Polymers+Monomers
Polymers+Monomers cont..
Composites
Composites Cont..
Composties cont..
100
___1___are materials that are made of large, long molecules formed by chemically reacting chains of monomers.
The chemical reaction that links the monomers together to make a polymer is called __2__.
1. Polymers (poly=many)
2. Polymerization
100
Addition Polymerization is also called ____
Free Radical
**The atmospheric oxygen inhibits addition polymerization ***
100
1. Silane coupling agents act as a coating and serve to transfer stress from a weak component to a weaker one.
2. Depth of cure is the specific amount of composite (Thin layer) that is cured by a light.
Both Statements are FALSE
1. weak component to a STRONGER one.
2. THICK Layer
100
What material would typically be used to restore a small chip on an anterior tooth?
A. Amalgam restoration
B. Porcelain
C. Composite Resin
D. Gold onlay
C. Composite Resin
100
Dental Composites-Combination of two materials
1. ______- is soft, weak, flexible, and prone to wear.
2. ______- engineered glass material formulated to have proper strength, hardness, and chemical properties for use in dental composites.
1. Matrix
2. Filler
200
Materials are called ____1__ because they can be heated and molded, shaped, after polymerization reaction, like wax.
1. Thermoplastic
200
Acrylic resins, composite materials for restorative work, cements, sealants, and adhesives all set by ______ _____. Also known as Free Radical.
Addition Polymerization.
200
Ceramic Filler Particles coated with _____ to:
-increase strength,
-make more tooth like structure,
-decrease polymerization shrinkage,
-decrease thermal expansion.
Silane Coupling Agents
200
It is possible to bond a new composite to an existing cured layer of composite.
True,
-Due to the Depth of Cure, the thickness of the composite is determined by the light source.
-If the composite material nearest to the pulp is not fully cured, pulpal irritation and postoperative sensitivity will occur. To prevent this, composite material is placed in a thin layer (>3mm thick) at the bottom of the preparation and cured before the next layer is placed.
200
Procedure for Composite Polishing:
-Explain the rationale of composite polishing
-Review steps of the procedure with the patient
-Inform patient of sensations he or she may experience during the process, especially those of finishing burs with a low-speed handpiece.
Pair up and share your rationale.
300
Material that is CROSSED-LINKED, which cannot be heated to melt or molded. Stronger and Tougher, decomposes rather than melt is called ______.
Thermoset Polymers
300
Name the steps in Addition Polymerization:
1.
2.
3.
1. Initiation-Activation of free radicals, free radical grows. Formation of Free Radicals
2. Propagation -Growth of lengthening the chain
3. Termination-Carbon-Carbon bond, no free radicals are left to continue growth of the chain.
300
Types and Properties of Dental Composites:
1. ____ filled
2. ____ filled
3. ____ composites
1. Microfilled
2. Macrofilled
3. Hybrid Composites
300
Which of the following requires visible light curing for setting?
A. Polyvinyl siloxane
B. Posterior Composite
C. Dental Amalgam
B. Posterior Composite
300
Rationale for Composite polishing: Let your patient be in the know.
-To create a restoration that is smooth, uniform, and easily cleaned by the patient.
-Increases longevity of restoration.
-Decreases the incidence of recurrent caries.
-Promote the health of surrounding tissues
-Patient will feel water and vibration from polishing.
400
Some characteristics of Thermoplastic Polymers....
**Think **Plastic-(surgery)-can change when heated.

-Soften when heated, they can be molded and cooled to harden. (plastics)
-They can soften again on heating.
-They are usually soluble in organic solvents
-Long linear chains
400
True or False:
Problems with Polymers are that they can shrink and expand.
