CMS-1500 Claim Form & Electronic Submissions
Billing and Reimbursement
Collections
Code Sequencing
Coding Instructions
100
What is the purpose of a clearinghouse?
To audit, edit, and transmit medical claims to third-party payers
100
_____is the process of reviewing and paying or denying claims that a healthcare provider has submitted to insurance.
Adjudication
100
What information is typically disclosed to borrowers under the Truth in Lending Act (TILA)?
The Truth in Lending Act (TILA) requires lenders to disclose information such as interest rates, repayment schedules, and any associated fees. Personal credit scores and Social Security numbers are not typically disclosed under TILA.
100
In diagnosis code sequencing, the reason for the patient’s current visit is listed as the primary diagnosis code.
A Sequela codes are used to report how an injury or health condition happened.
B The sequela code—the past disease or condition—is coded first.
C The condition or nature of the sequela—what the patient is currently experiencing—is coded first.
D A sequela should be used only if the acute phase of an injury or illness occurred more than one year ago.
C
The condition or nature of the sequela—what the patient is currently experiencing— is coded first.
A sequela, or late-effect condition, occurs after the acute phase of an injury or illness has ended. The late effect can occur shortly after an injury or illness or years later.
When coding sequela, two codes are usually used. The order of sequela codes is as follows: The condition or nature of the sequela—what the patient is currently experiencing—is coded first. The sequela code—the past disease or condition—is coded second.
100
ICD-10-CM codes are used to report which of the following? Select all that apply:
A Accidents
B Age
C Medical conditions
D Type of health insurance
E Diseases
A, C, E
ICD-10-CM codes are used to report patients’ diseases, conditions, accidents, and injuries.
200
Third-party payers typically will NOT accept CMS-1500 claims that have been __________.
Photocopied and/or non red ink
Explanation: Must be printed in red ink and original copy
200
What is the primary role of an Independent Review Organization (IRO) in the appeals process?
To review the claim denial and render an impartial decision
Explanation:
The role of an Independent Review Organization (IRO) in the appeals process is to review the claim denial independently and render an impartial decision based on the evidence provided.
200
The Fair and Accurate Credit Transactions Act (FACTA) provides consumers with which services?
The right to a free credit check
The Fair and Accurate Credit Transactions Act (FACTA) provides consumers with the right to obtain a free credit report each year from nationwide credit reporting agencies.
200
The ICD-10-CM code J03.90 identifies acute tonsillitis and J35.01 identifies chronic tonsillitis. When both acute and chronic exist, the specialist should code acute first. Both codes are required for a complete diagnosis.
Reason for the current visit with the provider
In diagnosis code sequencing, the reason for the patient’s current visit is listed as the primary diagnosis code.
200
Which of the following categories in the ICD-10-CM is used to report a routine prenatal visit with no complications?
A Z00 Encounter for general examination without complaint, suspected or reported diagnosis
B Z34 Encounter for supervision of normal pregnancy
C O09 Supervision of high risk pregnancy
D O08 Encounter for full-term uncomplicated delivery
Category Z34 is used to report encounters for supervision of a normal pregnancy.
300
Why is the CMS-1500 form printed using red ink?
To allow for optical scanning
The CMS-1500 forms are printed using optical character recognition (OCR) red ink to allow for optical scanning, which means the fields, boxes, and pre-populated text on the forms will be red.
300
What is the purposes of accounts receivable aging reports? Select all that apply:
A To analyze revenue generation patterns
B To monitor the aging of accounts receivable
C To assess payer satisfaction
D To identify unpaid invoices
A,B,D
To identify unpaid invoices; To monitor the aging of accounts receivable; To analyze revenue generation patterns
Explanation:
Accounts receivable aging reports are used to identify unpaid invoices, monitor the aging of accounts receivable, and analyze revenue generation patterns to ensure timely payments and efficient financial management.
300
After a claim is processed by a third party payer, which of the following actions should a billing and coding specialist take to collect the remaining allowed amount?
A Write off the remaining balance
B Submit an adjustment for additional reimbursement
C Call the third-party payer to negotiate a higher rate of reimbursement
D Prepare and send a patient statement
D As per the contract, providers are obligated to collect all patient financial responsibility from the client as their benefits dictate.
300
A patient with Alzheimer’s disease is seen by a provider for worsening symptoms of dementia. Which statement characterizes proper medical coding for the encounter?
A The code for dementia is the etiology code.
B There is no ICD-10-CM code for dementia.
C The code for Alzheimer’s disease should precede the code for dementia.
D The code for Alzheimer’s disease is the manifestation code.
C The code for Alzheimer’s disease should precede the code for dementia.
Explanation:
Dementia is a manifestation of Alzheimer’s disease, which is the underlying etiology. The code for the etiology should precede the code for its manifestation.
300
A patient presents to their providers office with a sore throat, and the provider diagnoses acute and chronic tonsilitis. Which of the following ICD-10-CM codes should the billing and coding specialist use for this diagnosis?
