The Patient Must Survive the Workup
Obstruction Destruction!
Get Rhythm
A Perfectly Bad Heart
Bugs n' Drugs
Alex's Mystery Mix
100
A patient presents with classic ischemic chest pain and ST elevations in contiguous leads. This action should occur immediately, rather than waiting for cardiac biomarkers.
What is activating the cath lab?
100
In the setting of a higher risk PE (categories C-E), promptly activating this team of specialists has been shown to improve patient mortality.
What is the PE Response Team (PERT)?
100
This atrial arrhythmia typically occurs due to a single organized re-entry circuit, which helps to explain its morphology.
What is atrial flutter?
100
A patient with a low cardiac index, high PCWP, and high SVR fits this classic hemodynamic profile.
What is cold and wet?
100
This organism is the most common cause of infective endocarditis.
What is Staphylococcus aureus?
100
The most common type of syncope across all age groups, this condition usually has prodromal warning signs - which you can uncover by taking a good history.
What is reflex syncope?
200
You'll need to order these two tests in a patient presenting with new and undifferentiated syncope.
What are EKG and Orthostatic VS?
200
Cardiac tamponade and tension pneumothorax mainly cause obstructive shock by impairing this aspect of cardiac function.
What is preload or venous return?
200
The EKG below shows this rhythm:
What is atrial fibrillation?
200
An 80 y/o M with a history of HFrEF 20% presents to the ED with AMS. On presentation he is lethargic, oriented to self, and his extremities are cool. What's your first move for treatment?
A) 1 L IVF bolus
B) Initiate inotrope/vasopressor support
C) Administer high-dose lasix
D) Activate the cath lab
What is B) Inotrope/vasopressor support
200
This class of beta-lactam antibiotics is considered broad-spectrum, but they don't cover MRSA.
What are the cephalosporins?
200
Of these four patients diagnosed with acute pulmonary embolism confirmed by CTPA, which of the following is the most appropriate candidate for outpatient management?
A. A 52 y/o M with HR 88 bpm, BP 124/76 mmHg, SpO₂ 95% on RA, no history of cardiopulmonary disease, normal troponin and BNP, and reliable access to follow-up care
B. A 67 y/o F with HR 102 bpm, BP 118/72 mmHg, SpO₂ 93% on room air, history of HFrEF, and mildly elevated BNP
C. A 45 y/o M with HR 110 bpm, BP 100/64 mmHg, SpO₂ 91% on room air, and reports of near-syncope at home
D. A 60 y/o F with HR 92 bpm, BP 122/70 mmHg, SpO₂ 98% on room air, lives alone and reports difficulty obtaining medications and follow-up care
What is patient A: 52 y/o M with HR 88 bpm, BP 124/76 mmHg, SpO₂ 95% on RA, no history of cardiopulmonary disease, normal troponin and BNP, and reliable access to follow-up care
300
A patient presents to a rural hospital with chest pain and is discovered to have an acute inferolateral STEMI. The nearest PCI-capable facility is 3 hours away. What is the most appropriate action?
A) Administer fibrinolytics
B) Start IV heparin bolus + infusion and prepare the patient for fixed wing transport
C) Start IV beta blockers and a glycoprotein IIb/IIIa inhibitor
D) Obtain CT coronary angiography for risk stratification
What is A) administration of fibrinolytics?
300
This physical exam finding helps differentiate a tension pneumothorax from cardiac tamponade (and other conditions)!
What is unilateral absent breath sounds?
