Risk factors
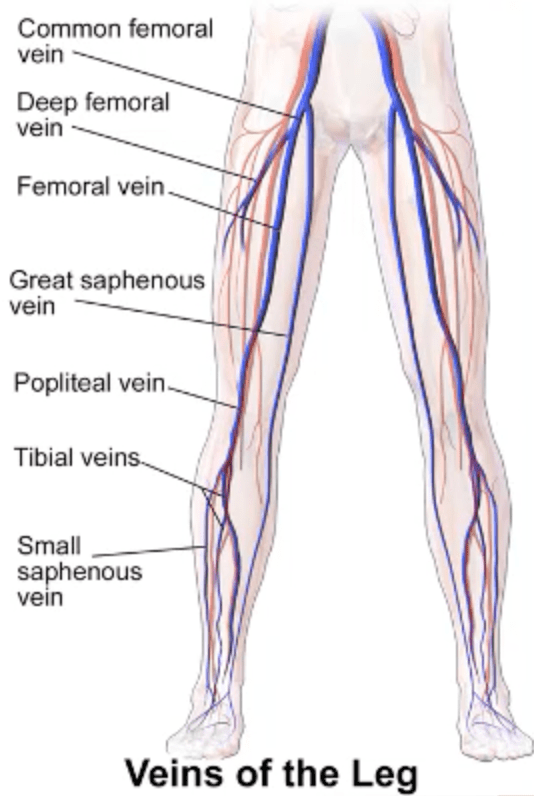
Anatomy
Pathophysiology
Evaluation/Diagnostics
Imaging Findings
Complications
Management/Heme
100
A person who sits for most of the day is at increased risk for DVT due to what part of Virchow triad?
What is venous stasis?
Stasis = slow flow → more time and opportunity for the coagulation cascade to generate a clot in the deep veins.
100
Most clinically significant pulmonary emboli arise from thrombi in which veins?
What are the proximal deep veins of the leg, especially the popliteal, femoral veins?
-DVTs are more likely to originate in calf veins, but PE-causing DVTs are much more likely to originate in the large proximal thigh veins
100
What property distinguishes an embolus from a thrombus?
What is a thrombus forms and remains attached at its site of origin, whereas an embolus breaks free and travels to another location.
100
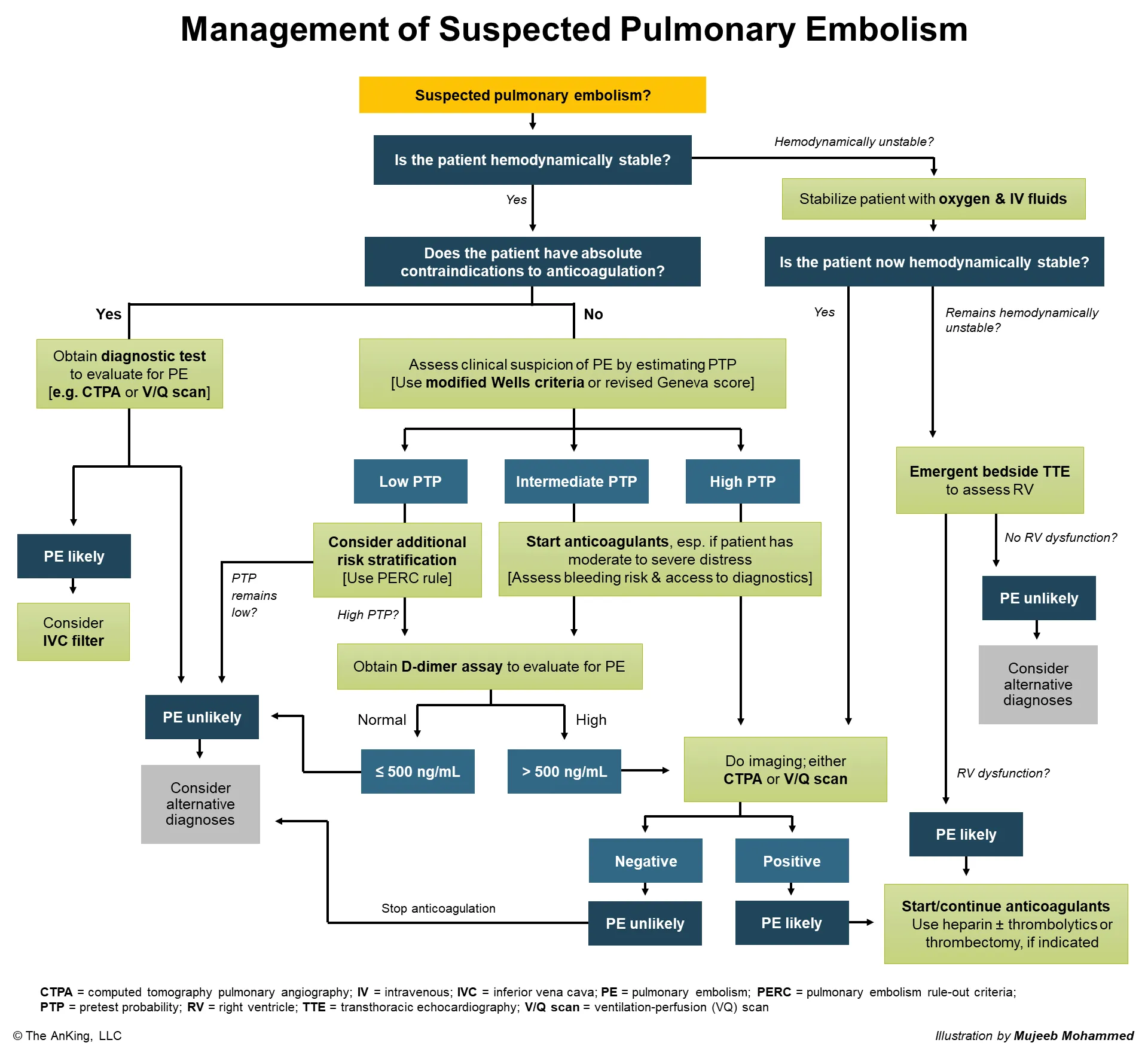
What is the diagnostic test of choice for pulmonary embolism?
