Community-Acquired Pneumonia
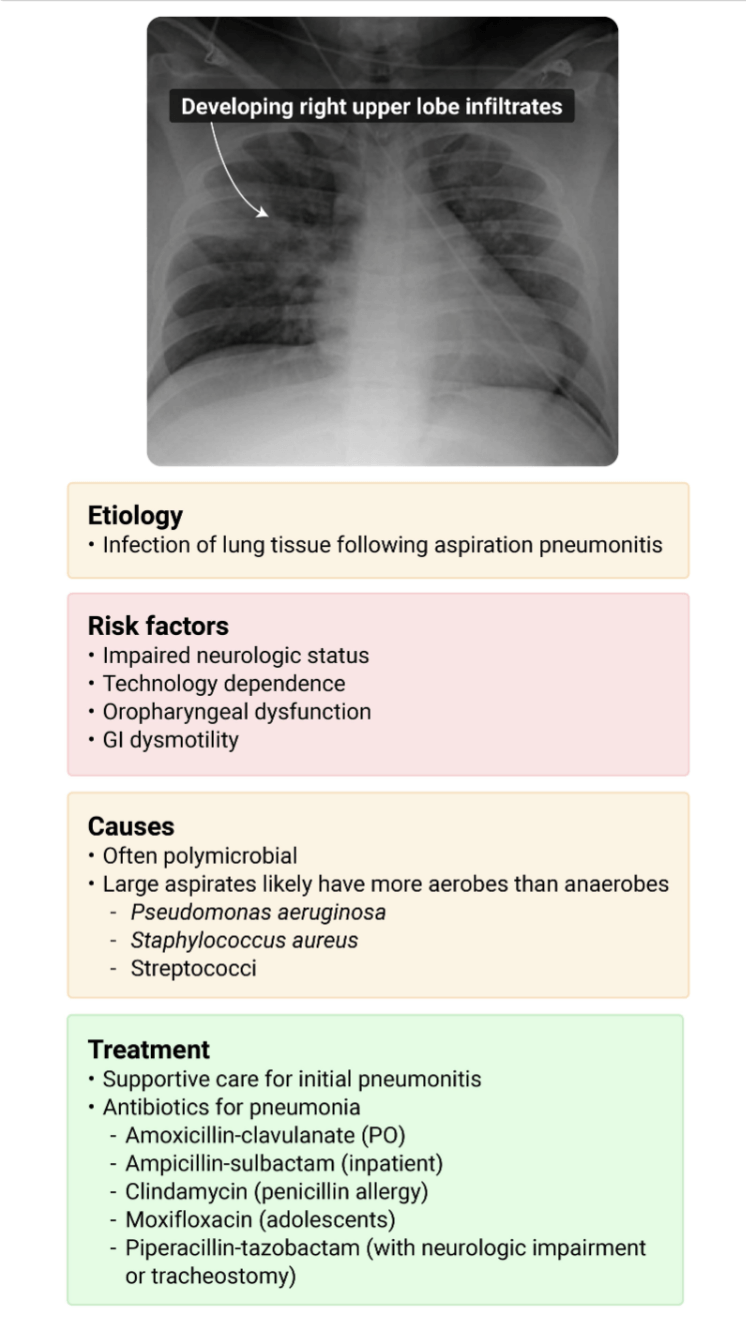
Aspiration Pneumonia
Non-Infectious Pulmonary Infiltrates
Lung Empyema & Abscess
Tuberculosis
100
What is the Organism?
Pneumonia in patient with fever, chills, malaise, dry cough, abdominal pain, diarrhea, nausea, vomiting
CXR: Multiple patchy non-segmented infiltrates and pleural effusion
Legionella pneumophila
Legionella species can cause a range of illnesses from benign self-limited disease to multisystem organ failure with ARDS.
Patients at higher risk include cigarette smokers, patients with chronic lung disease, transplant patients, and the immunosuppressed.
Commonly complicated by GI symptoms.
In addition, Legionella can affect other organ systems, causing sinusitis, pancreatitis, myocarditis, and pyelonephritis.
The chest radiograph frequently shows a patchy infiltrate, with the occasional appearance of hilar adenopathy and pleural effusions.
Urinary Legionella antigen testing in patients is no longer recommended; the tests have poor sensitivity and may lead to underdiagnosis.