300
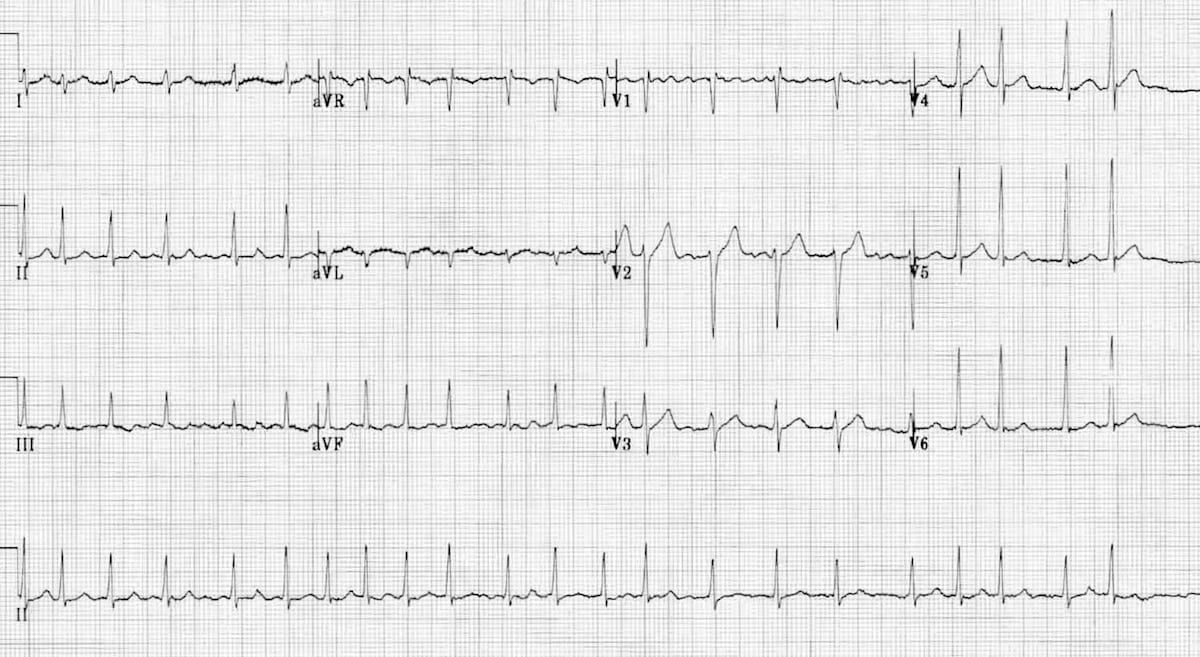
Describe the axis on the EKG below: 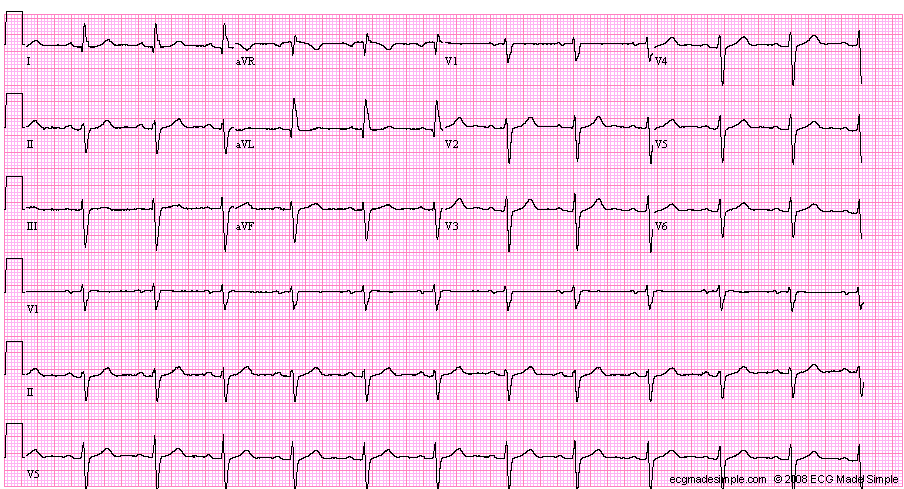
What is left axis deviation?
300
Patients with this condition may present after a syncopal episode without warning signs. The left ventricle EF is often normal (or even high), and there will be diastolic dysfunction and an enlarged left atrium.
What is hypertrophic cardiomopathy?
300
Compared to the 1st-generation cephalosporins (e.g., cefazolin), the 2nd-generation cephalosporins have more activity against this type of bacteria.
What are gram-negative bacteria?
300
You are evaluating a 45-year-old patient in the ED with a history of HTN presenting with headaches who is found to have a BP 190/78. On medication review, you note that they are on HCTZ, lisinopril, and amlodipine at high doses. You should first be highly suspicious for this problem.
What is secondary hypertension?
400
A patient with a history of pulmonary hypertension presents with hypotension and signs of RV failure. What is the most appropriate initial action?
A. 1 L IV fluid bolus and stat CTPA
B. 1 L IV fluid bolus and prepare for R heart catheterization
C. IV norepinephrine
D. Immediate diuresis
What is C. IV norepinephrine?
400
A patient with hypotension, JVD, and muffled heart sounds on exam may be experiencing this life-threatening condition.
What is tamponade physiology?
400
In the EKG below, there is a bundle branch block! But is it LBBB or RBBB, and why?

What is a RBBB?
