Definitions & Pathophysiology
Risk Factors/Imaging
Clinical Presenation/Treatment
Diagnosis/Treatment
Treatment/Complications
100
What categorizes PID?
Infection-caused inflammatory continuum from the cervix to the peritoneal cavity.
100
The majority of woman diagnosed with PID are less than _ (age)
25
100
What is the most common CCs
Lower abdominal pain/pelvic pain, vaginal discharge, dyspareunia, and/or abnormal vaginal bleeding.
"Landers and Sweet found that 35% of women with a TOA were afebrile and 23% had a normal WBC. Furthermore, only 50% of women with a TOA presents with a complaint of fever/chills".
100
PID is a _ diagnosis.
Clinical
100
Name an acute sequelae of PID
Formation of tuboovarian abscess
200
What are the universally accepted etiologic agents of PID?
Neisseria Gonorrhoeae and Chlamydia trachomatis
200
Name some risk factors.
1. Multiple sexual partners.
2. Age.
3. Hx of PID.
4. Recent IUD placement
200
When evaluating for PID what would increase your suspicion on pelvic exam.
Cervical discharge, CMT, uterine tenderness, adnexal tenderness, mass.
200
What should you order aside from STD testing when evaluating a pt with possible PID?
Pregnancy test! Rule out ectopic.
200
Name (3) chronic sequelae of PID
Tubal factor infertility, Ectopic pregnancy, chronic pelvic pain
300
What is the most commonly recovered bacteria from a TOA?
Escherichia coli, Bacteroides fragilis, other Bacteroides species, Peptostreptococcus, Peptococcus, and aerobic streptococci. Interestingly, neither Neisseria gonorrhea nor Chlamydia trachomatis is typically isolated from a TOA. (NIH).
300
There is a significant higher risk during the first _ days post IUD insertion.
A large international study reviewed by Farley et al. found that the overall rate of PID among IUD users was 1.6 cases per 1000 woman-years of use, with a significantly higher risk during the first 20 days post-insertion (9.7 per 1000 woman-years) compared to later periods (1.4 per 1000 woman-years).
300
TOAs greater than _ cm have a greater than 60% chance of requiring surgery.
10cm (compared to 20% in masses sized 4 to 6 cm).
300
Outpatient first line tx per the CDC
1. Doxycycline 100mg BID x 14 days
2. Ceftriaxone 500mg IM x1 OR (Cefoxitin 2g IM w/ probenecid (1g orally) x1 OR another 3rd gen cephalosporin.
+/- Metronidazole 500mg BID x 14 days
300
In patient treatment for PID per the CDC (give 3 regimens)
1. Ceftriaxone 1g IV q24 + Doxycycline 100mg PO q12 + Metronidazole 500mg PO or IV q12 hr.
2. Cefotetan 2g IV q12 + Doxycycline 100mg PO or IV q12
3. Cefoxitin 2g IV q6 hr + Doxycycline 100mg PO or IV q12
4. Ampicillin-Sulbatam 3g IV q6 hr + Doxycycline 100 mg PO or IV q12
5. CLindamycin 900mg IV q8 + Gentamicin
400
Differential Dx for TOA (3)
1. Appendicitis
2. Diverticulitis
3. IBD
4. Ectopic
5. Pyelonephritis
400

Pneumoperitoneum 2/2 to ruptured TOA
400
Describe the CT findings for MOST TOA's
"unilateral, multilocular adnexal mass, enhancing wall thickening of the mesosalpinx, "fat stranding"

400
Indications for hospitalization:
1. Pregnancy
2. Failed outpatient tx
3. Severe clinical illness
4. Abscess
400
There has been shown to be up to a _-fold increase in infertility in women with hx of PID
5
500
Name three conditions that may increased the risk of PID
1. Diabetes
2. Immunosuppression (HIV)
3. BV
500

