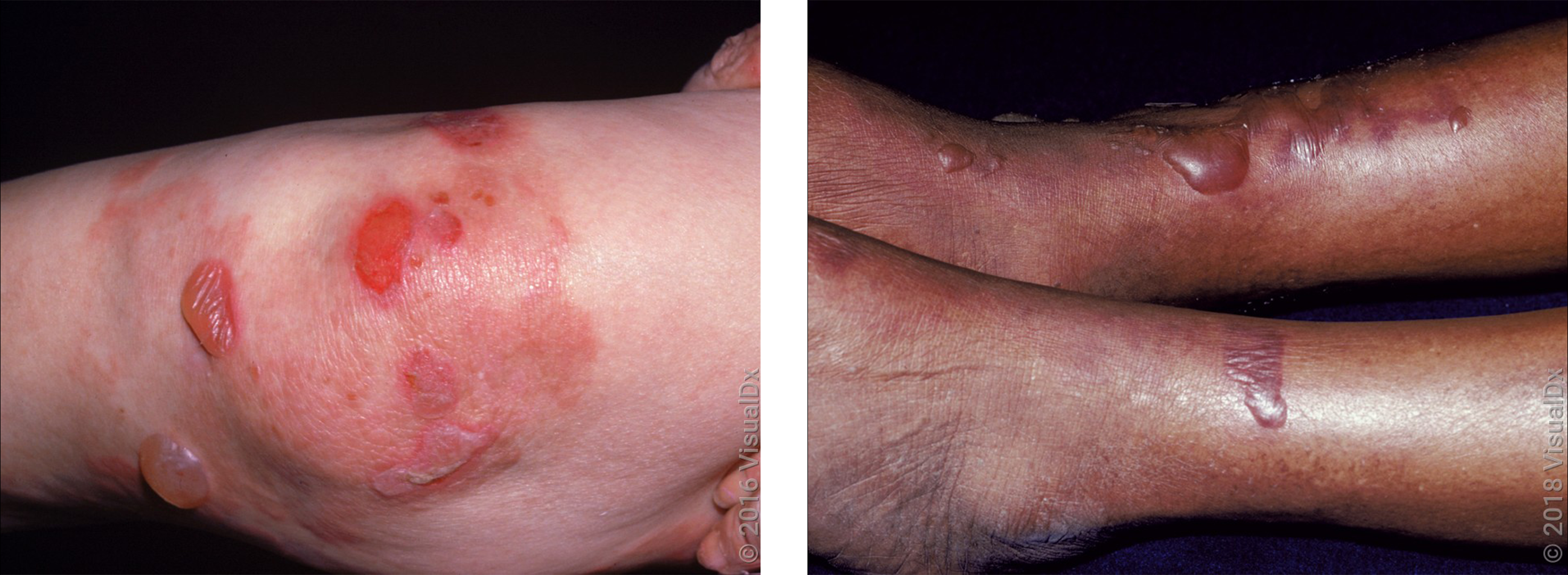
A 35‑year‑old man develops intensely pruritic clustered papules and vesicles on his elbows and knees. Biopsy shows subepidermal blisters, and direct immunofluorescence reveals granular IgA deposits in the dermal papillae. Which is the most likely diagnosis?
A. Bullous Pemphigoid
B. Linear IgA Dermatosis
C. Dermatitis Herpetiformis
D. Pemphigus Vulgaris
Correct Answer: C. Dermatitis Herpetiformis
Explanation:
Dermatitis herpetiformis presents as intensely pruritic grouped vesicles/papules, often on extensor areas (elbows/knees), with granular IgA deposition in dermal papillae (on immunofluorescence).
Linear IgA Dermatosis also has IgA deposition, but often linear along basement membrane zone rather than granular in papillae.
Bullous Pemphigoid usually in older adults, with large tense blisters, not grouped pruritic papulovesicles, and immunofluorescence shows linear IgG/C3 at basement membrane.
Pemphigus Vulgaris shows flaccid intraepidermal bullae and positive Nikolsky’s sign, often involves mucous membranes.
200
A 4-year-old child is scheduled to receive their second dose of the MMR and varicella vaccines. The parent expresses doubt about the effectiveness of the vaccines. Based on the best available evidence, what is the most appropriate information to share regarding the vaccine’s effectiveness?
