Types of Skull Fractures
Spinal Cord Injury
BASIC SOFT TISSUE TRAUMA
Chest Trauma
Trauma Assessment
100
BASAL (Basilar)
a fracture of the bones that make up the base of the skull, most commonly the temporal bone; commonly includes rupture of the meninges and leakage of CSF.
- Will present with raccoon eyes,
- bruising behind the ears, and
- leakage of CSF or blood from ears and nose.
100
VERTEBRAE- TOTAL BONES
NAMES AND HOW MANY BONES
CERVICAL: C1 C2 C3 C4 C5 C6 C7
THORACIC: T1 T2 T3 T4 T5 T6 T7 T8 T9 T10 T11 T12
LUMBAR: L1 L2 L3 L4 L5
SACRAL: Fused S1/S2/S3/S4/S5
COCCYX: Fused 3 vertebrae
100
DCAP- BTLS
- Deformities/Discolorations
- Crepitus/Contusions
- Abrasion/Avulsion
- Penetrations/Punctures
- Burns
- Tenderness
- Lacerations
- Swelling/Symmetry.
100
Sucking Chest Wounds
Signs and symptoms
TREATMENT
signs and symptoms of these complications are tracheal deviation, shortness of breath, reduced lung sounds, low SPO2%, and hypotension.
- Acquire an airtight (occlusive) dressing for the wound; these may be called "occlusive," "one-way," or "3-sided" dressings.
- Tape this dressing over the wound on 3-sides, ensuring air can escape from one side. This 3-way dressing allows built-up air pressure (and ideally blood) to escape while preventing further air from entering the wound. The open side is the lowermost (or dependent) side, so that gravity can assist blood exiting the wound and it won't fill the pouch-effect like having the open side on the top would.
- Transport the patient at best possible speed to the nearest trauma center.
- Re-assess the patient at regular intervals, even with the placement of occlusive dressings and administration of oxygen, these patients can suddenly and dramatically deteriorate.
100
Scene Size-up
· BSI · Safety
MOI
# of patients
Additional resources needed?
Consider C-Spine Protection
200
DEPRESSED
a depression or sunken-in spot on the skull, usually secondary to blunt force trauma and often associated with
- epidural or subdural bleeding which can result in increased intracranial pressure (ICP),
- brain compression, and
- death even in patients who initially recover.
200
C1 - C4
C5-C8
C1 - C4:
- Considered a high spinal fracture.
- Most severe of the spinal cord injury levels.
- Results in paralysis in arms, hands, trunk and legs.
Quadriplegia--all four limbs affected.
- Patient may not be able to breathe on his or her own, cough, or control bowel or bladder movements. ? Speech is impaired.
C5-C8:
- The nerves that control arms and hands; breathing is weakened; little or no voluntary control of bowel or bladder.
200
ABRASIONS
LACERATIONS
PUNCTURES
ABRASIONS: superficial wounds where the outermost layer of skin is scraped or rubbed off.
LACERATIONS: a cut in the skin caused by impact with a sharp object. The edges are usually rough or jagged unless the object was extremely sharp.
PUNCTURES: different than lacerations because the force is directed towards the body, as opposed to across the body in a laceration.
200
PHYSICAL EXAM FINDINGS
CARDIAC
Distended neck veins may also signify direct cardiac damage. The other findings of cardiac damage are nonspecific.
- ECG and lab tests are required to rule out if cardiac trauma is suspected.
- Hypotension, tachycardia, bradycardia, cyanosis, and low SPO2% are all possible findings, which are unfortunately shared with many other complications of trauma.
- Arrhythmia or abnormal rhythms that are NEW to the patient are common in survivable cardiac trauma.
- By far, the most common sign is sudden death due to cardiac arrest or induction of an unsurvivable rhythm.
200
Initial Assessment
· General Impression
Request ALS?
Responsiveness (AVPU)
Airway · Breathing · Circulation · Bleeding
Identify Priority Patients
300
OPEN
removal of a portion of skull leading to exposure of the brain or meninges, most commonly secondary to penetrating trauma.
- High risk for infection, it may be associated with a deeper injury that is not initially obvious.
- Any skull injury that is draining clear or yellow fluid (CSF) in conjunction with blood should be considered an open fracture.