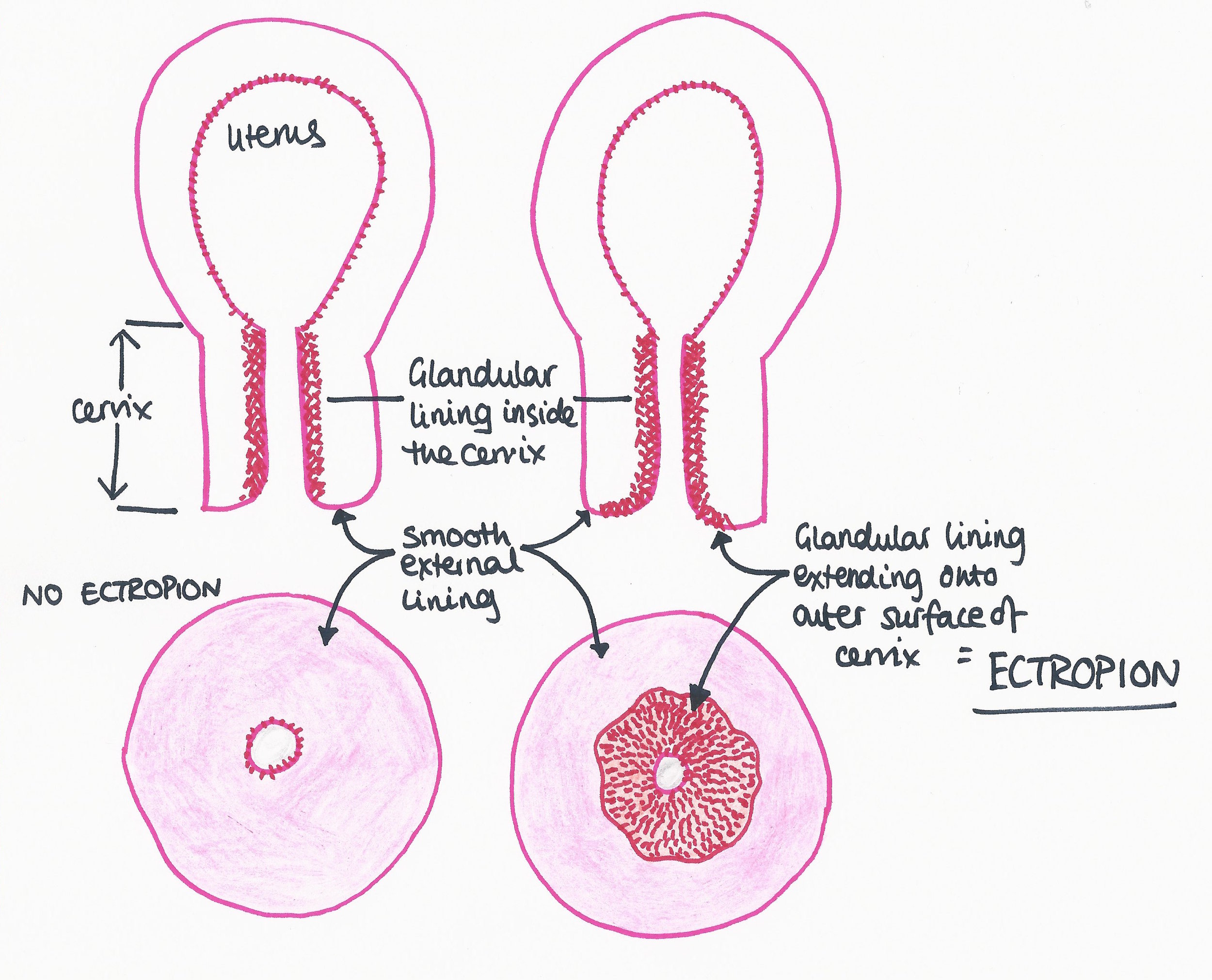
Cervical Ectropion (Columnar epithelium).
Cervical ectopy increases susceptibility to PID by exposing a larger area of columnar epithelium to infection.

500
What is the GOLD STANDARD way for diagnosis of PID/TOA?
Laparoscopy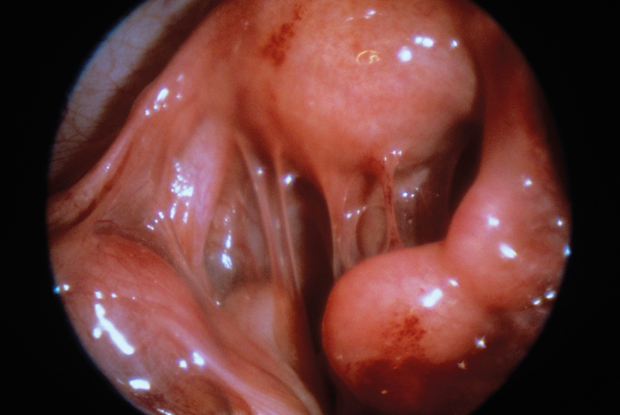
500
In patients greater than _ kg, 1 gram of ceftriaxone should be given instead of 500mg.
150kg
500

What is Fitz-Hugh-Curtis Syndrome