What is CT pulmonary angiography (Directly visualizes filling defects (clots) in the pulmonary arteries)?
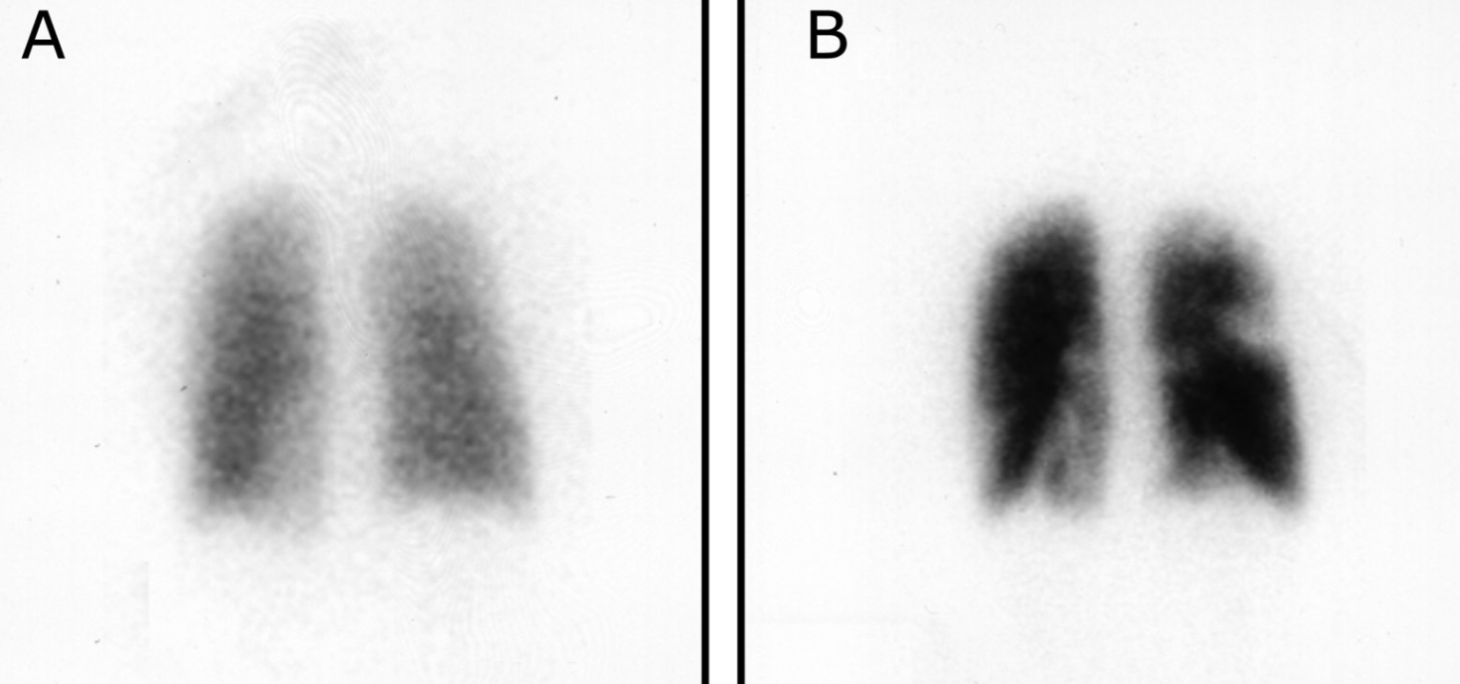
-V/Q scan in patients with renal insufficiency or contrast allergies or pregnant.
-Ventilation: shows where air goes in the lungs.
-Perfusion: shows where blood goes in the lungs.
100
On lower-extremity ultrasound, this finding indicates a deep vein thrombosis.
What is a noncompressible vein?
Solid thrombus is filling the vein and making it stiff.
Normally, a healthy vein is soft and collapses easily when you press with the ultrasound probe. In DVT, a clot forms inside the lumen → this clot physically blocks the space and supports the vein walls from the inside → when you press with the probe, the vein cannot fully collapse, so it appears partially or completely noncompressible on ultrasound
100
In a patient with pulmonary embolism who develops pulmonary infarction, explain what causes blood to appear in the sputum.
What is embolus blocks blood flow to a segment of lung → that area becomes ischemic and can undergo infarction → in the infarcted region, small pulmonary and bronchial blood vessels are damaged and may rupture → blood leaks into the alveoli and airways → when the patient coughs, this blood is brought up as blood‑tinged sputum (hemoptysis).
