Smörgås-BOARD
Rheum with A View
Liv-er Let Die
Heme-agen Dragons
Final Jeopardy
100
This is the first line treatment for a patient presenting with erythmatous rash that has been progressively enlarging since they returned from a camping trip in Massachusetts two weeks ago, having the following appearance:

What is doxycycline?
Key Point:
This patient has an enlarging erythematous skin lesion with central clearing suggestive of erythema migrans and should be prescribed doxycycline. Erythema migrans is the most common presentation of Lyme disease, seen in up to 80% of patients, although an initial heterogenous patch of erythroderma is more common than the classic target-like appearance.
Early localized Lyme disease and southern tick–associated rash illness present with erythema migrans and are clinically indistinguishable; therefore, patients with erythema migrans should be treated with doxycycline, which is effective in both conditions.
100
The most likely diagnosis for a 40 year old woman with pain, tenderness and swelling of the small joints of the hand and foot. It is accompanied by patches of erythema and scaling behind the ear and at the oc ciput of the scalp.
ciput of the scalp.
Changes of the nail are seen below:
What is psoriatic arthritis?
Key Point
Psoriatic arthritis is associated with psoriasis, enthesitis, dactylitis, tenosynovitis, arthritis of the distal interphalangeal joints, asymmetric oligoarthritis, and spondylitis.
Nails should be examined for pitting or onycholysis.
The recently developed Classification Criteria for Psoriatic Arthritis (CASPAR) have a sensitivity and specificity of more than 90%, especially for the diagnosis of early psoriatic arthritis.
100
According to the American Association for the Study of Liver Disease, this disorder is projected to become the leading cause of liver cirrhosis/transplantation in the US by 2030.
What is NASH/NAFLD?
Key Point:
NAFLD is the most common cause of abnormal liver test results in the United States. Approximately 30% of the U.S. population has NAFLD, some of whom have normal liver enzyme levels. Most patients with NAFLD have insulin resistance associated with obesity, hypertriglyceridemia, and/or type 2 diabetes mellitus. Approximately 20% of patients with NAFLD have nonalcoholic steatohepatitis (NASH), which is characterized by hepatic steatosis accompanied by inflammation and often fibrosis.
100
The underlying disorder for this case presentation:
61 year old man presents with transient visual disturbances, hypertension, erythromelalgia, aquagenic pruritus. On exam patient is found to have facial plethora and splenomegaly. Labs show +JAK2 mutation.
What is Polycythemia Vera (PV)?
PV is a myeloproliferative disorder due to clonal rbc proliferation that is EPO-independent. Most patients have a low EPO level and +JAK2 mutation testing. Patients at low risk for thrombosis (<60y/o, no prior thrombosis) are treated with serial phlebotomy, low-dose aspirin, and symptom control. Those at greater thrombus risk or active thrombus also require myelosuppression.
100
According to the STITCHES trial, in addition to optimal medical therapy, this would be the preferred treatment for a symptomatic patient unable to walk two blocks due to SOB, with an ECHO showing LVEF 30% and anterior wall akinesis, the following EKG, and a cardiac cath showing 90% stenosis of LAD, 70% stenosis of circumflex artery, and 20% stenosis of RCA.
What is coronary artery bypass graft (CABG)?
Key point:
Coronary artery bypass graft (CABG) surgery is the most appropriate treatment for this patient with heart failure with reduced ejection fraction and electrocardiographic findings compatible with ischemic cardiomyopathy. As demonstrated in the recent STICHES trial, surgical coronary revascularization for ischemic cardiomyopathy, in combination with medical therapy, provides durable benefits compared with medical therapy alone. STITCHES shows a significantly reduced 10-year rate of all-cause death than those treated with medical therapy alone.