True
400
Advantages of Micro vs Macro
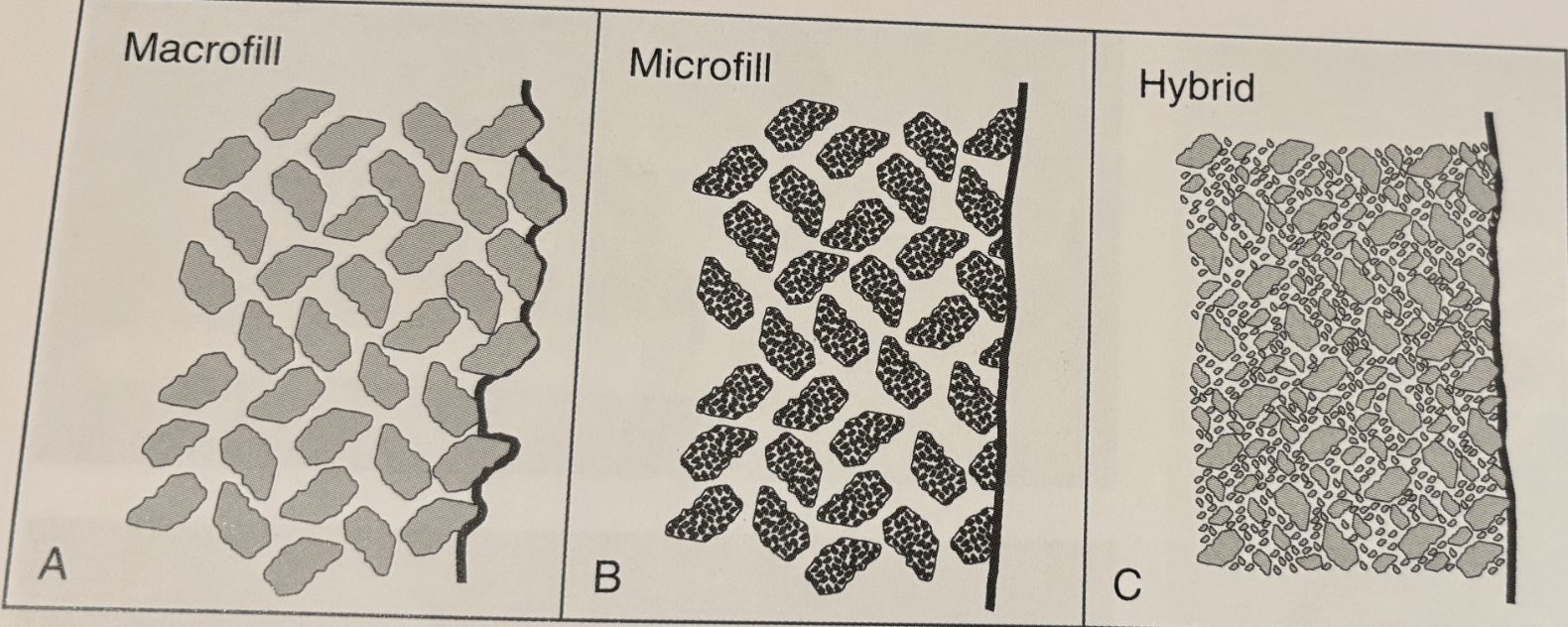
1. Macrofilled- feels rough and appears rough and unfinished. Developed in 1960's when placed on posterior teeth resulted in postoperative sensitivity, leakage, and recurrent decay.
2. Microfilled- Developed in 1970's. Polish very smoothly and Lustrous. Smaller particles than Macro. Best to use for Class V restoration, more likely to retain due to elasticity and flex.
400
Indications for Composite Polishing:
**skills test on composite polishing,
**Care of Restoration evaluation only done on Amalgam.
-Overextension
-Premature occlusal contact
-Limited stain
-Limited re-contouring of anatomy
-Small chips or defects
400
Steps in Composite Polishing:
Evaluate restoration (use an explorer... but DON’T scratch it).
1. -Dry restoration with air, visually inspect the contours to detect proper anatomical form, chips, voids, stains, or defects....
2. Dura-Green: silicon carbide stones for adjusting.
3. Dura-White: aluminum oxide stones for finishing.
4. CompoSite: silicone points are impregnated with aluminum oxide for polishing.
Polishing points, disks or cups
5. Occlusal contacts can be evaluated using articulating paper.
6. Use the explorer to examine the margins gently.
500
Some characteristics of Thermoset Polymers....
**Think ** SET in your ways, cannot change, cannot warm up. **

-They are molded and polymerized in the Final Shape
-They are resistant to change when heated
-They are usually insoluble
-The chains are cross-linked
500
1. Polymeric materials have high coefficients of thermal expansion compared to tooth structure.
(T or F)
2. The coefficient can be 2 to 10 times greater than the tooth structure.
(T or F)
Both states are True.