Treatment for Legionella is based on clinical suspicion.
100
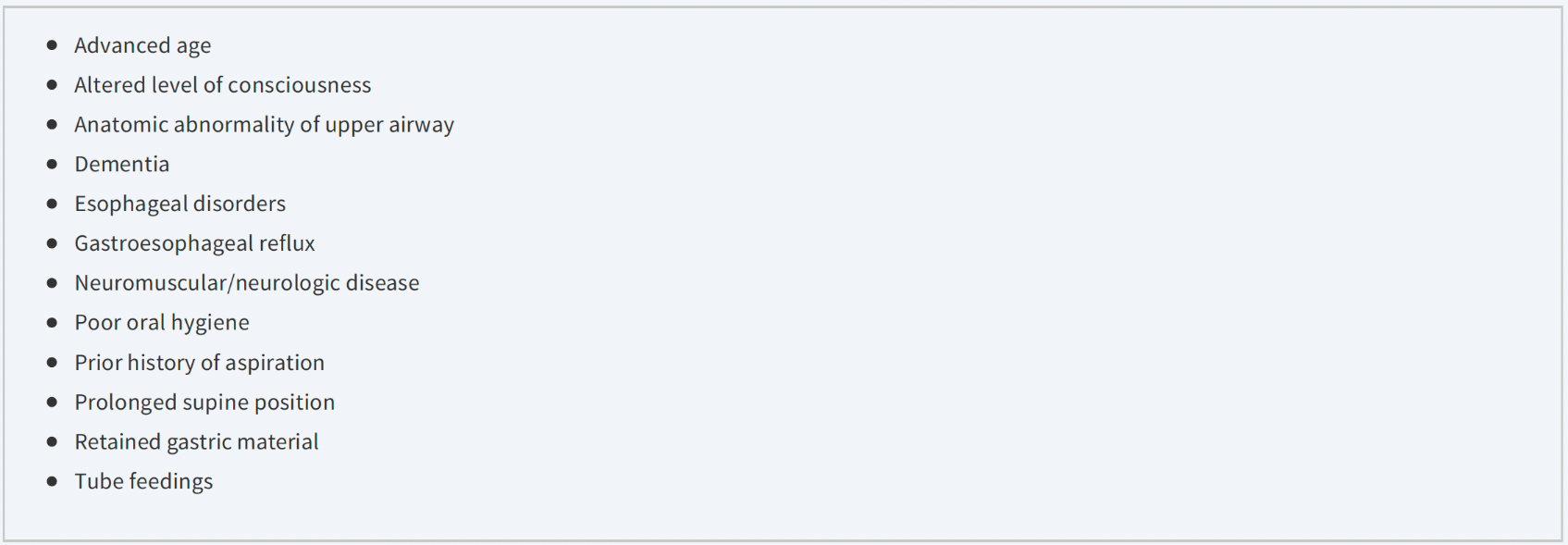
Risk Factors
Name 3 risk factors for Aspiration Pneumonia
100
Differential Diagnosis
What are 3 common causes of non-infectious pulmonary infiltrates?
Congestive heart failure, aspiration pneumonitis, and pulmonary embolism.
Others: Allergic bronchopulmonary Aspergillosis, Acute eosinophilic lung disease, Hypersensitivity pneumonitis (extrinsic allergic alveolitis), Organizing pneumonia (bronchiolitis obliterans organizing pneumonia [BOOP]), Acute interstitial pneumonia, Sarcoidosis, Anti–glomerular basement membrane antibody disease (Goodpasture's syndrome), Drug-induced pneumonitis, Chemical pneumonitis, Radiation pneumonitis, Acute respiratory distress syndrome, Alveolar hemorrhage, Fat emboli
100
What is the Treatment?
The definitive treatment of an empyema is?
Drainage and Antibiotics
In addition, treat any underlying disease, especially pneumonia. NSAIDs or opioids can decrease pleuritic pain. Thoracentesis and drainage aid in the diagnosis and provide symptomatic relief for dyspnea.
