A
B
C
D
E
100
c-ANCA/PR3-ANCA is most commonly associated with this disease of small vessels
Wegners or granulomatosis with polyangiitis
100
describe the heart sound/murmur that would be associated with the abnormality shown below
mid-systolic click (with possible late systolic murmur)
100
a patient presents with c/o a small, painful bump under the proximal portion of his fingernail. Biopsy reveals hyperplasia of smooth muscle cells that help with regulating A-V shunts and temperature control of the digits. Should the patient be concerned about the possibility of this metastasizing?
nope, glomangiomas are benign
100
An ED physician gets a patient who presents with Dyspnea on Exertion. PE is notable for an S3 heart sound. Echo reveals a decrease LV EF of 35% secondary to structural abnormalities of the heart. Hx is significant for chronic abuse of both alcohol and cocaine. What type of cardiomyopathy is likely present?
Dilated cardiomyopathy
100
You are seeing a 2yo Asian patient who presents with strawberry tongue, fever, and conjunctival injection. PE also reveals hand swelling and cervical lymphadenopathy. While this disease is typically self limiting, these patient are at increased risk of developing aneurisms in what location?
coronary arteries
200
The image below is from a 65yo male pt who presents with syncope and DOE. Biopsy reveals a non-malignant tumor. What is the most likely Dx?

Myxoma
200
A 35yo Asian patient presents with fatigue, night sweats, vision changes, and concerns about their pulses. You note on PE that you are not able to feel their radial pulses. If a granulomatous disease is suspected, was vessels in the body are typically affected?
Aortic arch and branches.
200
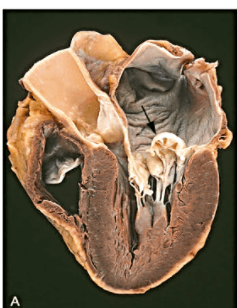
If the image taken below is from the heart of a patient with DOE and pulmonary edema, what is the likely type of cardiomyopathy that the patient is suffering from?
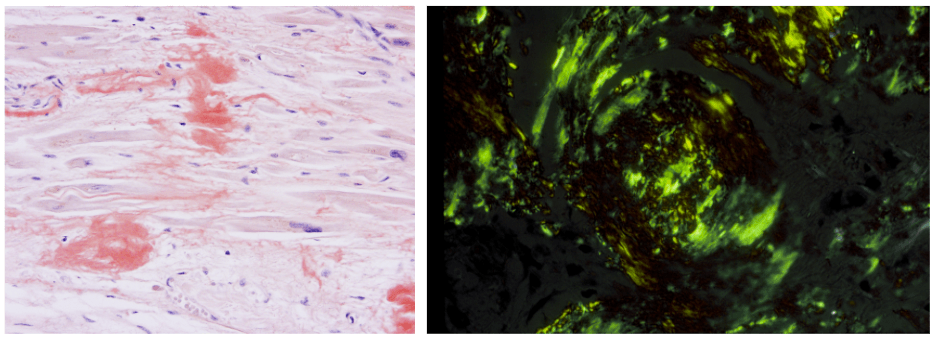
restrictive cardiomyopathy; secondary to amyloidosis
200
A patient presents to your office with concerns of joint pains, chest pain, a rash, and small firm nodules under the skin. Hx is significant for a sore throat 3 weeks ago, but pt did not go to the doctor then. ASO titers are high. The patient's disorder is likely to be caused Abs against which bacterial protein present in the initial infection?
M protein. Abs against this protein often exhibit cross reactivity against normal body proteins, leading to the sxs of rheumatic fever
200
A mother brings her 13yo son with concerns of sudden cases of epilepsy, headaches, and vision changes. The patient also has a noticeable nevus flemmus on the R side of his face. With which cranial nerve are these nevi typically associated with?
Usually follow the distribution of the trigeminal nerve
300
A patient presents to the ED with signs of a heart attack. A right-sided ECG is conducted and shows ST elevations in RV3-RV6. Your coworker wants to give nitrates to the patient. Why should they fire your coworker?
R ventricular infarction is highly dependent on preload to keep perfusion up. Decreasing preload will cause the patient to go into cardiogenic shock due to lack of CO
300
A patient presents with the below rhythm:

What is the rhythm indicated by the arrows, and what medication, which acts on Na/K ATPase, is responsible for the development of these abnormal beats
PJCs, digoxin
300
5 weeks after having a lateral wall MI, a patient suffers from a sudden cardiac death. Autopsy reveals an out-pouching of the ventricular wall, which had ruptured and leads to severe, acute cardiac tamponade. Analysis of the outpouching revealed that it was only comprised of thrombus components and pericardium. What is the name for this type of pathology?
pseudoaneurism
300
A 42 yo female presents with CKD and abdominal pain. Extensive testing indicates that the patient has a fibrinous disease of medium sized vessels that typically spares the lungs. 1/3 of all patients with this disease have IgG Abs against which virus that is commonly associated with this disorder?
HBV
300
A patient presents 5 days post-MI to the ED with signs of cardiogenic shock. ECHO reveals a ventricular septal rupture. In which leads were there most likely ST elevations during the initial STEMI?
V1-V4 (anterior leads)
400
a 16Yo female is brought in by her mother with concerns of small bruises appearing over her body. Hx reveals an increase in the number of nosebleeds that the patient has been having. Additionally, they also report numerous small growths on her skin, similar to the image below:

Pt has no history of travel, and all microbiological testing comes back negative. Is it likely that the pt's mother or father also had this disease?
yes, Heriditery Hemorrhagic Telangiectasia is autosomal dominant
400
A patient presents with sudden onset of hypotension, tachycardia, dyspnea, and pulmonary edema. PE positive for Holosystolic blowing murmur. Hx is significant for a STEMI 3 days ago, with ST elevations in leads II, III, and AVF. Assume a structure that was damaged during the STEMI is responsible for the spontaneous decomposition of the patient. What is the most likely artery that feeds this structure.
R coronary artery (inferior MI can lead to spontaneous posterior papillary rupture)
400
Sxs of pre-eclampsia
Gestational hypertension and proteinuria
400
A patient suffering from and NSTEMI comes to your ED. Your coworker wants to administer fondaparinux orally to prevent further thrombus formation. Why is this not a good idea?
This medication can only be given via injection
400
A cardiac pt presents with an arrhythmia where the SA node is no longer the dominant pace maker, it is now the AV node. What would we expect the pt's heart rate to be?
40-60
500
A biopsy of a heart from a patient that suffered an MI showed contraction band necrosis in the area supplied by the Left circumflex artery. In what leads on and ECG would ST elevation have appeared while the patient was actively having an attack?
Lateral leads; I, AVL, V5, V6
500
You are seeing a pregnant patient who suddenly develops Afib from the increased blood volume associated with pregnacy. Pt is generally asymptomatic, and does not have RVR. However, you would like to wait and see if Afib resolves post-delivery in a few weeks. As of right now, you just want to control for potential thrombus formation. The class of medication that you would give to the patient operates by binding to what enzyme?
antithrombin
500
A 67 yo patient presents with c/o of DOE. Echo shows marked thickening of the LV. CBC reveals an anemia is present, and peripheral blood smear shows fragmented erythrocytes. PE is positive for Crescendo-decrescendo systolic murmur, preceded by a click, heard best at 2nd R intercostal space. Pt. has never had rheumatic fever. What is the most likely underlying etiology that is causing the pt's symptoms?
Aortic stenosis most likely caused by calcific degeneration
500
A patient presents to the ED with an accelerated ventricular rate following an ischemic event. PE shows hearing loss, diaphoresis, and a HR of 190. Your colleague gives the patient Quinidine to slow their heart rate. Shortly after administration, heart rate slows to 85 BPM, but then rapidly turns into this arrhythmia:

What underlying genetic disorder could have predisposed the patient to developing this condition?
Jervell and Lange-Nielsen Syndrome
500
When dealing with a patient with ischemic heart disease, where in the heart does damage occur first (generally) when blood flow is cut off?
subendocardial area in the center of the ischemic zone