100
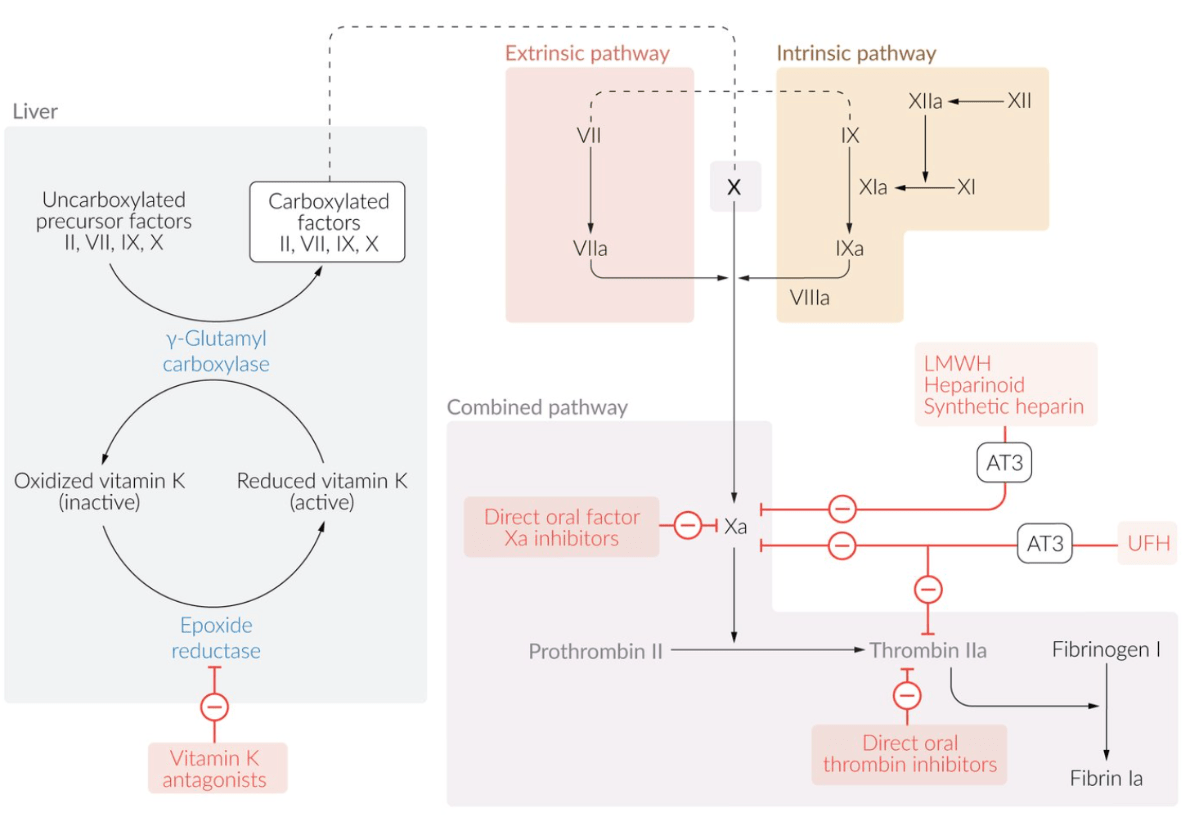
A patient was given oral apixaban for long-term therapy. What is the mechanism of action of this medication?
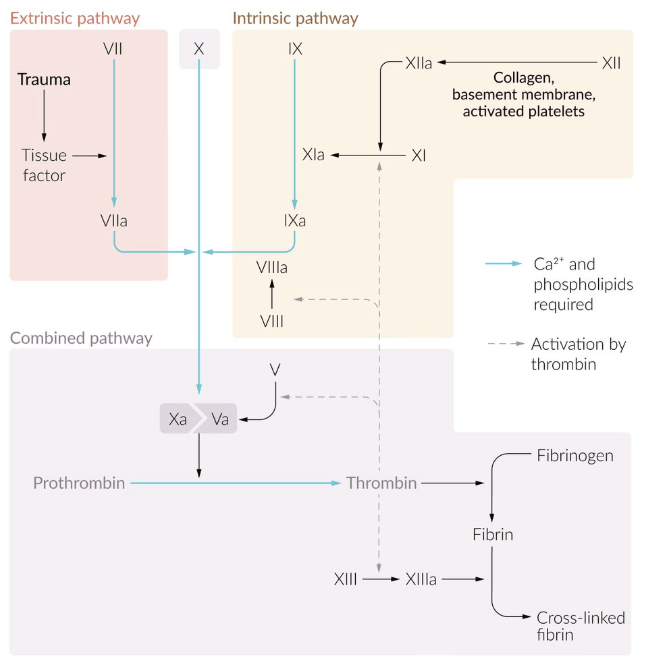
What is apixaban is a direct factor Xa inhibitor. It inhibits factor Xa, which decreases conversion of prothrombin to thrombin and therefore reduces fibrin clot formation.
200
A 64-year-old man with metastatic pancreatic cancer presents with recurrent, painful, migratory thrombophlebitis affecting different areas of his lower extremities over several weeks. Which mechanism best explains his increased risk of thrombosis?
What is Trousseau syndrome?
Malignancy (e.g., pancreatic adenocarcinoma) → tumor releases procoagulant factors and mucins → systemic hypercoagulable state → ↑ risk of migratory thrombophlebitis and DVT
200
A thrombus breaks off from the femoral vein. List the order of structures it travels through before reaching the pulmonary arteries.
What is femoral → external iliac → common iliac → IVC → R atrium → R ventricle → pulmonary arteries?
200
A bedridden patient develops a DVT. How does venous stasis mechanistically contribute to clot formation?
What is slow blood flow allows activated clotting factors to accumulate and promotes thrombus formation.
200
This highly sensitive blood test is commonly elevated in DVT and PE and is most useful to rule out disease in low-risk patients.