A. Two doses of MMR and varicella vaccines offer minimal protection against the diseases
B. Two doses of varicella vaccine reduce the risk of severe varicella by 50%
C. Two doses of MMR and varicella vaccines significantly reduce the risk of measles, mumps, rubella, and varicella
D. A single dose of MMR and varicella vaccine is more effective than two doses
Correct Answer: C. Two doses of MMR and varicella vaccines significantly reduce the risk of measles, mumps, rubella, and varicella
Explanation:
Multiple studies show that two doses of the MMR and varicella vaccines are highly effective:
Measles: RR = 0.04
Mumps: RR = 0.12
Rubella: RR = 0.11
Varicella: Rate ratio = 0.05 (over 10 years)
These numbers represent significant reductions in disease risk, based on moderate- to high-certainty evidence. Option A underestimates effectiveness, and Option D is incorrect. Option B misrepresents the data, the reduction in varicella of any severity was 95%, not just severe cases.
200
A 66-year-old female with a past medical history of well-controlled type 2 diabetes diagnosed at age 60 presents for a health maintenance examination. She was previously vaccinated with 23-valent pneumococcal polysaccharide vaccine (PPSV23, Pneumovax 23) at the time of her diabetes diagnosis.
Based on CDC guidelines, which one of the following should you recommend to her today to complete her pneumococcal vaccination series? (check one)
A. No additional pneumococcal vaccine
B. A repeat dose of PPSV23
C. 13-valent pneumococcal conjugate vaccine (PCV13, Prevnar 13)
D.15-valent pneumococcal conjugate vaccine (PCV15, Vaxneuvance)
E.20-valent pneumococcal conjugate vaccine (PCV20, Prevnar 20)
Correct Answer E
In patients who were previously vaccinated with 23-valent pneumococcal polysaccharide vaccine between the ages of 19 and 64 due to risk factors such as type 2 diabetes, the CDC now recommends one dose of 20-valent pneumococcal conjugate vaccine.
300
Which of the following interventions has been shown to have the most consistent positive impact on safety and quality of life for patients experiencing IPV?
A. Routine use of HARK screening in all adults
B. Individual psychotherapy focusing on self-esteem improvement
C. Multidisciplinary advocacy including safety planning and warm handoffs
D. Mandated reporting of all IPV cases to law enforcement
Correct Answer: C. Multidisciplinary advocacy including safety planning and warm handoffs
Explanation:
The most effective IPV interventions involve multidisciplinary care, including behavioral health, advocacy, social work, and warm handoffs. These programs focus on patient autonomy, safety planning, and resource provision. Psychotherapy may help with depression/anxiety, but advocacy-focused care improves safety and quality of life outcomes.
300
A 9-year-old girl presents with moderate pain after a dental extraction. The clinician considers prescribing an opioid for short-term use. Which of the following statements best reflects current guidelines regarding opioid selection for this patient?
A. Tramadol is preferred over codeine due to its partial agonist effects and lower addiction potential
B. Codeine is safe in children older than 6 years if the dose is adjusted based on weight
C. Tramadol and codeine should be avoided in children under 12 years due to the risk of respiratory depression
D. Tramadol is appropriate for children with obstructive sleep apnea as long as naloxone is coprescribed
E. Codeine is contraindicated only in postoperative pain related to orthopedic procedures
Correct Answer: C. Tramadol and codeine should be avoided in children under 12 years due to the risk of respiratory depression
Explanation:
The FDA has issued strong contraindications (its highest level warning) against the use of codeine and tramadol in:
Children under 12 years
Children under 18 years after tonsillectomy or adenoidectomy
Adolescents 12–18 years with obesity, OSA, or severe lung disease
These drugs are metabolized variably (especially codeine, which is a prodrug converted to morphine), and ultra-rapid metabolizers are at increased risk of respiratory depression and death.
A is incorrect: Tramadol is not safer; it's also contraindicated in this age group.
B is incorrect: Codeine is never considered safe in children under 12, regardless of weight.
D is incorrect: Tramadol is specifically contraindicated in patients with OSA.