300
T1-T5
T6-T12
T1-T5:
- Nerves for upper chest, mid-back and abdominal muscles. (Arm and hand function is usually spared).
- Affects the trunk and legs (also known as paraplegia).
T6-T12:
- Nerves for abdominal and back muscles.
- Usually results in paraplegia, with normal upper-body movement.
- Should be able to cough productively (if abdominal muscles are intact).
- Little or no voluntary control of bowel or bladder.
300
STERILE GAUZE
SECURED GAUZE
OCCLUSIVE DRESSING
STERILE GAUZE: The simple placement of sterile gauze over a wound and applying pressure with a gloved hand is the go-to traumatic dressing for a wide variety of situations. Everything from scrapes to stab wounds can be served by this dressing.
SECURED GAUZE: This intervention replaces the source of compression, switching from the rescuer's hand to tape and a specialized pressure bandage.
OCCLUSIVE DRESSING is a non-permeable medical dressing that's used to protect wounds from air, moisture, and contaminants
300
PHYSICAL EXAM FINDINGS
PULMONARY
Breath sounds may be decreased in hemothorax or pneumothorax.
- Abnormal movement of a segment of the chest wall may indicate multiple rib or sternal fractures.
- Stridor or severe wheezing may indicate accompanied tracheal/bronchial collapse/rupture.
- Pulmonary contusion and Acute respiratory distress syndrome (ARDS) are notable for minimal findings on physical exam despite low O2 saturation and dyspnea.
- Hemoptysis (coughing up blood) may indicate damage to the lung tissue, bronchi, or trachea itself has occurred.
300
Rapid Trauma Assessment
DCAP-BTLS + on
Head o Neck (apply C-Collar) Chest o Abdomen
Pelvis, Extremities
Posterior (Place pt on backboard & initiate transport!)
400
LINEAR
most common skull fracture--a simple line through the entire thickness of the skull.
- It usually goes unnoticed until the patient is imaged, often unimportant compared to the traumatic brain injury (TBI) that may have occurred from the same injury.
- As in compressed fractures, linear fractures may result in bleeding beneath the skull.
400
L1-L5
S1-S5
L1-L5:
- Loss of function in the hips and legs.
- Little or no voluntary control of bowel or bladder.
S1-S5:
- Loss of function in the hips and legs.
- Little or no voluntary control of bowel or bladder.
400
PNEUMATIC TOURNIQUET
MECHANICAL TOURNIQUET
MECHANICAL SPLINTING
PNEUMATIC TOURNIQUET: the pneumatic tourniquet is a quickly adjustable method of cutting off the blood flow to an area. Often used for any form of arterial bleeding.
MECHANICAL TOURNIQUET: Using the same philosophy as a pneumatic tourniquet, the mechanical version is generally used for more severe bleeds. Mechanical tourniquets generally cause more trauma to tissue than pneumatic variants but are less prone to failure when used correctly.
MECHANICAL SPLINTING: Certain wounds on extremities are amenable to the placement of rigid support over the gauze that is covering the wound. This offers support to any damaged bones, compression over a wide area, and can act as a partial tourniquet, further slowing the rate of bleeding.
400
PHYSICAL EXAM FINDINGS
VASCULAR
Changes in or absence of pulses in the extremities are a sign of possible vascular damage upstream of the limb or severe blood loss anywhere in the body.
- Distention of the veins in the neck indicates a problem getting blood through the heart, which can be due to damage of the great vessels (The vena cava, pulmonary arteries/veins, and aorta).
- A decrease in the level of consciousness may point to severe blood loss.
- Finally, the presence of a pulsatile mass is concerning for an aneurysm, which can uncommonly result from acute trauma.
400
Last Steps
Determine Transport Priority and to where
Vital Signs (Baseline) BP, RR, HR, Skin, Pupils, SPO2
SAMPLE - If possible
Load and go - Reassessment of vitals 5 or 15 mins
500
EPIDURAL vs SUBDURAL BLEED
- Epidural bleeding is typically arterial.
- Subdural is typically venous.
- Epidural bleeding is more acutely serious.
- Subdural bleeding progresses more slowly.
- Epidural bleeding cannot cross "suture lines," because it is blocked by the falx cerebri--a downward reflexion of the dura mater that dives between the right and left cerebral hemispheres, but is anchored to the skull above (under the suture line). Therefore, all bleeding is compartmentalized and limited by the dura's attachment to the skull. It is this arrangement of anatomy that produces a "midline shift" of the brain on imaging studies.