What is D-dimer? Sensitive but not specific. Can be useful when normal in setting of low-mod Wells score.
200
What is the preferred test for the initial evaluation of pulmonary embolus in a pregnant patient?
What is V/Q scan?
200
Recurrent small pulmonary emboli can cause this long-term complication by producing chronic obstruction and remodeling of the pulmonary vasculature.
What is pulmonary hypertension?
Recurrent small pulmonary emboli → chronic obstruction and endothelial injury → thickening, smooth muscle hypertrophy, and fibrosis of pulmonary arteries → lumen narrowing → increased pulmonary vascular resistance → pulmonary hypertension
200
A patient with acute DVT and severe renal failure requires anticoagulation. Which medication is preferred?
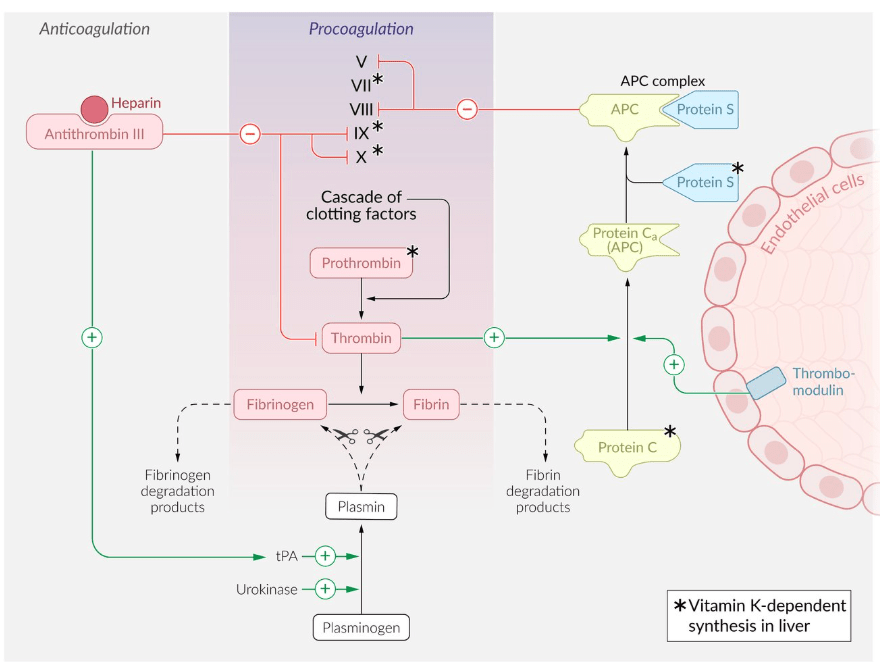
What is unfractionated heparin?
LMWH is renally cleared → accumulates → bleeding risk
300
A 34-year-old man develops a DVT after his flight and then has a stroke despite normal carotid imaging. Which congenital cardiac abnormality most likely allowed the thrombus to bypass the lungs and enter the systemic circulation?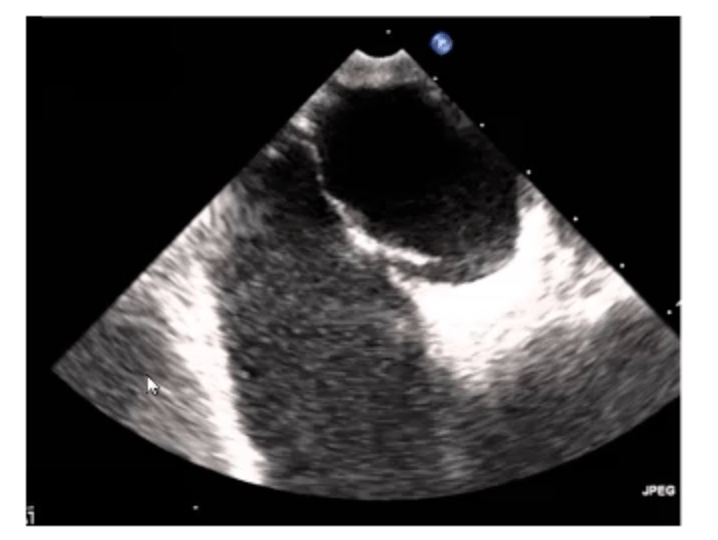
What is a patent foramen ovale causes paradoxical embolism?
(Arterial septal defect SD can also cause paradoxical embolism if pulmonary hypertension leads to Eisenmenger physiology with R-to-L shunting)
300
A 34-year-old man develops a DVT after a long flight and later has a stroke. What abnormal route did the thrombus most likely take to reach the brain? (Can start from the R atrium)
What is R atrium → across a R-to-L shunt (classically PFO) → L atrium → L ventricle → systemic circulation
-> brachiocephalic trunk → R common carotid → internal carotid → cerebral artery (anterior, middle, posterior) → stroke
OR
From the aortic arch → L common carotid → internal carotid → then up into a cerebral artery
300
A patient with PE has impaired gas exchange. Explain how mechanical vessel obstruction causes this abnormality.
What is the embolus blocks blood flow to part of the lung, so alveoli may still be ventilated but are not adequately perfused. This creates V/Q mismatch (V for airflow, Q for bloodflow). This also creates increased dead space (V/Q = infinity), meaning air reaches alveoli that are not participating effectively in gas exchange because little or no blood is available to pick up oxygen.