200
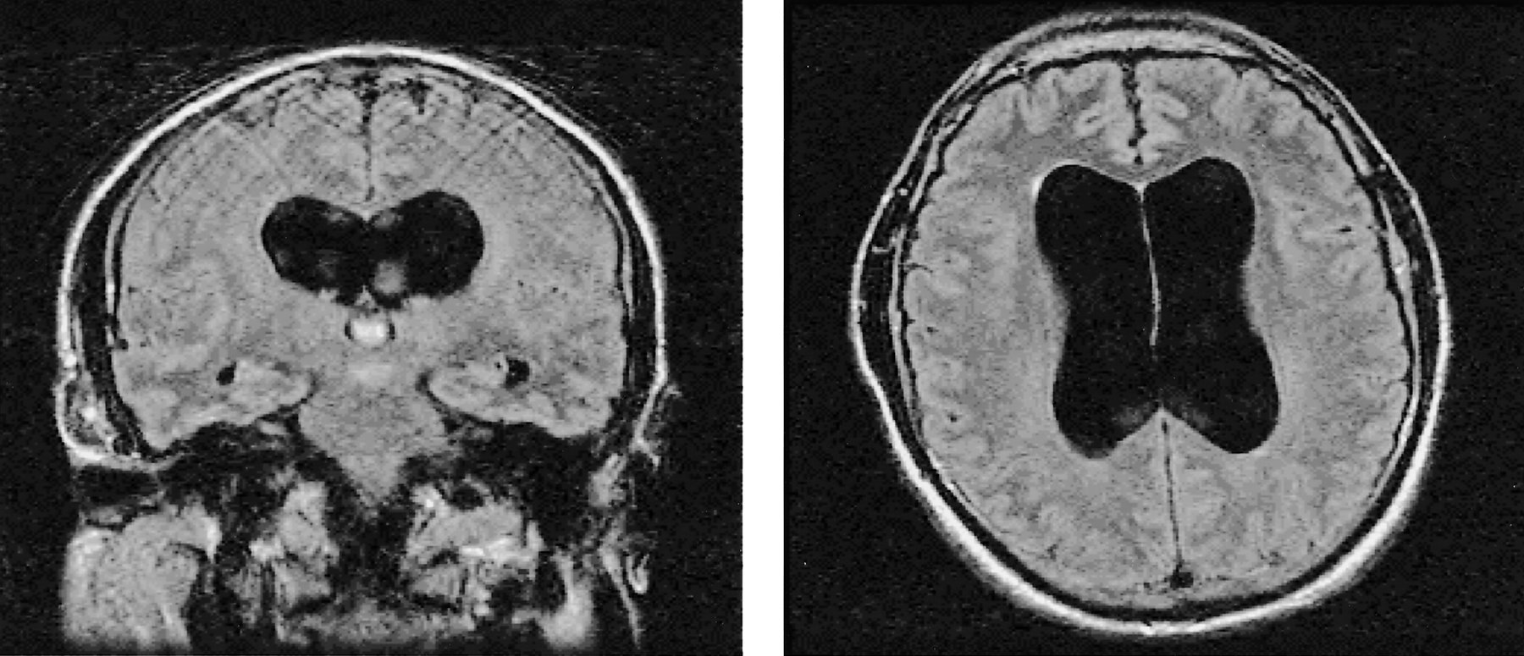 This is the indicated treatment for a patient having memory and concentration difficulties; urinary urgency, frequency and incontinence; a wide, slow, shuffling gait; and the following CT brain findings:
This is the indicated treatment for a patient having memory and concentration difficulties; urinary urgency, frequency and incontinence; a wide, slow, shuffling gait; and the following CT brain findings:
What is large-volume lumbar puncture?
Large-volume lumbar puncture is indicated in this patient with likely normal pressure hydrocephalus (NPH). NPH is the most likely diagnosis in the setting of the triad of gait abnormalities, cognitive impairment, and urinary disturbance, especially when neuroimaging studies show enlarged ventricles out of proportion to cortical atrophy. NPH is a potentially reversible cause of cognitive and motor decline.
200
This should be the first test ordered in a 40 year old man with history of well controlled chronic plaque psoriasis who suddenly develops painful joints and  worsening psioratic plaques of the trunk and extremities as picture below:
worsening psioratic plaques of the trunk and extremities as picture below:
What is HIV antibody testing?
Key Point
The development of explosive onset or severe flare of psoriatic arthritis should raise suspicion for concomitant HIV infection.
200
The most likely diagnosis in a 58 year old women with hx of hypercholesterolemia presenting progressive fatigue and generalized pruritis without rash.
Labs show:
ALT 75
AST 54
ALK 328
Tbili 1.2
Dbili 0,6
Antimitochondrial Ab 1:640
Normal RUQ US.
What is primary biliary cirrhosis?
