What A Headache
Random Rigmarole
Copy Cat
100
This headache is rare and characterized by ipsilateral cranial autonomic symptoms. This is shown to be effective in terminating acute episodes of these headaches
Administration of 100% oxygen
Effective in terminating acute episodes of cluster headache in up to 80% of individuals. The exact mechanism is unknown, but it is thought to involve the vasoconstriction of cranial blood vessels in response to high oxygen concentration and hypocapnea.
100
One clinical feature of atypical auras is paresis. This physical exam technique is used to detect true vs. false leg paresis. This is its name and the differential diagnosis we're attempting to rule in/out
Hoover's for Malingering
Disclaimer: SOR C due to small, lower-quality case control studies but obviously used in practice at times nevertheless.
Cup heels and have patient press down with paretic limb, then have patient raise opposite limb. True diagnostic paresis if no difference in downward pressure at heels.
100
In addition to fever, brain abscesses often present with persistent headaches. These are the two absolute indications for immediate stereotactic aspiration of the abscess according to UWorld
Larger than 2-2.5cm
Clinical features of increased ICP
A neurosurgeon should be consulted at the time of initial diagnosis of brain abscess in all patients. In most settings, needle aspiration or surgical excision should be performed to identify the causative pathogen prior to the initiation of antibiotic therapy and to reduce the size of the collection
300
This headache is often described as dull, pressing and nonpulsating holocranial pain that frequently recur several times per month for more than three months. This is the type of headache and the prophylactic treatment of choice
Chronic Tension Headache
Amitriptyline is the prophylactic treatment of choice for chronic tension headache, which is defined as episodes occurring at least 15 days per month for more than 3 months. In addition to amitriptyline, lifestyle and behavioral modification (e.g., exercise, sleep, avoiding stress) are crucial for the treatment of tension headaches. The patient has had significant stress in her life, and avoidance of stressful situations would likely help to reduce her symptoms.
300
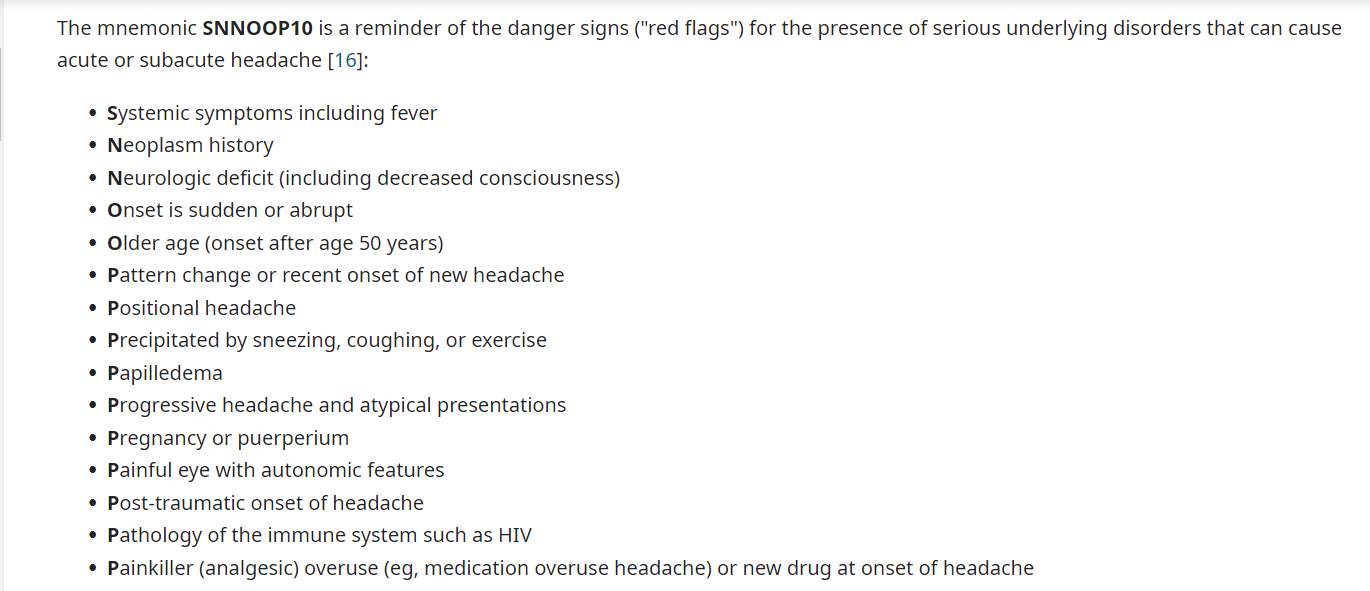
When a patient presents for evaluation of a headache, it is important to assess for warning signs that should lead to the consideration of early imaging. These are three of them
The mnemonic SNNOOP10 is a reminder of the danger signs ("red flags") for the presence of serious underlying disorders that can cause acute or subacute headache according to UpToDate
300
This headache is often a diffuse (but sometimes bifrontal), pulsating headache that is exacerbated by physical activity and may be accompanied by altered mental status.
Hypertensive Crises
Clinical diagnosis: elevated BP (>180/120) with (emergency) or without (urgency) signs of end-organ damage
- Labs: anemia, ↑ creatinine, ↑ BNP, proteinuria, hematuria
- ECG: left ventricular hypertrophy, signs of cardiac ischemia (e.g., ST depressions or elevations)
- Chest x-ray: cardiomegaly, pulmonary edema
500
These drugs are considered first-line agents for monotherapy for acute migraine attacks when the migraine is associated with vomiting/nausea according to AMBOSS. These are the two preferred drugs and the drug class to which they belong.
Parenteral metoclopramide or prochlorperazine-- antidopaminergic antiemetics
500
A causal association between migraine aura and headache is supported by evidence that both are linked to the phenomenon known as
Cortical spreading depression of Leão
Cortical spreading depression is a self-propagating wave of neuronal and glial depolarization that spreads across the cerebral cortex. Cortical spreading depression is hypothesized to
●Cause the aura of migraine
●Activate trigeminal nerve afferents (pain!!)
●Alter blood-brain barrier permeability by matrix metalloproteinase activation and upregulation
500
Immunosuppressed patient presents with weeks of increasing headache, vomiting, lethargy with fever. CT of the head show moderate hydrocephalus and basilar meningeal enhancement; no mass lesions are present. This is the most likely diagnosis
TB meningitis
Tuberculous meningitis is typically marked by subacute symptoms of meningeal irritation (eg, vomiting, headache, nuchal rigidity) and imaging findings of basilar meningeal enhancement, hydrocephalus, and stroke due to vasculitis. Risk is increased with immunocompromise (eg, HIV)