bug
transmission
treatment
STDs
All systems
100
26 y/o F comes to clinic after close contact with a child who have meningococcal meningitis. She takes Oral contraceptive pills and Daily multivitamin. Most appropriate next step?
Single dose of PO Ciprofloxacin
Rifampin two times a day for 2 days/Cipro single dose/Ceftriaxone single dose
Rifampin generally preferred ,but in this patient it interacts with OCPs and decreases their efficacy.
100
77 y/o M with cold develops fever,chills and cough over 24 hrs. H/o COPD, HTN,CKD and osteoarthritis. He used his albuterol inhaler more frequently during last few days due to SOB. he is also taking OTC cough suppressant with no relief. He is uptodate with his vaccines. Diagnosis and further treatment
Flu, Admission
100
Treatment of Syphilis in a penicillin allergic patient in Pregnancy
Penicillin Desensitization
100
Thin, greenish yellow, frothy vaginal discharge. Diagnosis and treatment
Trichomoniasis, Metronidazole
100
Patient started on IV Labetalol and Nitroprusside infusion for BP of 230/112, dissection of descending aorta, found to be confused,agitated,having GTCS. Most likely diagnosis
Cyanide toxicity because of nitroprusside
Flushing, AMS, seizures,coma, arrhythmias, metabolic acidosis
Treatment: Cessation of nitroprusside and administration of Sodium Thiosulfate
200
19 y/o comes with abdominal discomfort,diarrhea and nausea after a trip from Guatemala. Vitals normal, Labs normal except eosinophilia, Fecal occult blood. She doesn't take any medication.Next step?
Albendazole
intestinal helminths-eosinophilia characteristic
Metronidazole for Giardiasis, Entamoeba
200
25 y/o medical interpreter at a regional hospital found to have Tuberculin test positive with 12 mm induration at 48 hrs. CXR done showed no abnormality. Next step?
Latent TB-start treatment with INH for 6-9 months,Rifampin for 4 months, INH and Rifapentine weekly for 3 months under supervision
She is non-infectious and can go to work
200
64 Y/o F with h/o Myasthenia gravis, comes with neck stiffness, fever and headache.12 days ago treated for UTI. Labs: WBC: 13,000,CSF: opening pressure-300 mm H2O, Glucose-30 mg/dl, Protein- 180 mg/dl, WBC 2,500 with 90%neutrophils, RBC 5,CSF gram stain and culture showed no organisms, cryptococcal Ag negative, CT head with contrast negative. Most likely cause of patient's symptoms
Bacterial Meningitis
Sensitivity of CSF gram stain varies from 60-90%, yield of both gram stain and culture reduced by prior antibiotic use.
200
Man with multiple sexual partners, develops fever, maculopapular rash all over the body, tender lymphadenopathy,tender ulcers with white exudates on oropharynx, Lab showed WBC 1,600/mm3, Platelets 120,000/mm3. All symptoms started 3 days back. Most likely diagnosis?
Acute HIV infection
Acute retroviral syndrome due to recently acquired HIV infection.Symptoms resemble infectious mononucleosis, diagnosis with HIV ag+HIV 1/2 ab+HIV viral load. Treatment with Antiretrovirals
200
Sudden cardiac death in an young adult on exertion with no family history of CAD or sudden death
Anomalous coronary artery
300
Got a cut while cleaning a tropical fish tank, followed by hemorrhagic bullae surrounding laceration
Vibrio vulnificus
300
60 y/o underwent bonemarrow transplantation 1 month ago for aplastc anemia presented with productive cough,pleuritic chest pain, hemoptysis. CXR showed cavitary lesion in left upper lobe with ground glass opacities. Diagnosis, Treatment?
Aspergillosis, IV Voriconazole and reduction of immunosuppressive agents.
300
Advanced HIV,TB .Was started on treatment for active pulmonary TB and HIV . 6 weeks later developed recurrent fever, cough , worsened pulmonary infiltrates. Diagnosis and treatment
IRIS-immune reconstitution inflammatory syndrome
No change in Anti-TB or anti retroviral. Treatment symptomatic. NSAIDS or short course steroids can be used in those with bothersome .
300
35 y/o came with concern about his HIV status. He had a new sexual partner and found out to be HIV positive. Initial P24,HIV 1/2 Ab negative a month ago. What is the best next step?
Repeat P24,HIV1/2.