Primary biliary cirrhosis (PBC), now termed “primary biliary cholangitis”, is a chronic cholestatic liver disease of unknown cause. PBC mainly affects middle-aged women. Most patients are asymptomatic at presentation but develop symptoms of PBC within 10 years; symptoms include fatigue, dry eyes, dry mouth, and pruritus. Hyperlipidemia is common, but jaundice, cutaneous hyperpigmentation, hepatosplenomegaly, and xanthelasmas are rarely observed at diagnosis. PBC is diagnosed by serum alkaline phosphatase levels greater than 1.5 times the upper limit of normal and typically normal serum total bilirubin levels. Serum aspartate (AST) and alanine (ALT) aminotransferase levels are typically less than five times the upper limit of normal. Serum antimitochondrial antibody is present in 90% to 95% of patients. For patients with undetectable serum antimitochondrial antibody levels, a liver biopsy is required for diagnosis. Treatment with ursodiol slows disease progression and may prevent or delay advanced disease and the need for liver transplantation.
200
This is the standard long-term treatment to prevent recurrent thromboembolism in cancer patient.
What is Enoxaparin?
Low molecular weight heparin (LMWH), e.g. enoxaparin, is more effective than vitamin K antagonists (e.g. warfarin) in reducing the risk of recurrent venous thromboembolism in cancer patients. However, LMWH is not associated with improved survival in these patients.
300
The most appropriate treatment for a liver transplant patient treated with mycophenolate mofetil and prednisone, who as developed painful swallowing and the following EGD findings:
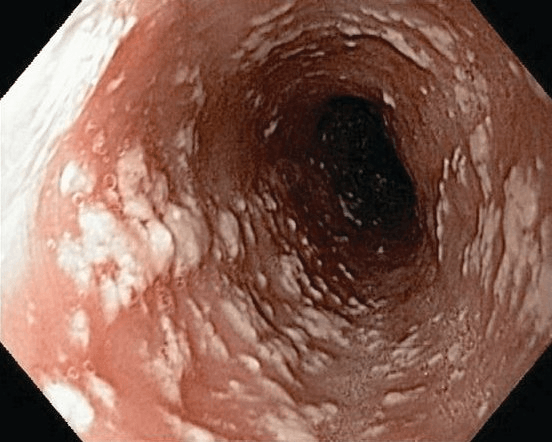
What is fluconazole?
Key Points:
This patient has a clinical presentation and findings characteristic of Candida albicans esophagitis. Infectious esophagitis can be caused by bacterial (uncommon), fungal, viral, and parasitic pathogens. Fluconazole is the first-line therapy for Candida esophagitis and is a more effective therapy than swallowed nystatin.
300
The most likely diagnosis in a 44 year old male who has color change in the hands when exposed to the cold, finger skin tightness with palpable nodules, fatigue, and pruritus.
His physical exam shows skin thickening of the face and finger. There are a few firm, gritty nodules on the palmar aspect of the digits. There is no rash or digital pits.
There are no telangectasias or esophageal dysmotility present.

What is limited cutaneous systemic sclerosis?
Key Point:
Limited cutaneous systemic sclerosis is characterized by distal skin thickening (face, neck, and hands) and is typically not accompanied by internal organ fibrosis; patients may display features of the CREST (calcinosis cutis, Raynaud phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasia) syndrome.
300
The most likely diagnosis of an 18 year old woman hospitalized with confusion and jaundice after taking tylenol.
Her labs show: hgb 9, reticulocyte 9%, INR 1.7, ALT 239, AST 243, Alk 34, T bili 8.4 and D bili 2.6.
Drug screen positive for acetominophen.
Physical exam notes asterixis and palpable spleen, and the picture eye exam: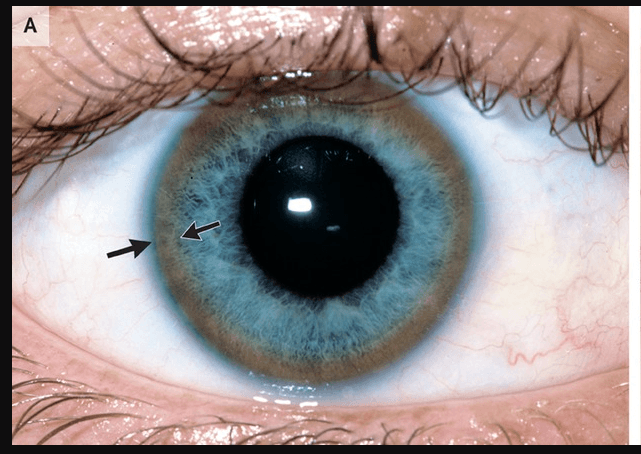
What is Wilson's Disease?