300
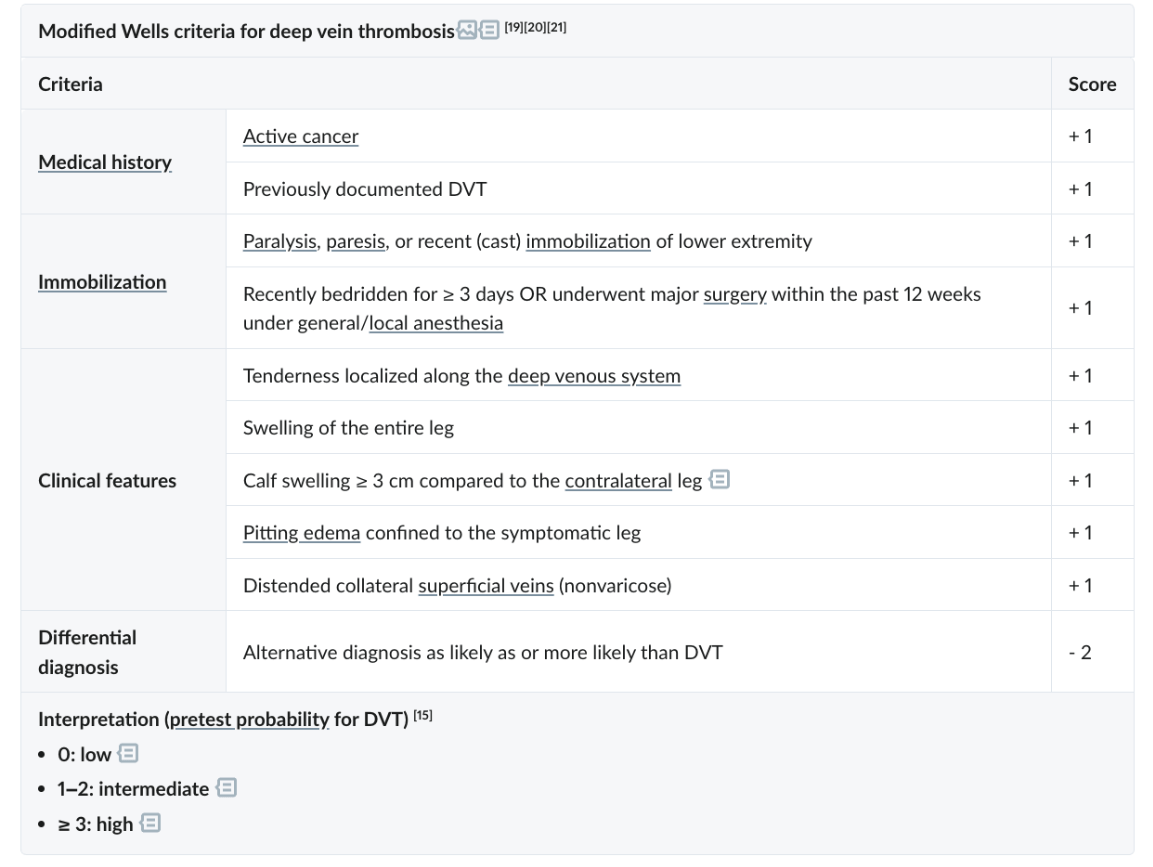
A patient presents with active cancer, calf swelling measuring 4 cm larger than the contralateral leg, and pitting edema confined to the symptomatic leg. There is no alternative diagnosis as likely as DVT. Using the modified Wells criteria table provided, calculate this patient’s Wells score and determine whether DVT is low, intermediate, or high probability.
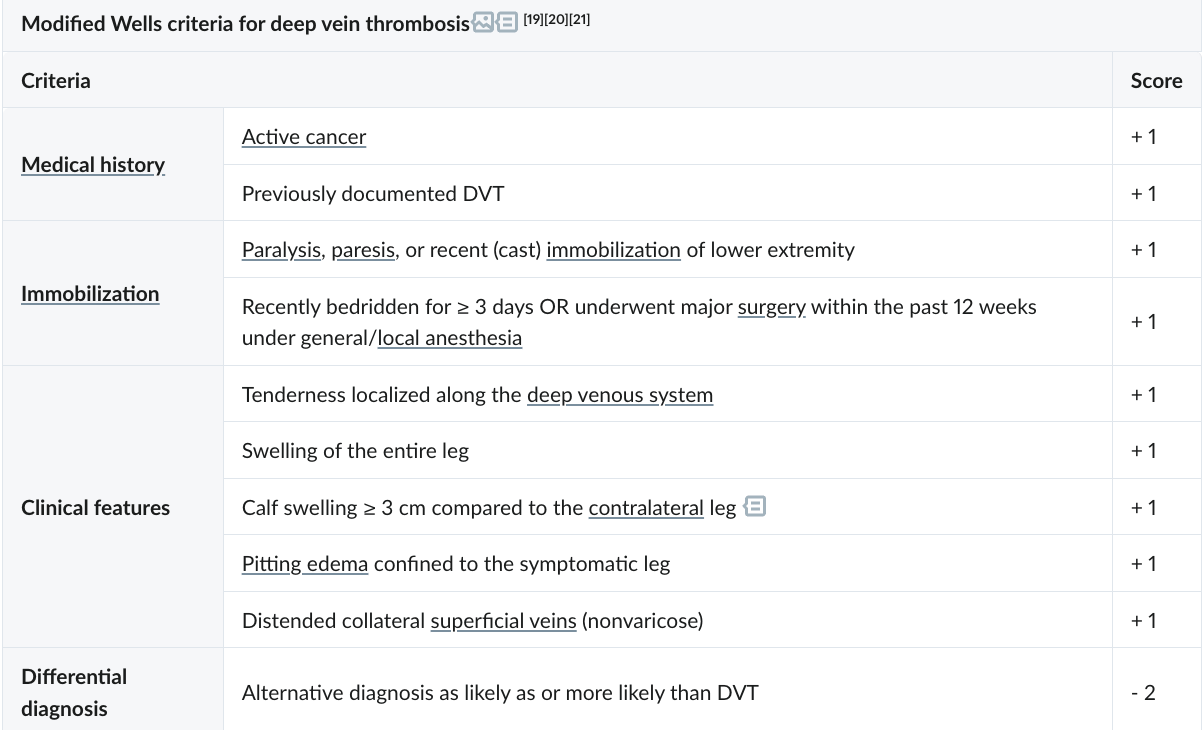
What is Wells score = 3; high probability of DVT?