LBBB and RBBB are distinguished by ECG by looking at the QRS complex in leads V1 and V6.
LBBB shows a wide, negative QRS (deep S) in V1.
RBBB shows a wide, positive QRS (rSR'/rabbit ears) in V1.
400
You are a cardiology ACNP evaluating a patient in clinic with recently diagnosed Afib. You have chosen to pursue a rate-control strategy for now. Per the ACC guidelines, you should aim for this resting heart rate.
What is < 110 beats/min?
400
Your ICU patient's blood cultures came back, and they are growing Candida albicans. Which action should be taken first?
A) Order repeat blood cultures due to likelihood of contamination
B) Start treatment with IV fluconazole (Diflucan)
C) Perform immunosuppression workup
D) Order additional cultures including sputum and urine cultures
What is B) Start treatment with IV fluconazole (Diflucan)
400
Congratulations! You just passed your ACNPC-AG boards exam, sanctioned by the American Association of Critical-Care Nurses (AACN). You can now consider yourself to be which of the following?
A. Licensed
B. Credentialed
C. Certified
D. Accredited
What is C - Certified!
500
You are evaluating an adult male who was the restrained passenger in a high-velocity rollover motor vehicle crash. Primary and secondary survey were unremarkable. He is hemodynamically stable and protecting his airway. FAST exam was negative. You plan to order this imaging to comprehensively evaluate for internal injuries.
What is a CT head, neck, chest, abdomen, and pelvis (pan scan)?
500
A 72-year-old patient presents with chest pain, hypotension (BP 78/50), JVD, and clear lungs. You suspect obstructive shock due to pulmonary embolism. EKG shows sinus tach at 110, no STEMI. SpO2 is not reading due to poor pleth. What should you do next?
A) Send the patient for a CTPA
B) Start heparin
C) Perform bedside TTE
D) Order a stat troponin
What is C) Perform a bedside TTE
500
This EKG is suspicious for myocardial injury to this wall:
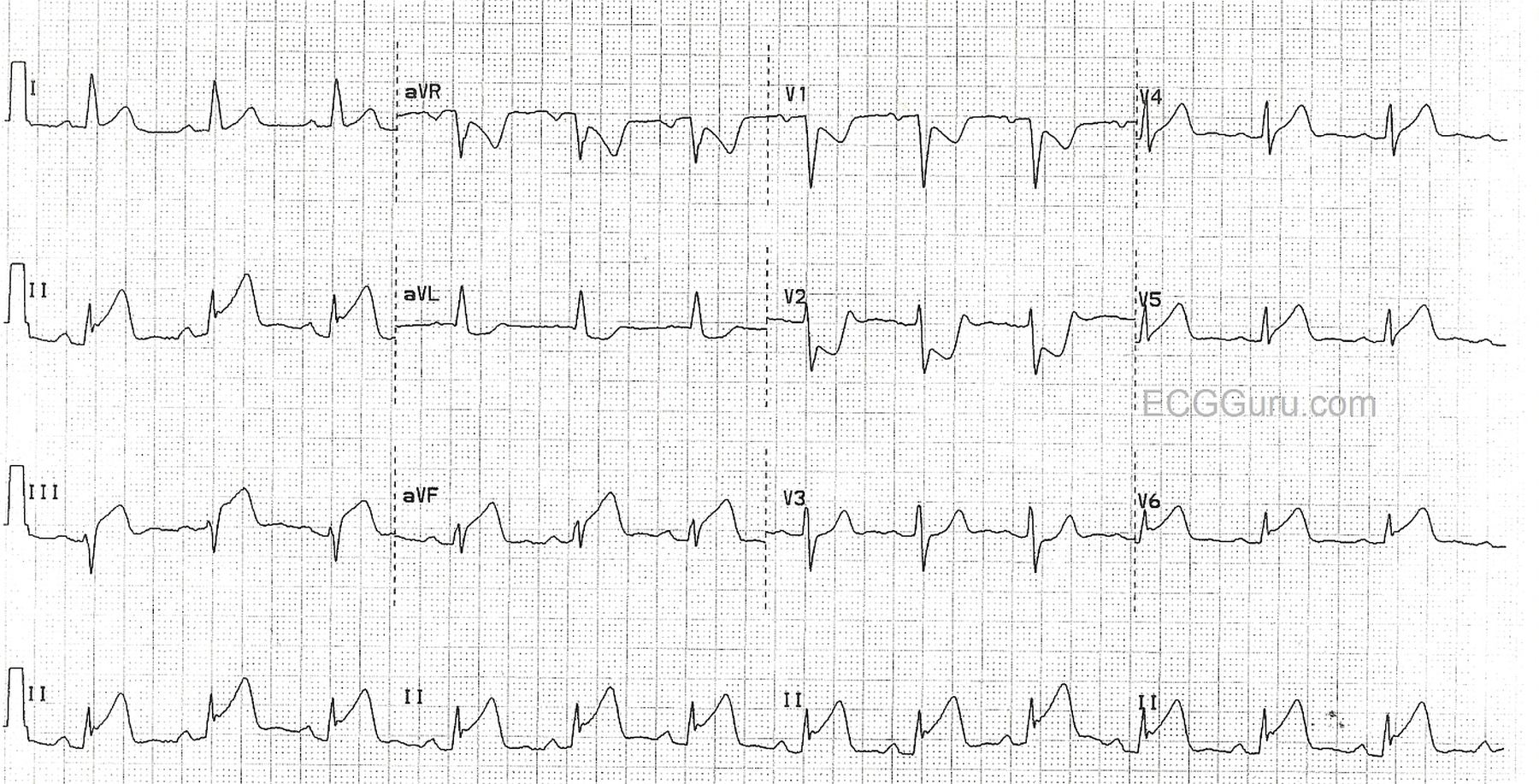
What is the inferior wall?
500
Which of the following patients should NOT receive a DOAC as first-line anticoagulation?
A) A 70 y/o with nonvalvular AF
B) A 65 y/o with stage 2 chronic kidney disease
C) A 75 y/o with a prosthetic aortic valve
D) A 50 y/o with type 2 diabetes and cirrhosis
What is C) a 75 y/o with a prosthetic aortic valve
500
You are a hospitalist NP evaluating a patient who has been hospitalized for a month who has developed pneumonia. Sputum cultures are pending. Which of the following antibiotics would be appropriate to start for empiric treatment?