100
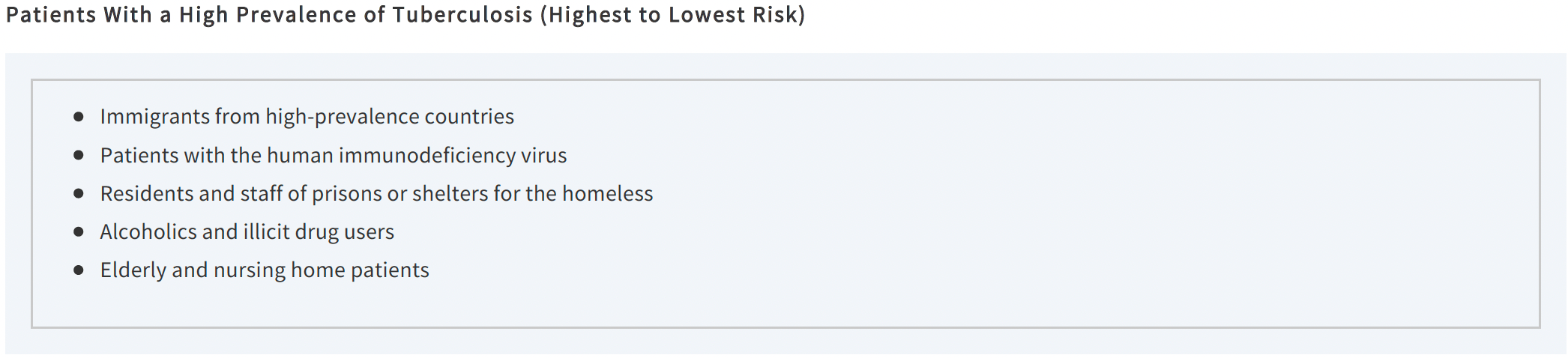
Patient Populations
Name 3 of the 5 patient populations with a high prevalence of Tuberculosis
200
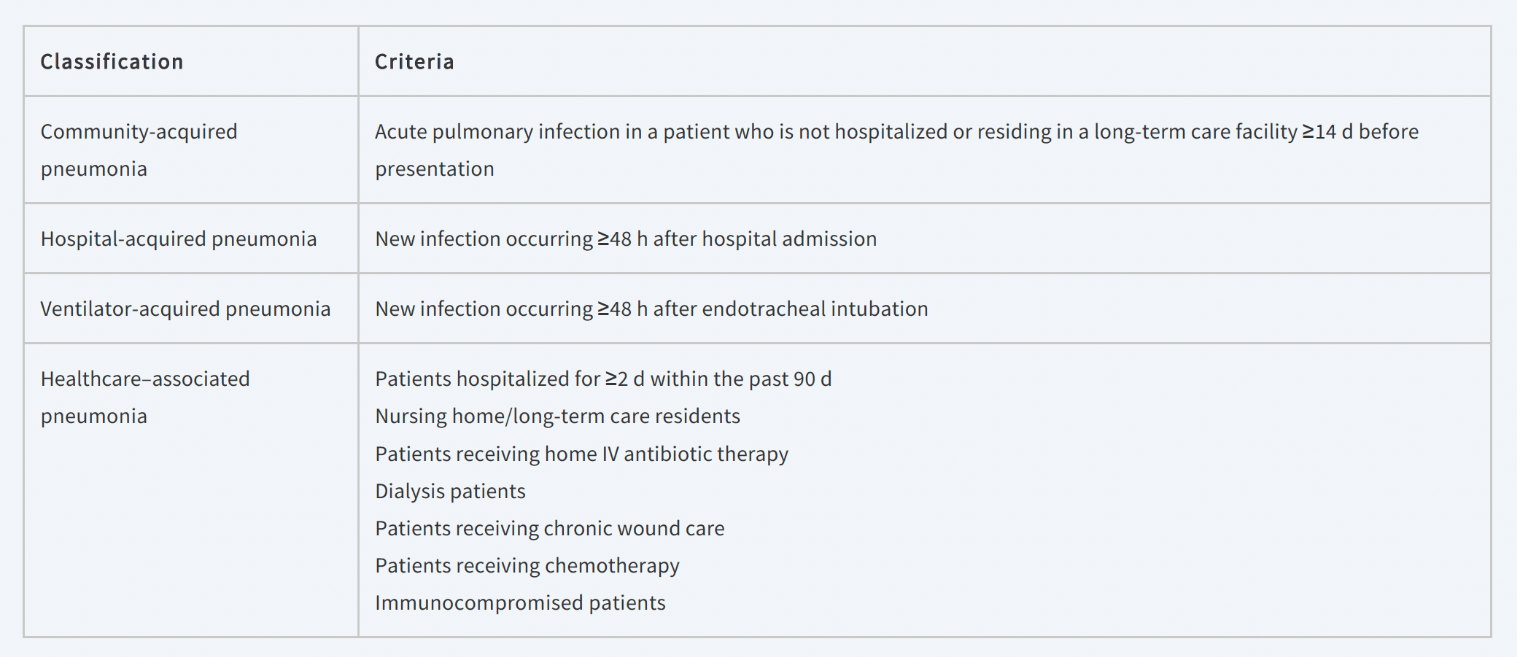
Patients with healthcare-associated pneumonia are at risk for infection with which type of organisms?