300
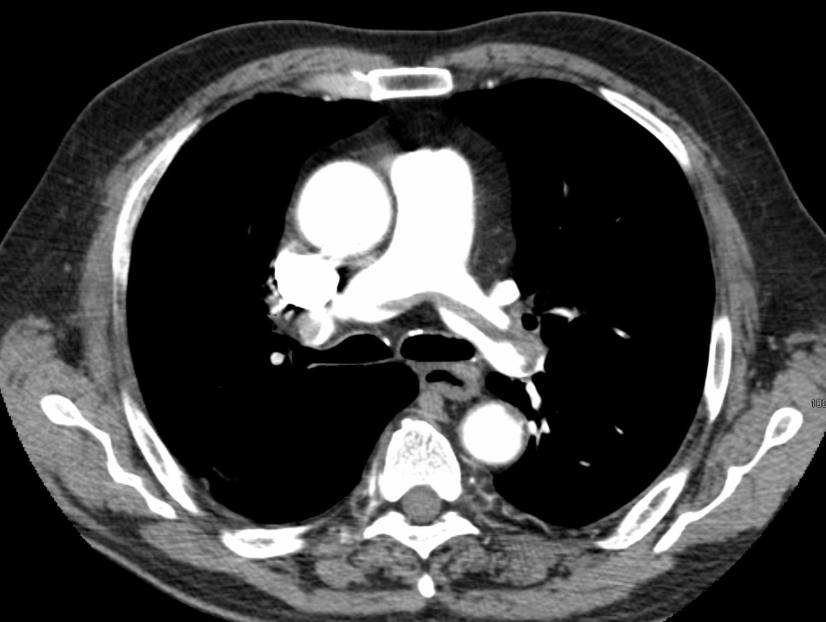
On CT angiography, a thrombus is seen extending into both the right and left pulmonary arteries from the pulmonary trunk. What type of pulmonary embolism is this?
What is a saddle PE?
300
This lower extremity shows hyperpigmentation, scaling, and edema due to chronic venous hypertension following prior deep vein thrombosis. What is the diagnosis?

What is chronic venous insufficiency/post-thrombotic syndrome/stasis dermatitis?
300
Deep venous thrombosis is treated with [...] to prevent thrombus propagation, [...] to bust the clot, and a(n) [...] for treatment-refractory patients/high-risk DVT patients
What are anticoagulant, thrombolytics, and IVC filter?
400
A young patient has recurrent unprovoked DVTs. Name 2 autosomal dominant inherited thrombophilias and briefly state their mechanism.
What are?
-Factor V Leiden → mutated factor V resistance to degradation by activated protein C
-Protein C or S deficiency → impaired inactivation of factors Va and VIIIa
-Antithrombin deficiency → decreased inhibition of thrombin and factor Xa
-Prothrombin G20210A → increased prothrombin levels
400
A thrombus forms in the axillary vein. List the major venous structures it passes through before reaching the R atrium.
What is Axillary vein → subclavian vein → brachiocephalic vein → superior vena cava → R atrium
400
A patient with massive PE develops hypotension even though the left ventricle itself is structurally normal. Why?
What is the embolus raises RV afterload, causing RV dilation and failure; this reduces blood reaching the left heart, decreases LV preload, and drops cardiac output.
400
A V/Q scan shows preserved ventilation with segmental perfusion defects in a patient with pulmonary embolism. How is the V/Q ratio affected in the involved lung regions?
What is V/Q ratio is increased because ventilation is present but perfusion is reduced?
- Ventilation scan (V): Shows how air is distributed throughout the lungs. The patient inhales a radioactive gas, and you see where the air goes.
- Perfusion scan (Q): Shows blood flow in the lungs. The patient is injected with radiolabeled particles in blood stream, and you see where blood is flowing in the pulmonary circulation.