- Subdural hematomas can cross suture lines, bleeding under and following a route similar to CSF circulation.
- Epidural bleeds are usually due to a strike to the head (sports, etc.)
- Subdural bleeds, especially in children, are usually due to child abuse (skull fractures, shaking).
500
SCOLIOSIS / KYPHOSIS / LORDOSIS
SCOLIOSIS: lateral (sideways) curvature of the spine.
KYPHOSIS: abnormal convexity of the spine ("hunch back").
LORDOSIS: abnormal inward curvature of the lower spine ("swayback").
500
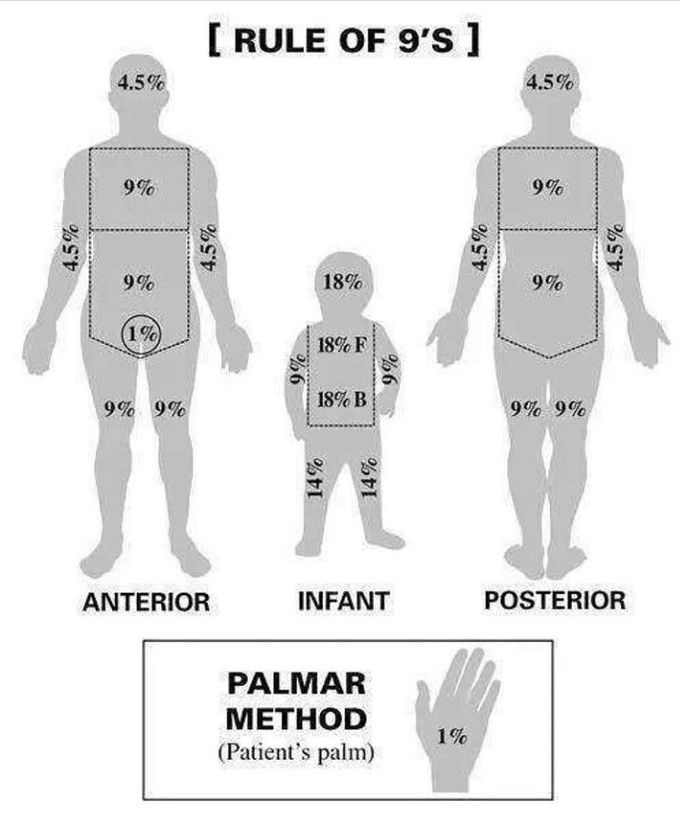
RULES OF NINE & PALMER METHOD
DRAW AND LABEL
ADULT, CHILD, INFANT
500
TENSION PNEUMOTHORAX
SIGNS AND SYMPTOMS
TREATMENT
SIGNS
- Jugular vein distention (JVD)
- Hyper-resonance on one side
- Tachycardia
- Hypotension
TREATMENT of open pneumothorax is focused around the placement of an "occlusive dressing." By placing the dressing, taping down three sides and leaving one end open to the air, you create a one-way valve that seals the chest upon inspiration but allows accumulated air and blood to leave the lung on expiration. Air can still accumulate if the lungs' visceral pleura is also damaged, lifting the dressing off of the wound temporarily will allow any developing tension pneumothorax to decompress.
500
Pediatric Assessment Triangle (PAT)
Appearance: children in traumatic situations should appear stressed, panicked, tearful, and hyperactive or hyperaware. Fatigued-appearing, lethargic, or unresponsive children should prompt significant concern.
Work of Breathing: Nasal flaring, grunting, and intercostal retractions are easy to see in children who are in respiratory distress. The presence of these are also signs of impending respiratory collapse, the small size of children and their increased need for oxygen relative to their size makes decompensation a rapid process when it occurs.
Circulation to the Skin: The final element of the PAT, the presence of cyanosis, cold extremities, or mottled skin are reliable signs that sufficient circulation or oxygenation is not occurring. If a pulse is to be checked in a pediatric patient, the most reliable site is the brachial pulse, which is best felt on the medial aspect of the bicep 2/3 of the way up the upper arm. Blood pressure can be unreliable in young patients, hence the use of circulatory signs as a key part of the PAT.