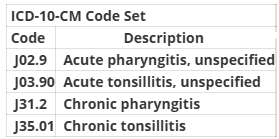
A J02.9, J31.2
B J35.01, J31.2, J35.01, J03.90
C J35.01, J03.90
D J03.90, J35.01
D
The ICD-10-CM code J03.90 identifies acute tonsillitis and J35.01 identifies chronic tonsillitis. When both acute and chronic exist, the specialist should code acute first. Both codes are required for a complete diagnosis.
400
For a provider with a non-NPI ID number, in which item number on the CMS-1500 claim form should the ID qualifier be recorded?
A Item Number 24I
B Item Number 10a
C Item Number 33b
D Item Number 32b
A Item Number 24I
Explanation:
If the provider has a non-NPI ID number reported in Item Number 17a, that number should be recorded above the dotted line in the shaded section of Item Number 24J, and the ID qualifier should be recorded in Item Number 24I.
400
A billing and coding specialist is reviewing a Medicare electronic remittance advice. The remittance advice indicates a payment of $80.00 for a wellness exam. The billed amount was $220.00 and the allowed amount was $80.00. Which of the following actions should the specialist take?
Post the payment and write off the difference
Since the payer determined the allowed amount was $80.00 and reimbursed $80.00, the patient financial responsibility is $0.00. The remainder should be written off.
400
A billing and coding specialist is reviewing a remittance advice that has a remark code that indicates a claim is pended for review of medical records. Which of the following actions should the specialist take?
A send the requested medical records to the third-party payer
B resubmit the claim to the third party payer as a corrected claim
C notify the third-party payer to review the claim for payment
D advise the patient that they will be responsible for the charges not covered by the payer
A The specialist should send the requested medical records to the third-party payer for processing.
400
Which language in the ICD-10-CM coding manual should alert a coding specialists of the need for a secondary code?
"use additional code"
Some conditions require more than one diagnosis code to be reported. The note “Use additional code” will be listed next to the codes for these conditions.
400
A billing and coding specialist is completing a claim for a new patient who reports swelling in their ankles. The provider performs an appropriate history and examination, with high complexity medical decision-making, spending 60 min with the patient. Which of the following Evaluation and Management (E/M) codes should the specialist select?
A 99285 Emergency department visit of a patient which requires a medically appropriate history and/or examination and high medical decision-making
B 99205 Office or other outpatient visit for a new patient which requires a medically appropriate history and/or examination and high medical decision-making
C 99214 Office or other outpatient visit for an established patient which requires a medically appropriate history and/or examination and moderate medical decision-making
D 99215 Office or other outpatient visit for an established patient which requires a medically appropriate history and/or examination and high medical decision-making
B
The specialist should select E/M code 99205. This code describes new patient E/M services, including a reported time spent with the patient of at least 60 min.
500
Which of the following information is needed to accurately review, evaluate, and resolve denied claims?
A An aging report breakdown of a patients account
B A remittance advice with reason codes
C Registration notes
D SOAP notes
B The remittance advice from the third-party payer shows the allowed amount, adjustments, or reason for denial.
500
A billing and coding specialist receives a denial from a third-party payer due to missing information. Which of the following actions should the specialist take to receive reimbursement?
A Request reimbursement from the patient
B Submit an adjustment
C Contact the third-party payer to provide the information
D Resubmit the claim with the completed information
D The specialist should resubmit the claim with the completed information.
500
Which of the following is an example of a clinical data abstraction error?
A Incorrect date of service was used.
B Authorization was not obtained
C Referral request for a mammogram was billed as charges
D Secondary insurance was billed as primary insurance
C Billing as charges when a referral request is created in the patient chart is an example of an abstraction error.
500
Which of the following is reported when using an external cause code? Select ALL that apply
A Whether the injury was intentional or unintentional
B Names of individuals responsible for causing the injury
C Severity of the injury
D How the injury happened
E the place where the injury occurred
A D E
How the injury happened, whether the injury was intentional or unintentional, the place where the injury occurred
External cause codes are not reported as a first-listed diagnosis. The appropriate injury code should be reported before the external cause. The first-listed diagnosis code tells what happened to the patient and the external cause code provides more information about the injury.
500
A child received a measles, mumps, rubella, and varicella (MMRV) vaccine with provider counseling. Which of the following CPT codes should be reported for the vaccine and administration?
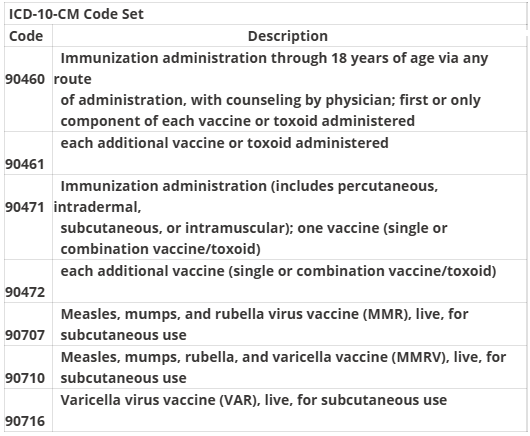
90710, 90460, 90461 x 3