E is incorrect: The codeine ban applies to tonsillectomy/adenoidectomy, not just orthopedic surgeries.
300
A 12‑year‑old girl presents with a 4‑week history of progressive muscle weakness and this rash over her eyelids and upper arms. She also reports difficulty rising from a chair and climbing stairs. Which of the following is the most likely diagnosis?
A. Systemic Lupus Erythematosus (SLE)
B. Dermatomyositis
C. Polymyalgia Rheumatica
D. Seborrheic Dermatitis

Correct Answer: B. Dermatomyositis
Explanation:
Dermatomyositis is characterized by proximal muscle weakness plus characteristic skin findings such as a heliotrope rash (violaceous discoloration of the eyelids), shawl/back/upper arms erythema, Gottron papules. The image suggests violaceous rash and distribution consistent with this.
SLE can cause rash, but not usually muscle weakness of this pattern, nor the heliotrope eyelid finding.
Polymyalgia Rheumatica causes proximal muscle pain/stiffness but no rash.
Seborrheic Dermatitis causes erythema and flaking in seborrheic distribution (scalp, nasolabial folds), not muscle weakness.
300
The parent of a 12-month-old child expresses concern about the safety of the MMR vaccine, particularly regarding the risk of autism. Which of the following statements is most accurate based on current evidence?
A. Although a few observational studies suggest a link between MMR vaccination and autism, large-scale reviews have found a modest increase in risk.
B. The MMR vaccine has been associated with a transient increase in febrile seizures, but there is no credible evidence linking it to autism spectrum disorder.
C. While the MMR vaccine may increase the risk of autoimmune conditions like inflammatory bowel disease, no significant neurologic risks have been found.
D. Adverse effects such as idiopathic thrombocytopenic purpura and developmental delays, including autism, have been associated with MMR vaccination in cohort studies.
Correct Answer: B. The MMR vaccine has been associated with a transient increase in febrile seizures, but there is no credible evidence linking it to autism spectrum disorder.
Explanation:
Option B is the most accurate summary of current evidence:
The MMR vaccine does slightly increase the risk of febrile seizures within about a week of vaccination (rate ratio = 2.45), but this remains a rare and self-limited event.
Multiple high-quality studies, including Cochrane reviews and CDC data, show no association between MMR vaccination and autism spectrum disorder (ASD).
The vaccine is not associated with inflammatory bowel disease (IBD) or long-term neurologic harm
300
A 65-year-old woman presents to the clinic with her adult child with concerns of considerable mental decline in the past 6 months. She has been unable to complete previously familiar tasks without the use of a list, and she has been having difficulty recalling recent events. Her child also notes changes in the patient’s gait that resulted in a recent fall. In addition, she has reported increased symptoms of urinary urgency and two episodes of urinary incontinence. In addition to a history and physical examination, the clinician performs a brief cognitive test. The patient is able to initially repeat three words and draw a clock but later can only recall one word. Which of the following is the best next study to order in the evaluation of this patient?
A.Cerebrospinal fluid analysis
B.Genetic testing for the apolipoprotein E4 allele
C.Noncontrast head CT
D.Thyroid-stimulating hormone level
Correct Answer ( D )
Explanation:
Cognitive decline is a prevalent concern in older patients and is often reported by a patient’s family member. This patient appears to have a constellation of cognitive, urinary, and motor concerns, which may be suggestive of a neurologic process. In this case, the patient presentation alludes to the triad of normal pressure hydrocephalus (NPH), which includes dementia, urinary incontinence, and gait disturbance.
Dementia can present with memory loss, loss of executive function, and psychomotor slowing, and it has a multitude of causes. Clinical examination should include a brief cognitive test, such as the Mini-Cog, which can be administered in a few minutes. Diagnostic studies should start with a standard dementia workup to rule out differential causes of dementia. This panel should include a complete blood count and complete metabolic profile and vitamin B12, folate, and thyroid-stimulating hormone levels. Testing for HIV and syphilis may be included if these infections are suspected.
400
A 28-year-old woman presents to your office for a routine wellness exam. She appears anxious and avoids eye contact. You suspect possible intimate partner violence (IPV). You are practicing in a state where reporting IPV is not mandatory unless there is a weapon involved or the patient is a minor. What is the most appropriate next step in management?
