Fluids
Hyponatremia
Hypernatremia
Hypokalemia
Hyperkalemia
100
What two compartments is total body water divided into?
Intracellular fluid (ICF) and extracellular fluid (ECF)
100
What serum sodium defines hyponatremia?
<138 mEq/L
100
What serum sodium defines hypernatremia?
>145 mEq/L
100
What serum potassium define hypokalemia and what is the most common cause of hypokelamia?
<3.5
Insufficient dietary intake
100
What test is necessary in all hyperkalemia patients?
EKG
200
Name 5 signs or symptoms of dehydration
Dark urine or decreased urine output, dizziness (orthostasis), dry axilla, tachycardia, neurologic impairment, sunken eyes, skin tenting, dry mouth
200
Two main causes of hypoosmolar hyponatremia?
SIADH and cerebral salt wasting syndrome
200
What are the most common symptoms of DI?
Thirst, polydipsia, and polyuria
200
Treatment of severe hypokalemia (<2.5 mEq/L) or symptomatic patients with moderate (2.5 to 3 mEq/L) hypokalemia
IV potassium
200
What serum potassium defines hyperkalemia and what is the most common cause?
[K+] of >5.5 mEq/L
Most common cause = factitious hyperkalemia caused by hemolysis during phlebotomy
300
What percentage of body weight is total body water?
60%
300
Rate of correction of sodium for chronic hyponatremia?
6 mEq/24 hours for high risk patients and 12 mEq/24 hours for low risk patients
300
What is the difference between central diabetes insipidus and nephrogenic diabetes insipidus?
Central diabetes insipidus (also called neurogenic) is due to inadequate ADH secretion. Nephrogenic diabetes insipidus (also called nephrogenic) occurs because the v2R receptors of the kidney’s collecting duct cells do not respond appropriately to ADH.
300
What electrolyte abnormality typically coexists with severe hypokalemia?
Hypomagnesemia
300
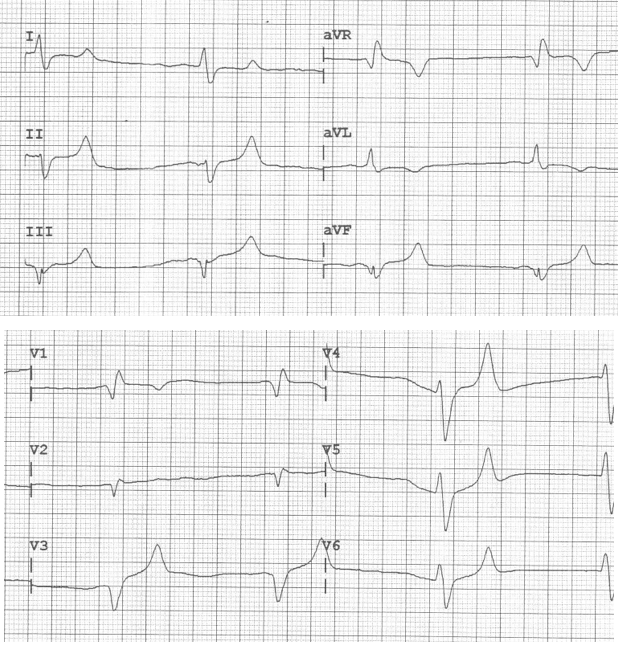
A 67-year-old man presents with generalized weakness. He has had poor oral intake for several days. An ECG is performed as seen above. Which of the following medications should immediately be administered?
What test
- Aspirin
- Calcium
- Dextrose
- Sodium bicarbonate
400
Equation for osmolality
2 × [Na+] + glucose/18 (normal range, 275 to 290 mOsm/L)
400
Treatment of seizing patient with hyponatremia?
The initial treatment includes infusion of 100-150 mL 3% hypertonic saline over 15–20 min, May repeat 150 mL of 3% hypertonic saline up to 3 total doses,or a total of 450 mL IV of3% hypertonic saline
400
Rate of sodium correction for hypernatremia?
Acute: 1 mEq/L/h
Chronic: 0.5 mEq/L/h or 10 to 12 mEq/24 h
400
What are the EKG findings possible with hypokalemia?
Prolonged QTc, flattened T wave, U wave
400
Treatment for hyperkalemia with mechanism of action of each step in treatment
1. Calcium (chloride or gluconate) - stabilizes the cardiac membrane
2. Sodium bicarb - shifts potassium intracellularly
3. Insulin and glucose - shifts potassium intracellularly
4. Albuterol - upregulates cyclic adenosine monophosphate and shifts potassium intracellularly
5. Lasix - increased renal secretion of potassium
6. Sodium polystyrene sulfonate (Kayexalate) or
sodium zirconium cyclosilicate (Lokelma) - increases GI potassium secretion
7. Hemodialysis
500
What is the difference between osmolarity an osmolality?
Osmolarity is the measure of solute concentration per unit volume of solvent. Osmolality is the measure of solute concentration per unit mass of solvent.
500
What are 5 symptoms of osmotic demyelination syndrome?
Dysarthria, dysphagia, lethargy, paraparesis or quadriparesis, seizures, and coma.
500
What can occur if you correct chronic hypernatremia to quickly?
Cerebral Edema
500
Name 5 signs or symptoms of hypokalemia
Hypertension, orthostatic hypotension, malaise, weakness, fatigue, hyporeflexia, cramps, paresthesias, nausea, vomiting, abdominal distention
500
What are the main EKG changes based on different potassium levels?
6.5–7.5 = Prolonged PR interval, tall peaked T waves, short QT interval
7.5–8.0 = Flattening of the P wave, QRS widening
10–12 = QRS complex degradation into a sinusoidal pattern