Abdominal Vascular Trauma
Extremity Vascular Trauma
Extremity Vascular Injury Complications
Thoracic Vascular Trauma
100
Describe 3 Zones of the retroperitoneum?
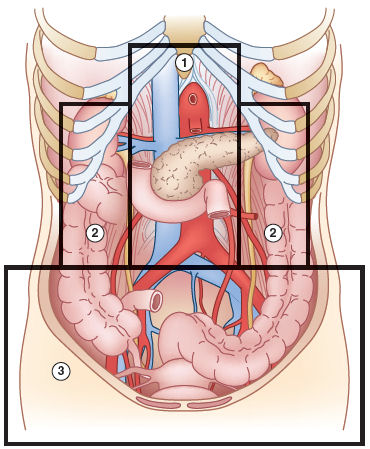
Zone 1: This zone begins at the aortic hiatus and ends at the sacral promontory.
Zone 2: This zone is located at the pericolic gutters.
Zone 3: This zone begins at the sacral promontory and encompasses the pelvis
100
3 soft signs of vascular extremity injury?
A diminished but palpable pulse, a non-expanding hematoma, a nearby nerve injury, unexplained hypotension, a history of significant bleeding, proximity of a wound to a major blood vessel, or a bone fracture close to a major vessel.
100
Indication for a prophylactic fasciotomy in a patient with vascular injury to the extremity?
Prolonged limb ischemia (greater than 6 hours), combined arterial and venous injury in an extremity, massive soft tissue trauma (crush injury), or complex vascular repair with high-risk factors for tissue compromise
100
3 signs concerning for blunt aortic injury in a trauma patient following a MVA?
Widened mediastinum; 1st/2nd rib fractures; left hemothorax; apical capping; tracheal deviation to the right; sternal fracture, scapular fracture; loss of AP window.
200
3 symptoms of abdominal compartment syndrome?
Hypotension, hypoxia, distended abdomen, low urine output, bladder pressures > 25-30; IVC compression leading to decreased cardiac output. upward displacement of the diaphragm leads to hypoxia. Low cardiac output leads to renal malperfusion.
200
3 hard signs of vascular injury to the extremities?
Pulsatile bleeding, expanding hematoma, absent distal pulses, bruit or thrill on auscultation, and signs of distal ischemia (like pallor, pain, paresthesia, paralysis)
200
Diagnosis of compartment syndrome in patient with prolonged lower extremity ischemia following vascular trauma?
Clinical diagnosis. Pain with passive motion; tense muscle compartments; compartment pressures > 30 mmhg. 6Ps.
200
Indications for OR thoracotomy following placement of a chest tube in the trauma bay?
> 1500 cc after initial insertion, > 200 cc/hr for 4 hours, > 2500 cc/24 hr, bleeding with instability.
300
3 key principles of damage control surgery?
- Rapid control of hemorrhage: The primary preventable cause of death in trauma patients is hemorrhage.
- Temporary control of contamination: This is achieved by inspecting the bowel wall and closing any perforated viscus.
Resuscitation in the intensive care unit (ICU): This phase restores normal physiology and involves a thorough examination to identify all injuries.
300
Management of patients with soft signs of vascular injury to the extremity?
CTA with bilateral LE run offs.
300
What makes up the Mangled Extremity Severity Score (MESS)? What value correlates with primary amputation?
Age, limb ischemia, shock, skeletal/soft tissue injury. Score of 7 or more indicates primary amputation.
300
Most likely location for an aortic tear?
Proximal descending thoracic aorta at the ligamentum arteriosum.
400
When is damage-control laparotomy is considered appropriate?
Damage-control procedures should be considered in patients in extremis who have exhausted their physiologic reserves and are in danger of irreversible shock and death. The criteria include coagulopathy, hypothermia (temperature < 35°C), base deficit greater than 15 mEq/L (15 mmol/L), and severe bowel edema.
400
Management of stable patient with pulsatile hematoma following GSW with comminuted fracture of right femur?
Hard signs requires emergent OR for exploration. Vascular repair prior to orthopedic repair.
400
Most commonly damaged nerve during a 4 compartment fasciotomy an the effects?
Superficial Peroneal Nerve. Affects foot eversion.
400
Operative approach for a injury to the descending thoracic aorta?
Left thoracotomy
500
Describe the repair a posterior wall infrahepatic IVC injury?
Right medial visceral rotation which involves the medial rotation of the right-sided abdominal viscera (except the kidney) allows for visualization of the entire infrahepatic inferior vena cava. Repair of posterior wall through anterior IVC.
500
Repair of LE arterial injuries > 2 cm?
GSV interposition graft from contralateral LE; PTFE
500
Most commonly missed compartment during a 4 compartment fasciotomy? How do you ensure this compartment is not missed?
Deep posterior compartment. The deep posterior compartment is decompressed by elevating the soleus muscle from the tibia.
500
Operative approach for a distal right subclavian artery injury?
Mid clavicular incision with resection of medial clavicle. The median sternotomy should be reserved for injuries to the heart, ascending aorta, innominate artery and vein, and superior vena cava. The anterolateral incision is used as a resuscitative thoracotomy. The descending thoracic aorta may be cross-clamped through this incision.