Patients with healthcare-associated pneumonia are at risk for infection with Atypical and Resistant organisms.
- Legionella
- Chlamydia
- Mycoplasma
- Methicillin Resistant S. aureus
200
Aspiration pneumonia is the 2nd leading cause of infection in nursing homes, after what other type of infection?
Urinary Tract Infections
It is the leading cause for transfer from nursing home to the hospital and the leading cause of death in nursing home patients.
200
Name the Disease
What is a non-infectious cause of pulmonary infiltrates commonly seen in patients with asthma or cystic fibrosis?
Allergic Bronchopulmonary Aspergillosis
Symptoms: Dyspnea, wheezing, productive cough; may have hemoptysis and occasionally fever.
Chest Radiography Findings: Branching tubular opacities may be seen, usually predominantly or exclusively involving the upper lobes.
Pathophys: Eosinophils filling small airways and alveolar spaces due to inflammation. Bronchiectasis.
200
What is the Treatment?
Which fibrinolytics can be used to improve drainage of loculated parapneumonic effusions and empyemas?
Urokinase, Alteplase, or Streptokinase
A blinded randomized trial comparing double placebo, alteplase and DNase, alteplase and placebo, or DNAase and placebo found that DNase alone or alteplase alone was ineffective, but the combination of alteplase and DNase improved fluid drainage, decreased the frequency of surgical referral, and decreased the length of hospital stay.
200
Percentage
What percent of patients become infected with Tuberculosis after exposure?
Only 30% of patients become infected after a droplet exposure.
Mycobacterium tuberculosis is a slow-growing aerobic rod that settles in areas of high oxygen content and blood flow. Transmission occurs via aerosolization of bacteria and inhalation of droplet nuclei into the lungs. Persons with active tuberculosis who excrete mycobacteria in saliva or sputum are the most infectious.
300
What is the difference between hospital-acquired pneumonia and healthcare-associated pneumonia?
(How do you define each?)
300
What is the Treatment?
Name 3 reasonable antibiotics for suspected community-acquired aspiration pneumonia
Clindamycin, a Carbapenem, Ampicillin-sulbactam (Unasyn), and Moxifloxacin are all reasonable treatments for suspected community-acquired aspiration pneumonia.
300
Name the Disease
Idiopathic or Secondary to chemical agents
Acute Interstitial Pneumonia
Symptoms: Rapid progression to respiratory failure. Mortality rate higher in those with comorbidities.
Chest Radiography Findings:
Normal for first 12–24 h. Bilateral opacities with sparing of costophrenic angles. Minimal or no pleural effusion. “White lung” due to extensive consolidation.