-Repeated expansion and contraction of polymeric materials can Percolate (open and close gaps at the margin of restoration)
-Resulting in recurrent decay and microleakage increase.
500
Hybrid Composite- Develped in 1980's, Smallest Nanofilled particles , Most widely used on the market, very popular.
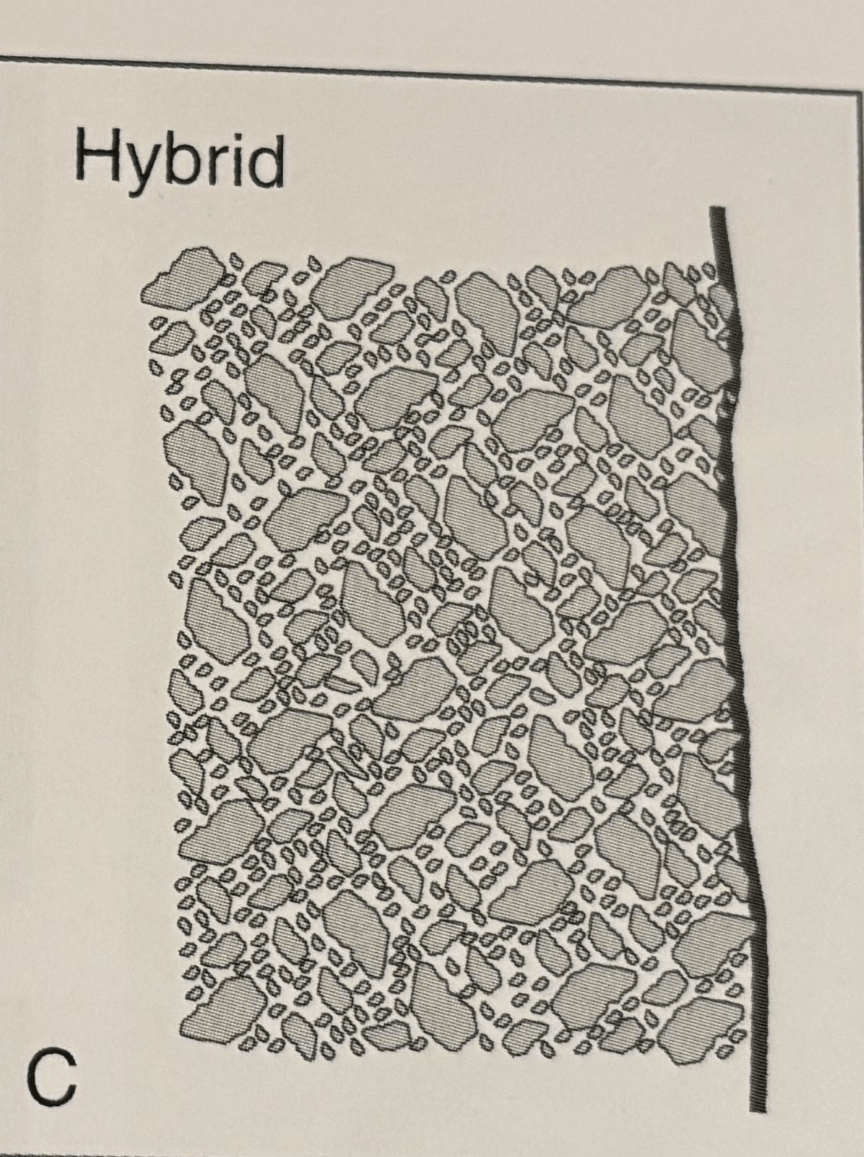
-Strong, polishes well
-Replaced Microfilled Composites, the most popular
-Has a range of particle , Nanosized/Nanofilled
-Accepted use for small to medium Class I, II, III and IV restorations
500
-Placing composite in __1__
-Assures adequate ___2__
-Material allowed to ___3__before adding additional layers
1. Layers
2. Polymerization
3. Shrink
500
In the United States, standards for dental materials are developed and administered by the:
A. ADA (American Dental Association)
B. FDA (Food and Drug Administration)
C. AADR (American Association for Dental Research)
D. OSHA (Occupational Safety and Health Administration)