A. Screen for IPV using a validated tool like HARK or HITS, and if positive, contact local law enforcement immediately
B. Begin universal education about healthy and unhealthy relationships using nonjudgmental language, regardless of disclosure
C. Ask the patient directly if her partner has ever hit her, and document any signs of abuse in the EHR regardless of her response
D. Postpone addressing IPV until a future visit when more time is available and rapport is stronger
E. Distribute a printed IPV resource brochure only if the patient confirms abuse
Correct Answer: B. Begin universal education about healthy and unhealthy relationships using nonjudgmental language, regardless of disclosure
Explanation:
Answer A is incorrect: Although screening is important, mandatory reporting to law enforcement is not indicated unless your state law requires it (e.g., if a weapon is used, if the patient is a minor, or there's threat to a child). Immediate contact with law enforcement without patient consent can erode trust and potentially endanger the patient.
Answer B is correct: Universal education is a key approach recommended for all patients, regardless of disclosure. It normalizes conversations about IPV, provides resources without requiring disclosure, and can be done quickly and compassionately, even in a busy clinic. It supports autonomy, privacy, and patient empowerment.
Answer C is incorrect: Directly asking only about physical abuse misses the broader spectrum of IPV (emotional, psychological, sexual, etc.). Also, documenting sensitive suspicions without patient consent may increase risk if the EHR is accessed by the partner.
Answer D is incorrect: While rapport is important, delaying IPV intervention ignores the urgency of the issue. Brief, trauma-informed universal education can be done in any visit and does not require disclosure.
Answer E is incorrect: Providing resources only after disclosure undermines the preventive and educational role of universal education. Every patient should be offered IPV resources regardless of their situation.
400
A 16-year-old female with Ehlers-Danlos syndrome (EDS) is admitted for acute abdominal pain following a fall. She has been on stable long-term opioid therapy for chronic musculoskeletal pain. A new clinician considers tapering her baseline opioids to prevent overuse. What is the most appropriate next step in management?
A. Discontinue baseline opioids and begin short-acting opioids for acute pain only
B. Taper baseline opioids by 25% and add adjunctive therapy for pain
C. Continue baseline opioids and provide additional short-term opioids as needed for acute pain
D. Refer to addiction medicine before managing pain further
E. Switch to NSAIDs and acetaminophen only, as chronic opioid use increases risk of misuse
Correct Answer: C. Continue baseline opioids and provide additional short-term opioids as needed for acute pain
Explanation:
The guideline emphasizes that young people on long-term opioid therapy for chronic pain (e.g., from EDS or sickle cell disease):
Should not have their baseline opioids abruptly stopped or tapered during episodes of acute pain
Require additional analgesia during acute exacerbations, on top of their baseline regimen
May experience untreated pain, withdrawal, or illicit opioid use if therapy is withheld or modified inappropriately
A, B, E are incorrect: Tapering or stopping opioids during acute pain can worsen outcomes
D is incorrect: Referral to addiction medicine is not appropriate unless there's evidence of opioid use disorder (OUD)
Clinicians should also be able to differentiate between functional chronic opioid use and OUD, which is defined by loss of control, negative consequences, and declining function.
400

A 5‑year‑old child with 3‑day history of fever, sore throat, and now a diffuse maculopapular rash covering the trunk. The child is vaccinated for measles and rubella. What is the most likely cause?
A. Measles
B. Scarlet fever
C. Roseola (exanthem subitum)
D. Viral exanthem (non‑specific)
Correct Answer: D. Viral exanthem (non‑specific)
Explanation:
Given vaccination status for measles and rubella, those are less likely (though possible in rare vaccine failure). Measles often has Koplik spots, a prodrome, and associated cough/coryza/conjunctivitis.
Scarlet fever has a more characteristic sand‑paper rash, strawberry tongue, and often starts on neck/chest.
Roseola often has high fever for several days followed by abrupt defervescence and rash; rash typically appears as fever subsides.
A non‑specific viral exanthem is common, especially in children, with fever and rash; many viruses cause maculopapular rash that resolves with supportive care.