3 Stages:
1) Interstitial edema spreads to alveoli (Exudative)
2) Organization of fibrinous exudate (Proliferative)
3) Honey comb fibrosis (Fibrotic)
300
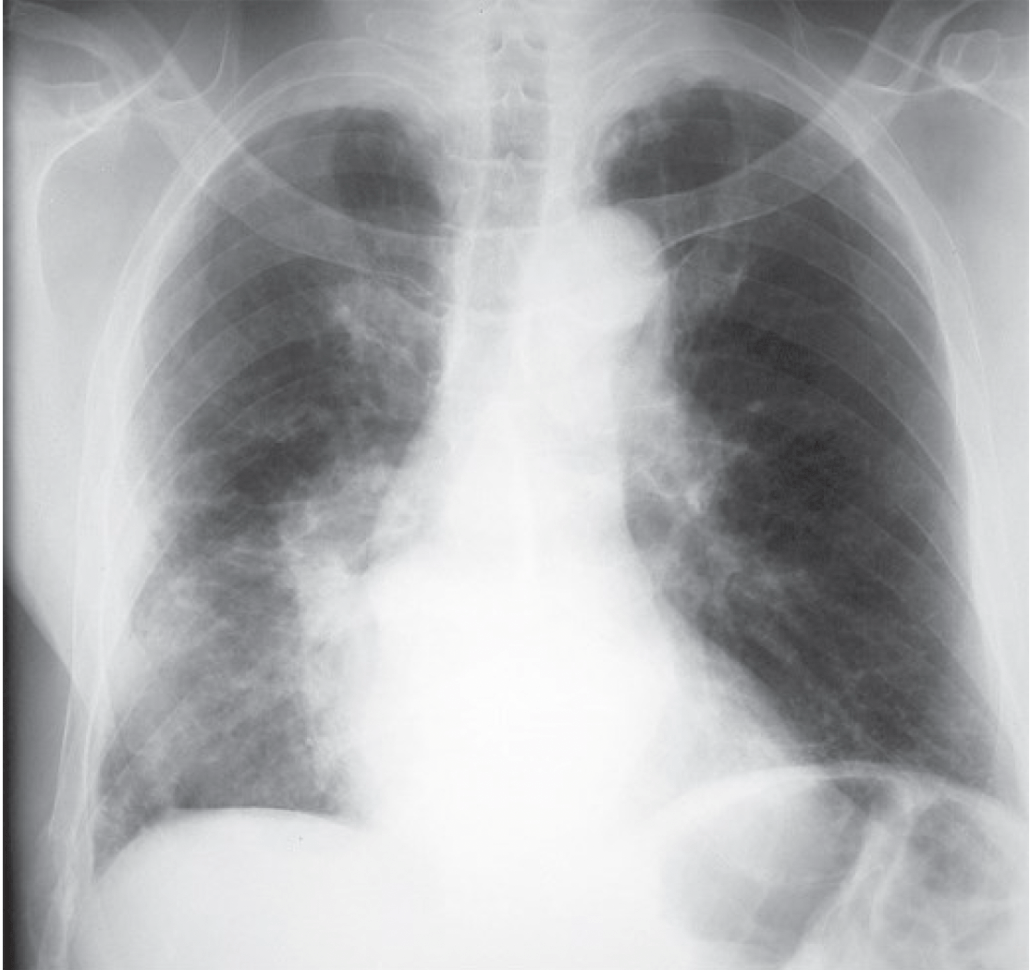
What is the Diagnosis?
What is the most likely diagnosis based on the image?


300
Name the Finding
What does the red arrow represent?
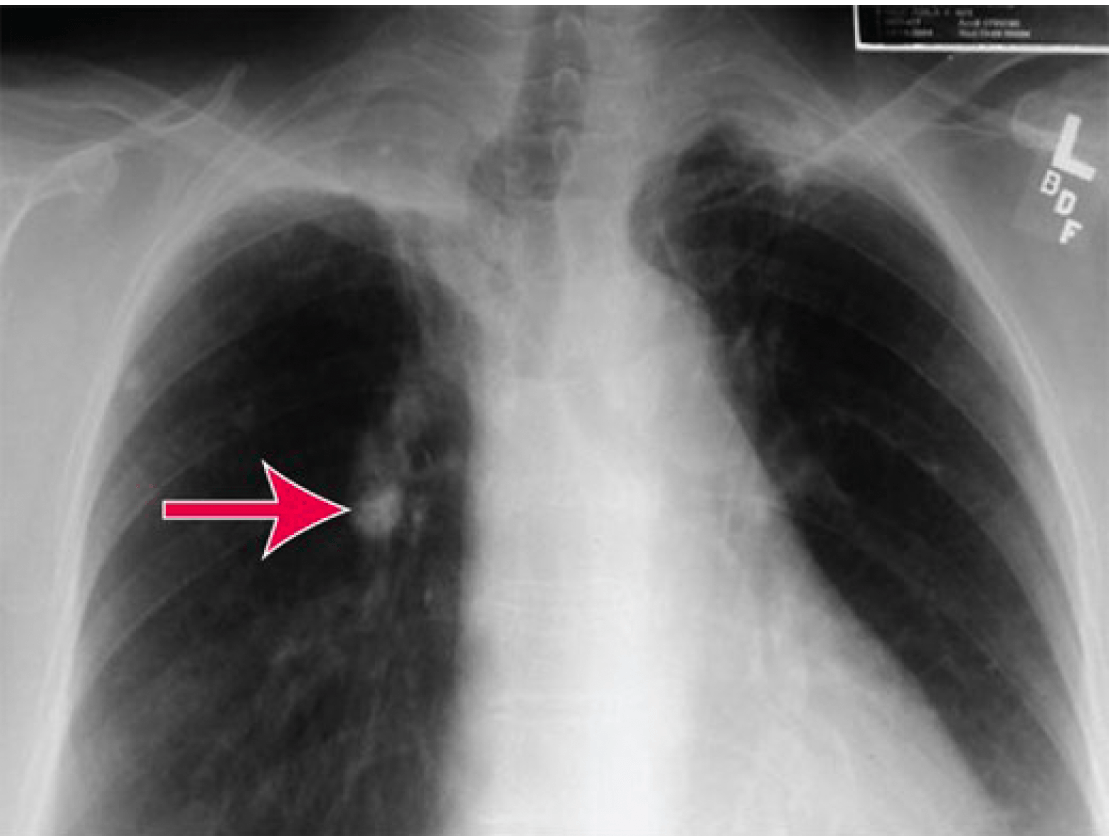
Primary Ghon Complex
The Ghon complex is a tubercle, appearing as calcified hilar lymph nodes.
Mycobacteria are highly antigenic, resulting in a rapid immune response. Some organisms survive in the regional lymph nodes, where the host cell-mediated immunity contains the infection.
Granulomas, known as tubercles, form from this process, which involves activated macrophages, T-lymphocytes, and active bacteria. Tubercles are a sign of primary infection and may progress to caseation necrosis and calcification. These tubercles create a protective area for bacterial growth.
If the tubercle fails to contain the infection, the mycobacteria may spread by hematogenous, lymphatic, or direct mechanical routes.
400
What is the Organism?
Pneumonia in patient with severe cough, sore throat, headache, R-ear pressure, and retrosternal chest pain. On exam there are small blisters over the R-TM.
CXR: Patchy infiltrates, hilar adenopathy, and pleural effusions
Mycoplasma pneumonia
Mycoplasma may cause a subacute respiratory illness with cough, sore throat, and headache, frequently associated with retrosternal chest pain.