Wilson disease is a rare congenital disorder of copper excretion that occurs in approximately 1 in 30,000 live births. Young patients with Wilson disease tend to present with acute liver failure; older patients present with chronic liver disease and/or neurologic manifestations. Wilson disease should be considered in all patients younger than 40 years of age who have unexplained liver disease.
When Wilson disease causes acute hepatitis, usually in young patients, the sudden release of copper from liver cells can also induce hemolytic anemia.
Kayser-Fleischer rings, noted on ophthalmologic examination, indicate copper deposition in the Descemet membrane of the iris. Patients with acute liver failure due to Wilson disease rarely recover and should be urgently referred for liver transplantation.
300
The underlying disorder for the following case presentation:
23 year old African American man presents with jaundice, dark urine, and fatigue. Was seen in clinic 4 days ago and prescribed trimethoprim-sulfamethoxazole. Peripheral blood smear shows bite cells. Direct and indirect Coombs' test are negative. Red blood cell glucose-6-phosphate dehydrogenase level is normal.
What is Glucose-6-Phosphate Dehydrogenase Deficiency?
Onset of acute hemolysis after treatment with TMP-SMX, negative direct and indirect anti-globulin (Coombs') test, and the presence of "bite cells" on peripheral smear is consistent with a diagnosis of Glucose-6-Phosphate Dehydrogenase (G6PD) Deficiency. It is a x-linked disorder, commonly induced by oxidative stress via medications (e.g. dapsone, antimalarials, sulfonamide antibiotics), ingestion of fresh fava beans, infections, metabolic abnormalities (e.g. DKA). Typically presents 2-4 days after an oxidatively stressful event with evidence of hemolysis. Testing for G6PD deficiency during an acute hemolytic episode may produce a false negative result as the older and more deficient erythrocytes are destroyed and replaced by reticulocytes that commonly have normal G6PD levels. If a false negative is suspected, it is recommended to recheck the G6PD level 2-3 months after the hemolytic episode.
400
This is the indicated management for a post surgical aortic valve replacement patient who developed exertional dyspnea, fatigue, lower extremity edema and findings of JVD with y descents, CVP of 12cm H2O, pericardial knock, and Doppler of hepatic veins consistent with constrictive pericarditis.
What is Ibuprofen (NSAIDS)?
Key Point
"In some patients with constrictive pericarditis, the constriction may be transient and either spontaneously resolve or respond to medical therapy, which obviates the need for surgical pericardiectomy."
400
This is the most appropriate treatment for a 24 year old woman with tender nodules over the legs, stiffness of ankles, and productive cough. Her labs show ESR of 38mm/hr, HCT of 35% and normal WBC and platelet counts.
Joint xrays show no bony erosions.
Chest xray appears as this:

What are NSAIDS?
Key Point:
This patient has Löfgren syndrome, a self-limiting form of sarcoidosis characterized by a triad of acute arthritis in combination with bilateral hilar lymphadenopathy and erythema nodosum. The “arthritis” associated with Löfgren syndrome is actually a nondestructive periarthritis of the soft tissue, entheses, and tenosynovium around the joints.
When the triad of features occurs, it has a 95% specificity for diagnosis, and further diagnostic tests (such as radiography or serologic testing) are unnecessary.
Ninety percent of patients remit within 12 months.
400
These two are the most appropriate treatments for a 56 year old woman hospitalized with confusion who has a hx of decompensated hepatitis B cirrhosis and chronic ascites.
Physical exam shows disorientation to time and date, asterixis and moderately distended abdomen with ascites.
Labs show T bili 2.8, Cr 1/3, BUN 34.
Paracentesis shows 640 PMN cells.
What are 3rd gen cephalosporin (e.g. cefotaxime) and albumin?
Key point:
This patient has been hospitalized with overt hepatic encephalopathy, which in many instances may be the sole presenting feature of spontaneous bacterial peritonitis (SBP). It is important to perform a diagnostic paracentesis in patients with ascites who are admitted to the hospital, especially those with overt hepatic encephalopathy. Ascitic fluid analysis with PMN >250 is diagnostic of SBP.
Patients with a serum creatinine level greater than 1 mg/dL (88.4 µmol/L), a serum bilirubin level greater than 4 mg/dL (68.4 µmol/L), or a blood urea nitrogen level greater than 30 mg/dL (10.7 mmol/L) should receive 1.5 g/kg of intravenous albumin (25%) on the day of diagnosis and 1 g/kg of albumin on day 3; this practice has demonstrated a survival benefit.