Although there is high sensitivity and specificity for these tests ,Ag and Ab titers are too low to detect initially during 1-4 weeks (window period)
300
Nurse had a needle stick, h/o Hepatitis B vaccination with low titers now. patient labs below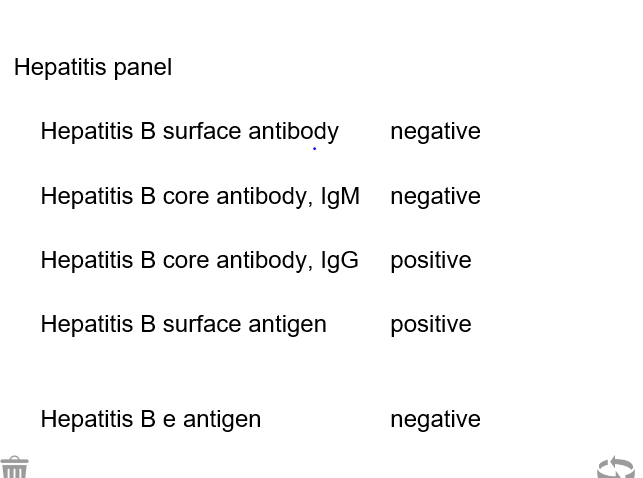
Hepatitis immunoglobulin and revaccination
400
56 y/o F undergoing chemotherapy presents with fever, rash. She developed a rash on her right thigh which within hours changed to pustule,formed a bulla, ruptured and formed an ulcer. similar rash occurred on left leg. O/E CVL appears clean with no erythema.Labs showed WBC count 800/mm3 with 10%neutrophils. Most likely diagnosis, causative organism?
Ecthyma gangrenosum , by Psudomonas
Patient with CVL, Chemotherapy induced neutropenia developed rapidly progressive, ulcerative skin lesions suggesting Echtyma gangrenosum.
400
49 y/o comes from a trip to India and develops rash, fever,joint pains, he got appropriate vaccinations before the travel and used bottled water throughout his stay. While checking Blood pressure, insufflation of cuff reveals petechial rash. Labs showed thrombocytopenia. Diagnosis and most common complication?
Dengue fever and Circulatory collapse-Dengue shock syndrome
400
25 y/o s/p Deviated nasal septum repair 2 days back comes to ER with high grade fever 103F, chills, myalgias, skin rash ,nausea and 3 episodes of profuse watery diarrhea and lightheadedness. O/E nasal packing on both nostrils, diffuse ,red, macular rash involving palms and soles. Diagnosis and pathogenesis
TSS-Toxic shock syndrome by Staph aureus, Exotoxin production
widespread activation of T cells by exotoxins leading to shock
400
20 y/o with 2 sexual partners in last 3 months presents with fever, pustular rash and pain in right wrist, left wrist and fingers. No effusion. What test yields the best result?
PCR of urogenital tract secretions for Gonorrhea
Disseminated gonococcal infection with dermatitis, tenosynovitis and polyarthralgia
400
Hepatitis B positive, develops pain in hands and knees 3 weeks ago, followed by rash which started initially on abdomen then extended to whole body associated with fever, abdominal pain started 24 hrs back-What kind of immune reaction/pathophysiological mechanism, what other agents cause same reaction
Serum Sickness like reaction type III Hypersensitivity-Ag+Ab+Complement
Fever, polyarthriris, dermatitis in Hep B infection
Beta lactams, Sulfa, Acute Hep B, mmune complex formation
500
19 y/o college student comes with 2 days of burning urination, urethral meatal itching after he has a new sexual partner a week ago. He denies urethral discharge,fever. O/E scanty, watery urethra discharge present. Causative organism and treatment?
Chlamydia (non-gonococcal urethritis) and Azithromycin
500
30 y/o with a past history of Diabetes type 1 admitted to hospital with DKA. Vitals temp :102F,BP 130/80,PR 110/min, mild periorbital swelling present. Right sided bloody, purulent nasal discharge and black eschar on inferior nasal turbinate. Diagnosis and treatment?
Mucormycosis, Amphoterecin B
500
26 y/o M with c/o headache,malaise, myalgia,gradually enlarging rash, recently returned from a 2 week camping and hiking trip to Eastern Pennsylvania. temp 100.4F,HR,RR,BP within normal limits.O/E: 4 cm oval ,uniformly red macular patch at the belt line. What's the treatment.
Oral Doxycycline
Lyme disease-Early localized Lyme disease
500
21 y/o F,college student presents with fever, myalgia, abdominal pain, weigh loss. She is sexually active and uses condoms inconsistently. O/E: Pharyngitis,Lymphadenopathy, Hepatosplenomegaly present. Diagnosis, you ask her to avoid?
Infectious mononucleosis, Suggest to avoid sports for at least 3 weeks and contact sports for 4 weeks to prevent splenic rupture
Monospot test or heterophile antibody test,
500
2 month old baby born to IV drug user who had Acute Hep B in third trimester received Ig and vaccine at birth, most appropriate next step in infant's care
Administer vaccine
Ig and Vaccine within 12 hrs after birth, routine vaccination ,serology testing after 3 rd dose of vaccine.