CXR shows patchy infiltrates, with the common occurrence of hilar adenopathy and pleural effusions.
Occasionally causes extrapulmonary symptoms, including bullous myringitis, rash, neurologic symptoms, arthritis and arthralgia, hematologic abnormalities, and, rarely, renal failure.

400
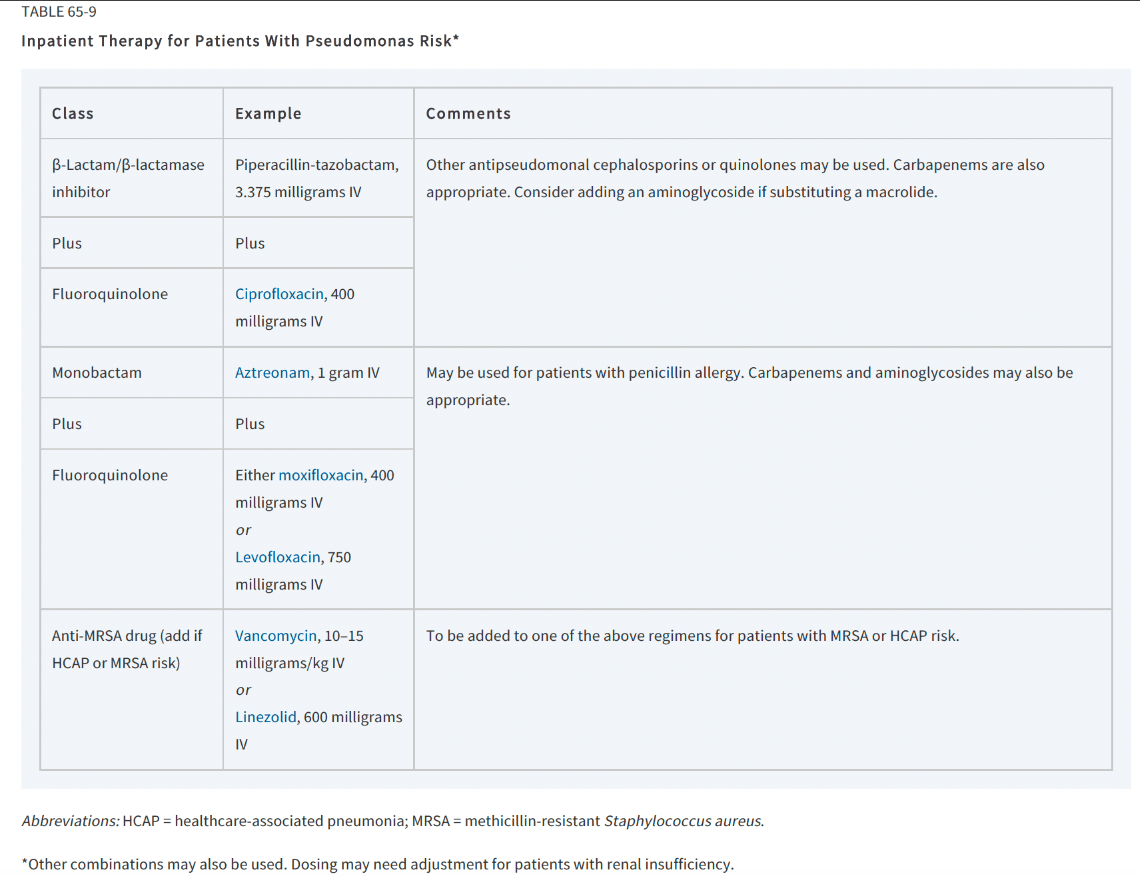
What is the Treatment?
Which of the following is a broad-spectrum antibiotic with coverage against Pseudomonas species?
1- Ampicillin-sulbactam
2- Clindamycin
3- Corticosteroids
4- Piperacillin-tazobactam
Piperacillin-tazobactam (Zosyn)
400
Name the Disease
Systemic granulomatous disease of unknown etiology. Noncaseating pulmonary granulomas.
Sarcoidosis
Symptoms:
Dyspnea, cough, weight loss; skin lesions may also be found. May be asymptomatic.
Chest Radiography Findings:
4 stages: bilateral hilar adenopathy; bilateral hilar adenopathy with reticulonodular pulmonary opacities; pulmonary opacities only; pulmonary fibrosis.
400
Name the Organism
Name 2 major organisms seen in lung abscess?
Type 3 Streptococcus pneumoniae and S. aureus are major causes of lung abscess, with an increasing frequency of Klebsiella pneumoniae infection.
Lung abscess is characterized by localized necrosis of the lung parenchyma and is typically caused by suppurative microbial infection. Initial infection is usually caused by aspiration of oral contents.
400
Diagnostics
The tuberculin skin test becomes positive 1 to 2 [days or months] after initial exposure
1 to 2 months after initial exposure
The skin test becomes positive 1 to 2 months after initial exposure.