400
22 year old hospitalized woman is evaluated for confusion, thrombocytopenia (12,000 platelets), microangiopathic hemolytic anemia with schistocytes and mild renal insufficiency. Direct Coombs test is negative, peripheral blood smear shows decreased platelets, polychromatophilic red blood cells, and multiple schistocytes with no platelet clumping.
What is Thrombotic Thrombocytopenic Purpura (TTP)?
TTP is characterized by the formation of small-vessel, platelet-rich thrombi due to severe deficiency of the vonWillebrand factor-cleaving protein ADAMTS13. TTP can be associated with pregnancy due to the formation of autoantibodies (acquired) or the emergence of a previously unknown heredity case. Patients with TTP can be minimally symptomatic or critically ill but classically have: Severe thrombocytopenia ~10,000 platelet count, Microangiopathic hemolytic anemia (MAHA) - schistocytes on peripheral blood smear, organ dysfunction (thrombi-indued ischemia can lead to neurologic manifestations and mild renal insufficiency. Diagnostic studies will reveal normal coagulation studies negative Coombs testing, and ADAMTS13 levels of <10%. Urgent treatment with plasma exchange, glucocorticoids, and rituximab are required to prevent death
500
This is the diagnostic test of choice for a 52 year old male hospitalized with several episodes of hemoptysis, fever, right hand weakness, labs showing Creatinine 2.1 and urinalysis with 3+ protein; 50 erythrocytes/hpf; 20 leukocytes/hpf; several mixed cellular casts, a sinus xray showing bony erosion of septum and turbinates, and a cxr showing diffuse infiltrates.
What is Antiproteinase 3 antibody levels?
Key Point:
This patient most likely has granulomatosis with polyangiitis (formerly known as Wegener granulomatosis), a systemic necrotizing vasculitis that predominantly affects the upper and lower respiratory tract and kidneys.
Patients may present with:
upper airway manifestations such as sinusitis or nasal, inner ear, or laryngotracheal inflammation
skin manifestations such as purpura and ulcers
Mononeuritis multiplex
Anti-PR3 antibodies is sufficient to establish a diagnosis in patients with classic upper airway manifestations, pulmonary infiltrates/nodules, and urinary abnormalities consistent with glomerulonephritis.
500
The is the underlying disorder of a 46 year old woman who has a summer time rash and noted physical findings of eyelid swelling and a periorbital violaceous rash, erythema and poikiloderma of the anterior chest and upper back, and an erythematous papular rash on the hands picture below; Muscle strength and reflexes are normal.
Labs show:
Normal CBC and Chem Panel
Creatinine kinase 100
ANA titre 1:640

What is amyopathic dermatomyositis?
Key Point:
Amyopathic dermatomyositis refers to dermatomyositis with cutaneous involvement in the absence of clinical, laboratory, electromyogram, or biopsy evidence of myositis.
500
This typical treatment for pulmonary hypertension should be avoided in patients with PAH who present with hx of liver cirrhosis and have portal hypertension.
What are calcium channel blockers?
Key points:
Portopulmonary hypertension is a Group 1 PAH that occurs in present of CLD with portal HTN. It has poor vasoactive response and can cause hypotension with splanchnic vasodilation.
Preferred medical treatments are prostacyclin analogues (epoprostenol), endothelin antagonists (bosenten), or phosphodiesterase inhibitors (sildenafil).
Other treatments to avoid:
Beta blockade
TIPS
500
The preferred treatment for a patient 6 weeks post NSTEMI, who develops a sudden drop in platelet count from 210,000/µL to 62,000/µL while receiving enoxaparin DVT prophylaxis on the sixth day of subsequent hospitalization for acute CHF exacerbation.
What is Argatroban/direct thrombin inhibitors?
Heparin-induced thrombocytopenia (HIT) should be suspected in patients treated (or recently treated) with heparin who develop unexplained thrombocytopenia (or a > 50% decrease in platelet count from baseline) or newly diagnosed thrombosis (venous or arterial). Once HIT is suspected, all forms of heparin must be stopped immediately, laboratory testing for HIT should be obtained, and alternate anticoagulants (eg, direct thrombin inhibitors; e.g. Argatroban) should be started even if thrombosis has not occurred.