400
A 32-year-old patient with moderate atopic dermatitis asks about starting topical therapy. You are considering prescribing either a corticosteroid or a calcineurin inhibitor. Which of the following statements is most accurate regarding the relative efficacy and safety of these options?
A. Tacrolimus 0.03% and potent topical corticosteroids are equally effective and have similar risk profiles for skin thinning
B. Tacrolimus 0.1% is among the most effective options, but it carries a higher risk of application site reactions compared to corticosteroids
C. Ruxolitinib is less effective than tacrolimus 0.1%, but it causes fewer application site reactions
D. Crisaborole 2% has high efficacy but may cause significant skin thinning with long-term use
Correct Answer: B. Tacrolimus 0.1% is among the most effective options, but it carries a higher risk of application site reactions compared to corticosteroids
Explanation:
Tacrolimus 0.1% demonstrated high efficacy (OR = 6.27 for patient-reported symptoms) and is one of the most effective topical therapies for eczema.
However, it has increased risk of application site reactions such as burning or stinging (OR = 2.2), while topical corticosteroids have a lower incidence of such reactions.
Option A is incorrect: While tacrolimus 0.03% is effective, it is not equally potent as very potent corticosteroids, and they do not have identical safety profiles.
Option C is incorrect: Ruxolitinib 1.5% is similarly effective (OR = 5.64), but the article does not provide comparative safety data favoring ruxolitinib over tacrolimus for site reactions.
Option D is incorrect: Crisaborole is among the least effective agents and is not associated with skin thinning. It does cause application site reactions but has no corticosteroid-like atrophy risk.
400
Which one of the following tests should you obtain in a patient with lichen planus?
A. Antihistone antibodies
B. Hepatitis C antibody
C. HIV antibody
D.Sjögren syndrome–related antigen A (Ro) and Sjögren syndrome–related antigen B (La) antibodies
Correct Answer B
Lichen planus is a disorder of unknown etiology affecting the skin, genitals, oral cavity, scalp, nails, and esophagus. Patients with lichen planus have a higher (up to sixfold) incidence of hepatitis C virus infection. Hence, screening for hepatitis C should be performed in patients with lichen planus even though the cause-and-effect relationship between hepatitis C and lichen planus is unknown.§Antihistone antibodies are present in patients with medication-induced lupus erythematosus. HIV antibody is used in screening for HIV infection. Sjögren syndrome–related antigen A (Ro) and Sjögren syndrome–related antigen B (La) antibodies are present in patients with Sjögren syndrome.
500
A 7-year-old child is brought in for evaluation after the mother disclosed IPV during a visit. There is no evidence of direct harm to the child. Which of the following is most accurate regarding your legal obligations?
A. Report the child’s exposure as child maltreatment in all 50 states
B. Report exposure only if physical harm to the child is evident
C. Report exposure as child maltreatment if practicing in Utah or Georgia
D. No reporting is required since the child was not physically harmed
Correct Answer: C. Report exposure as child maltreatment if practicing in Utah or Georgia
Explanation:
Only Utah and Georgia have laws that automatically define child exposure to IPV as child maltreatment, even without direct harm. In most states, reporting is required only if the child is harmed or threatened. Clinicians must be familiar with state-specific laws.
500
A 62-year-old woman with an intact uterus is interested in starting hormone therapy for mild hot flashes. She asks you about the risks found in the Women’s Health Initiative (WHI) trial. Which of the following outcomes was increased in women receiving combined estrogen-progestin therapy in the WHI?
A. Decreased risk of breast cancer and ovarian cancer
B. Increased risk of endometrial cancer and stroke
C. Increased risk of pulmonary embolism and breast cancer
D. Decreased risk of dementia in women over 65
E. No difference in gallbladder disease risk
Correct Answer: C. Increased risk of pulmonary embolism and breast cancer
Explanation:
In the WHI combined therapy arm (estrogen + medroxyprogesterone), significant increases were seen in:
Breast cancer
Pulmonary embolism
Stroke
Dementia (in women ≥65)
Gallbladder disease
Overall global index of harm
There was no increase in endometrial cancer, as progestin was added to protect the endometrium.
In contrast, estrogen-only therapy increased stroke and ovarian cancer, not breast cancer.