400
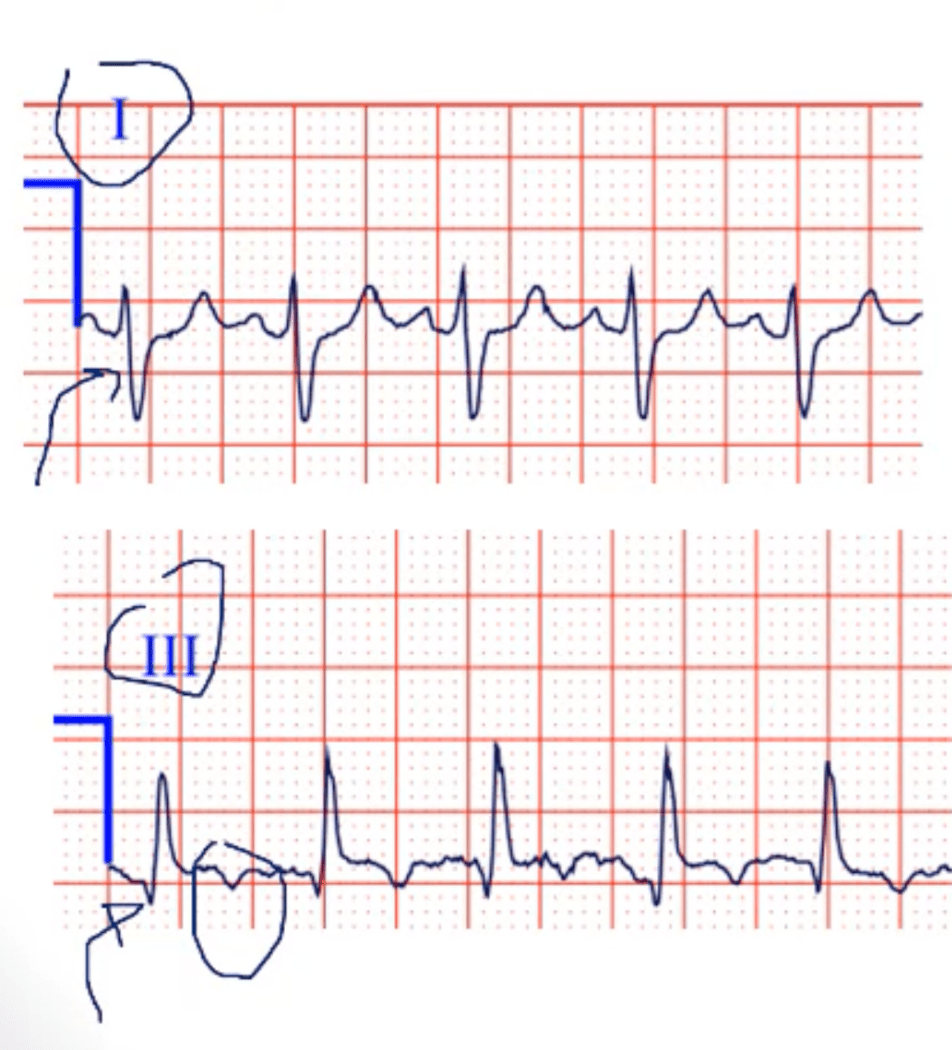
A 35-year-old woman presents to the emergency department with sudden-onset shortness of breath and sharp, pleuritic chest pain that worsens with inspiration. She recently underwent knee surgery and has been mostly bedridden for the past week. On examination, her respiratory rate is 28/min, heart rate is 110/min, and oxygen saturation is 90% on room air. Lung auscultation is clear bilaterally. ECG shows signs of acute right heart strain. Which of the following ECG findings is most characteristic of this patient’s condition?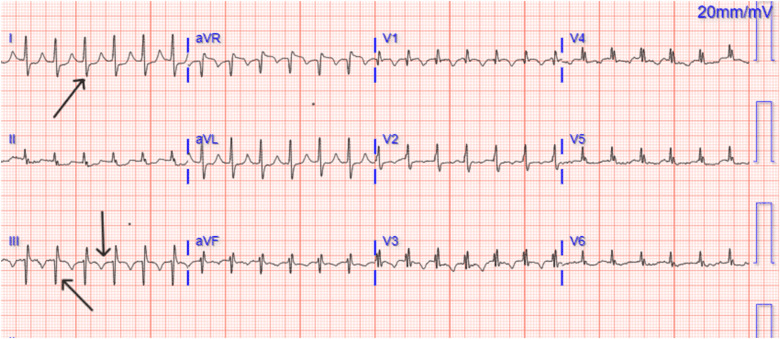
What is S1Q3T3 pattern?
-Deep S wave in lead I
-Q wave in lead 3 present
-Inverted T wave in lead 3
400
Explain the pathophysiology by which a large pulmonary embolism can lead to right-sided heart failure?
What is a large pulmonary embolism obstructs the pulmonary vasculature -> increases pulmonary vascular resistance and RV afterload. The right ventricle has to pump against this sudden pressure increase, so it dilates and fails, reducing blood flow to the L heart and causing hemodynamic instability.
400
A patient on apixaban for long-term anticoagulation presents with severe bleeding and requires urgent reversal. Which of the following is the most appropriate treatment?
What is andexanet alfa?
500
A postmenopausal woman on oral estrogen therapy develops a DVT. Name the coagulation factors increased by estrogen and the endogenous anticoagulants reduced or impaired by estrogen.
What are:
- ↑ factors II, VII, VIII, X, and fibrinogen (Factor I) → more clot formation
-↓ antithrombin → less inhibition of thrombin and factor Xa
-↓ protein S → weaker protein C/S anticoagulant activity
-↑ resistance to protein C → impaired inactivation of factors Va and VIIIa
500
A patient with a DVT develops a saddle pulmonary embolism. At what anatomic location is the embolus lodged?
What is the bifurcation of the main pulmonary trunk into the right and left pulmonary arteries?
500
A patient with a large pulmonary embolism develops acute right ventricular strain. In addition to mechanical obstruction by the clot, what vascular response further increases pulmonary vascular resistance?
What are vasoconstrictors (like thromboxane A2 and serotonin) secreted by activated platelet and the thrombus?
500
Early in an acute pulmonary embolism, patients often hyperventilate. Which of the following ABG findings best reflects this stage?
What is respiratory alkalosis with hypoxemia?