A) Ceftriaxone
B) Azithromycin
C) Piperacillin-tazobactam
D) Amoxicillin-clavulanate
What is C) Piperacillin-tazobactam
-Broad-spectrum with antipseudomonal gram negative coversage
-Appropriate for hospital-acquired PNA
500
You are evaluating a 60-year-old patient who was found down after an unwitnessed fall. You'll plan on suspecting this condition until proven otherwise.
What is syncope?
600
You are evaluating a hemodynamically stable patient with penetrating chest trauma who is found to have a small pericardial effusion on eFAST. Which of the following actions is appropriate?
A) Stat CT chest
B) Repeat echocardiogram in 6 hours
C) Urgent surgical exploration
D) Pericardiocentesis
What is C) urgent surgical exploration?
600
Your patient with category D acute PE is getting more hypotensive despite pressors, and you're thinking of giving them a fluid challenge. You might think about obtaining one of these first.
What is an echocardiogram?
600
You're reviewing your patient's EKG, and something just doesn't seem right! What is the can't-miss abnormality noted below, and what is its clinical significance?

What is a prolonged QTc?
Prolonged QTc increases the risk of ventricular dysrhythmia, particularly polymorphic VT (torsades de pointes). Check their electrolytes and review their medications for QT-prolonging agents!
600
You're evaluating a patient in the CCU with the following hemodynamic parameters:
-CI: 1.7 mL/min/m2
-PCWP: 26 mmHg (elevated)
-SVR 1750 dynes/sec/cm-5 (elevated)
Which treatment is indicated?
A) Inotrope +/- vasopressor support
B) Initiation of VV ECMO
C) IV fluids
D) Beta blocker
What is A) Inotrope +/- vasopressor support?
600
A 72-year-old ICU patient with a central line, recent prolonged hospitalization, and TPN develops fever, hypotension, and altered mental status. You suspect severe sepsis from an unknown source. Which of the following antibiotics provides the broadest empiric coverage and is most appropriate to initiate?
A. Cefepime
B. Piperacillin-tazobactam
C. Vancomycin
D. Meropenem
What is D. Meropenem?
600
These are the 5 steps of the sepsis one-hour bundle.
What are 1) Measure lactate, 2) Obtain blood cultures before antibiotics, 3) Start broad-spectrum antibiotics, 4) Administer 30 mL/kg crystalloid fluid bolus for hypotension or lactate >=4, 5) Start pressors if hypotensive during or after fluids to maintain MAP 65 or greater