500
A 40-year-old man from a leprosy-endemic region presents with two pale, well-defined patches on his cheek. He notes that these patches have been present for months and occasionally feel less sensitive to touch and temperature. No itching or scaling is noted. There is no history of trauma, inflammation, or prior topical treatments.
Which of the following is the most likely diagnosis?
A. Indeterminate leprosy
B. Early vitiligo
C. Hypopigmented tinea corporis
D. Postinflammatory hypopigmentation from subclinical eczema
E. Tuberculoid leprosy

E. Tuberculoid leprosy
Few, well-demarcated hypopigmented or erythematous lesions, often on face or extremities.
Significant clue is sensory loss, which is classic.
Endemic setting and lesion chronicity strongly support this.
Tip for Exam:
Sensory loss is the hallmark clinical clue that strongly favors leprosy over other hypopigmented conditions. In a leprosy-endemic area, one or more anesthetic skin patches should immediately raise concern for tuberculoid or borderline leprosy.
500
A 45-year-old man with chronic atopic dermatitis controlled on topical tacrolimus 0.1% expresses concern about long-term side effects and cost. He asks whether switching to a topical corticosteroid is reasonable. Based on current evidence, what is the best response?
A. Switching to corticosteroids may reduce adverse effects, but long-term use increases the risk of skin thinning even with low-potency formulations
B. Tacrolimus has a lower risk of skin thinning than corticosteroids but is less effective in symptom control and is more expensive
C. Topical corticosteroids are less effective than tacrolimus but are preferred due to their favorable cost and safety profile
D. Corticosteroids are comparably effective, more affordable, and have a lower rate of local side effects in short-term use compared to tacrolimus
Correct Answer: D. Corticosteroids are comparably effective, more affordable, and have a lower rate of local side effects in short-term use compared to tacrolimus
Explanation:
Corticosteroids (especially potent and very potent ones like clobetasol) are highly effective, with effectiveness comparable to tacrolimus 0.1%.
Short-term use (up to 3 weeks) of corticosteroids does not increase the risk of skin thinning, and local side effects like burning/stinging are less common than with tacrolimus.
Cost is another important factor: clobetasol is substantially cheaper than tacrolimus and especially than ruxolitinib.
Option A is misleading: While long-term corticosteroid use can increase risk of skin thinning, short-term use is safe, and the question implies that short-term use is the context.
Option B is incorrect: Tacrolimus is not more effective; it’s similarly effective but more costly and more irritating on application.
Option C is incorrect: Corticosteroids are not less effective than tacrolimus and may be preferred due to lower cost and side effect profile in short-term use.
500
A 35-year-old woman is brought to the emergency department for evaluation of a shoulder injury after a fall from her bicycle. She reports no loss of consciousness or pain in her back, neck, or head. Vital signs are normal. Physical examination shows an abrasion on the top of the left shoulder, guarding of the shoulder, and tenderness to palpation with limited range of motion. There is no visible deformity. Distal neurovascularity is intact. Which of the following assesses for acromioclavicular joint injury or separation?
A Dimple inferior to the acromion laterally
B Holding the affected arm in the contralateral hand
C Inability to hold the affected arm in an elevated position
D Palpable humeral head in the axilla
E Tenderness with cross-body adduction test
Correct Answer ( E )
Explanation:
The ligaments that stabilize the acromioclavicular joint are the coracoclavicular ligaments, which provide stability in the superior and inferior directions, and the acromioclavicular ligaments, which provide stability in the anterior and posterior directions. The usual mechanism of injury is a fall onto a shoulder with the arm across the body, which often causes the acromion to displace medially and inferiorly relative to the clavicle. Injury to the joint causes pain with overhead motion and arm adduction, but symptoms may not correlate with X-ray findings. Palpation may reveal tenderness of the joint. Provocative testing includes the examiner pulling the affected arm (and thus the acromion) in a downward motion and observing for a rise of the distal clavicle, indenting the skin, in cases of acromioclavicular separation. The cross-body adduction test involves bringing the affected arm across the body to squeeze the acromion and clavicle together, causing pain if arthritis or separation is present.
The Zanca view radiograph best visualizes the acromioclavicular joint