Only 1% to 13% of otherwise healthy patients develop active postprimary disease. Children and HIV patients have a higher risk, approaching a 20% frequency of postprimary infection.
Whether latent infection progresses to recurrently active (or “reactivation”) TB is dependent on the immune status of the host.
Latent infection is not transmissible.
500
What is the Type of Pneumonia/Organism?
Groups at higher risk: The elderly, children <2 years old, minorities, children who attend group daycare centers, and persons with underlying medical conditions (including HIV and sickle cell disease)
Most common cause of bacterial pneumonia
Pneumococcal pneumonia
Patients will frequently have lobar pneumonia.
500
Percentage
What percent of patients develop aspiration pneumonia after emergency endotracheal intubation?
Recent research demonstrated that 8% of patients developed aspiration pneumonia after emergency endotracheal intubation.
Emergency Airway Registry III investigators demonstrated witnessed aspiration in 5% of emergency endotracheal intubations, and occult aspiration occurs in 22% to 50% of prehospital emergency intubations.
500
Name the Disease
Reaction of the lung to a number of precipitating causes, including sepsis, trauma, surgeries, transfusions, and therapeutically induced immunosuppression. P/F ratio < 300
Acute Respiratory Distress Syndrome
Symptoms: Hypoxia, tachypnea, rales
Chest Radiography Findings:
Classically, patchy peripheral infiltrates that extend to the lateral lung margins suggest the diagnosis.