CO2 + H2O ⇌ H2CO3 ⇌ H+ + HCO3
- Low PaCO2
- High or high-normal pH
- PaO2 may be low or low-normal (mild hypoxemia) → there is a V/Q mismatch and some dead space, so oxygenation is impaired.
500
A chest X-ray shows a Hampton hump. What caused this finding, and why is this complication less likely to occur?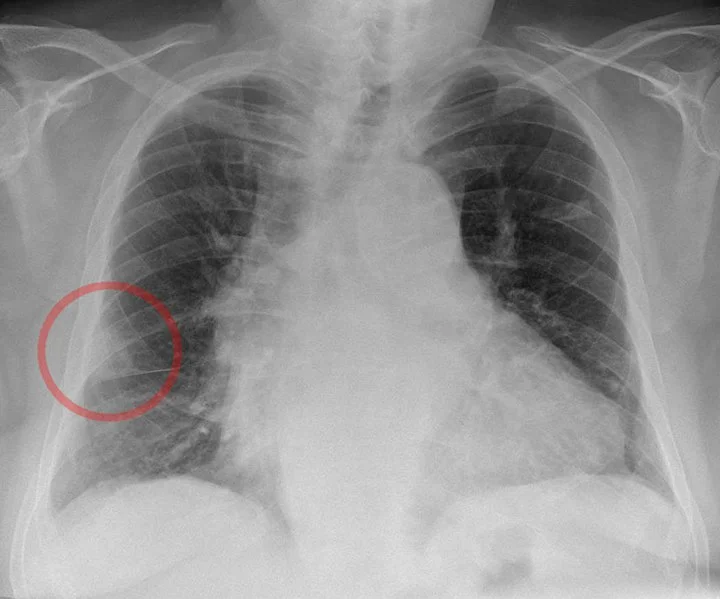
What is pulmonary infarction - pulmonary embolism obstructed pulmonary arterial blood flow
-Less common because bronchial circulation may protect against infarction.
500
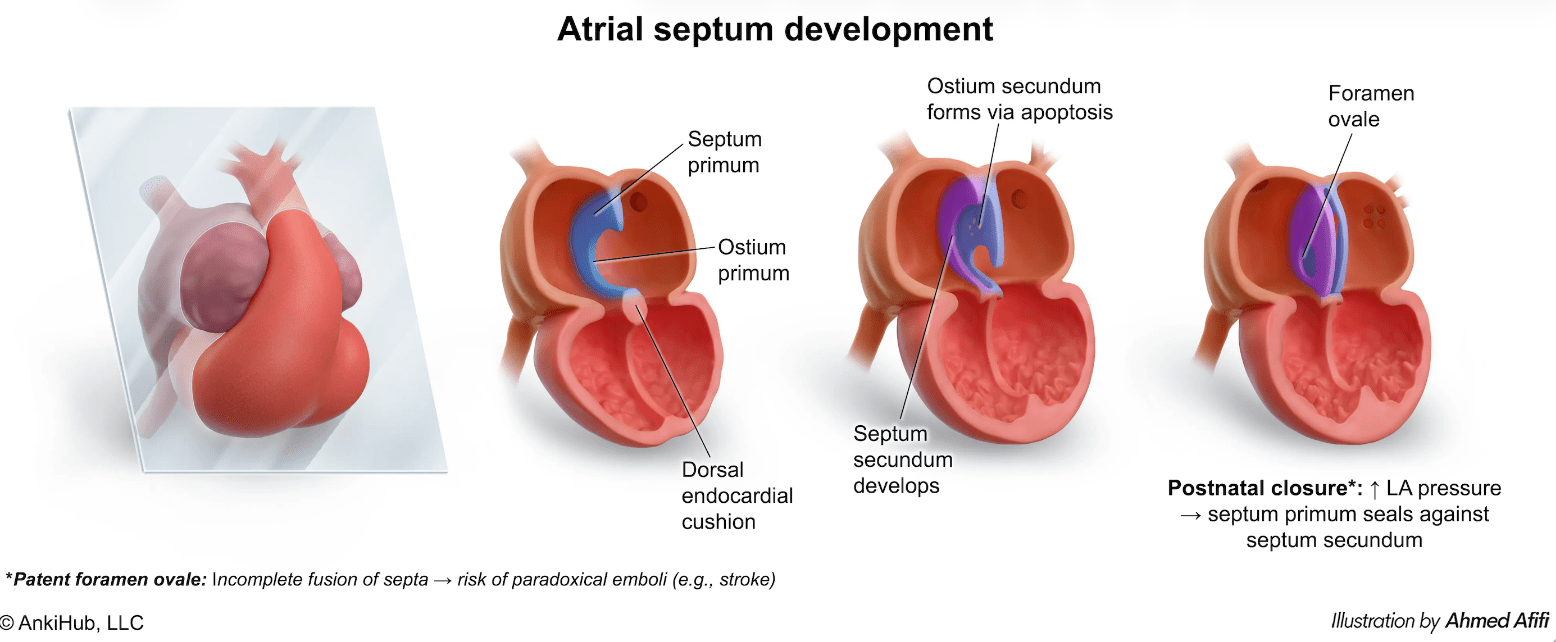
A patient with a DVT develops an embolic stroke, suggesting a paradoxical embolus. What went wrong embryologically to allow this defect to persist?
What is failure of the septum primum and septum secundum to fuse after birth?
500
A patient with a massive pulmonary embolism is crashing with hypotension and obstructive shock. Alteplase is given. What is the MOA by which this drug can rapidly improve the patient’s condition?
What is tPA turns plasminogen into plasmin, and plasmin cuts up fibrin → clot is broken down?