500
Diagnostic Criteria
Name 2 of the 4 diagnostic criteria for empyema needed in addition to aspiration of grossly purulent material on thoracentesis
- thoracentesis fluid with a positive Gram stain or culture,
-pleural fluid glucose <40 milligrams/dL,
- pleural fluid pH <7.2, or
- pleural fluid lactate dehydrogenase >1000 IU/L.
500
What is the Treatment?
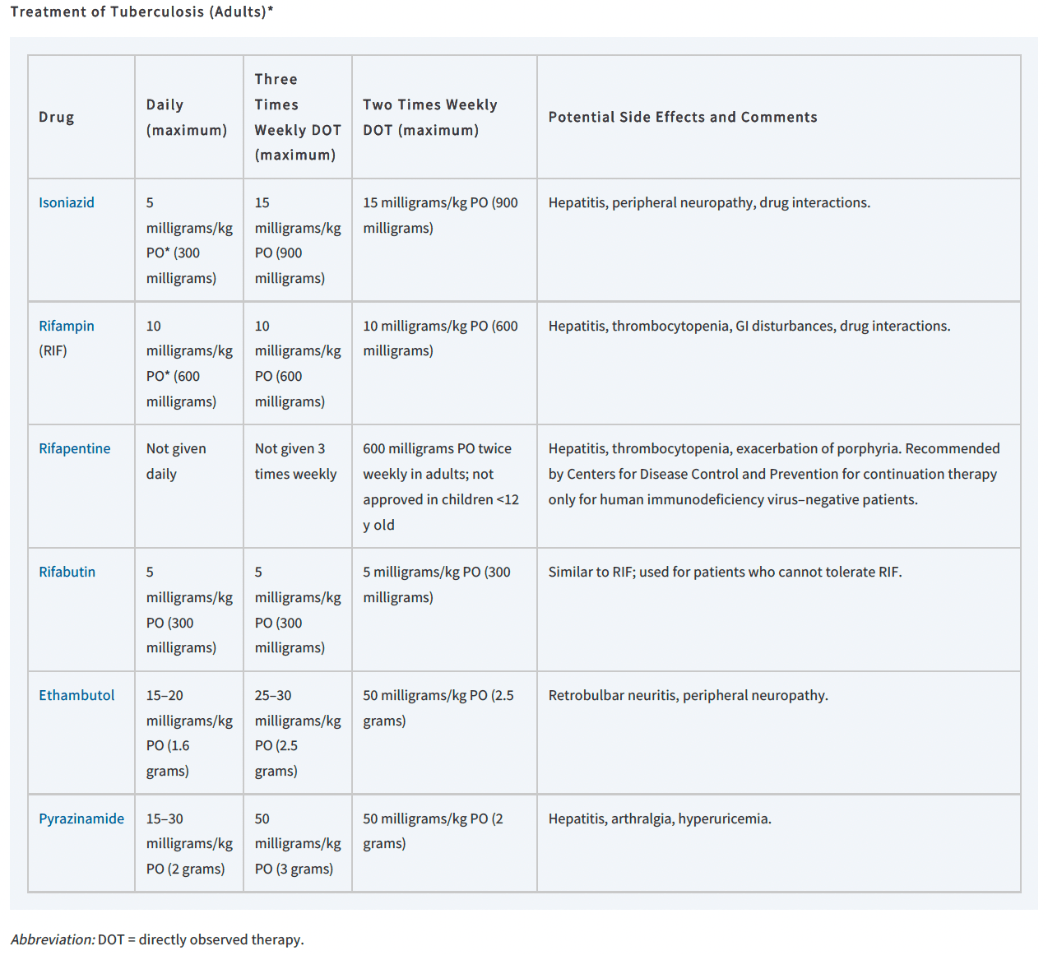
Initial therapy for active tuberculosis includes 4 first-line medications (isoniazid [INH], rifampin [RIF], pyrazinamide, and ethambutol) for [ ] weeks, followed by 2 drug continuation treatment for [ ] weeks based on culture results.
Initial therapy includes four firstline medications (isoniazid [INH], rifampin [RIF], pyrazinamide, and ethambutol) for 8 weeks, followed by two drug continuation treatment for 18 to 31 weeks based on culture results.