Is It PE or Just Vibes?
Coughing for 3–5 Business Days
Crackles & Crisis
LABA Drama
Withdrawal Weekend
Spray It and Pray
100
1. A 24-year-old female presents with complaints of intermittent shortness of breath and wheezing, particularly when visiting her parents who have a cat. She denies daily symptoms. Spirometry performed in the office shows an FEV1/FVC ratio of 68%. You administer a short-acting bronchodilator. Which of the following post-bronchodilator results would most strongly confirm a diagnosis of asthma?
A. An increase in FEV1 of ≥ 8%
B. An increase in FEV1 of ≥ 10%
C. An increase in FEV1 of ≥ 12%
D. Normalization of the FEV1/FVC ratio to exactly 70%
E. No change in FEV1, but patient reports feeling better
Answer: C (An increase in FEV1 of ≥ 12%)
Explanation: Reversibility of airway obstruction is a key diagnostic feature of asthma. The source states that a diagnosis involves an improvement in FEV1 of ≥ 12% after the administration of a bronchodilator.
100
A 6-year-old girl is brought to the clinic by her father. She has been using her albuterol inhaler 4 times a week for the past month and had to sit out of gym class twice last week due to coughing. The provider decides to initiate daily controller therapy. According to the stepwise approach, what is the preferred controller choice for Step 3 management? A. High dose ICS-formoterol scheduled
B. Low dose ICS-formoterol as needed (PRN)
C. Low dose ICS-formoterol scheduled
D. Oral Leukotriene Receptor Antagonist (LTRA)
E. Long-Acting Muscarinic Antagonist (LAMA) monotherapy
Answer: C (Low dose ICS-formoterol scheduled)
Explanation: According to the "Stepwise Approach (12 Years and Older)" chart provided in the source (Note: clinical judgement applies to age, but the chart is the reference), Step 3 preferred controller choice is Low dose ICS-formoterol scheduled. Step 1 & 2 use PRN dosing.
100
A 30-year-old patient presents to the clinic with fever, malaise, cough, and dyspnea on exertion for the past 2 weeks and also reports arthralgias. The patient is a Black woman. Chest radiograph reveals bilateral hilar adenopathy and pulmonary infiltrates. Biopsy reveals noncaseating granulomas. Mycobacterial and fungal cultures are negative, and the patient has no suspicious environmental exposures. Which of the following is the most likely diagnosis?
Histoplasmosis
Hypersensitivity pneumonitis
Sarcoidosis
Tuberculosis
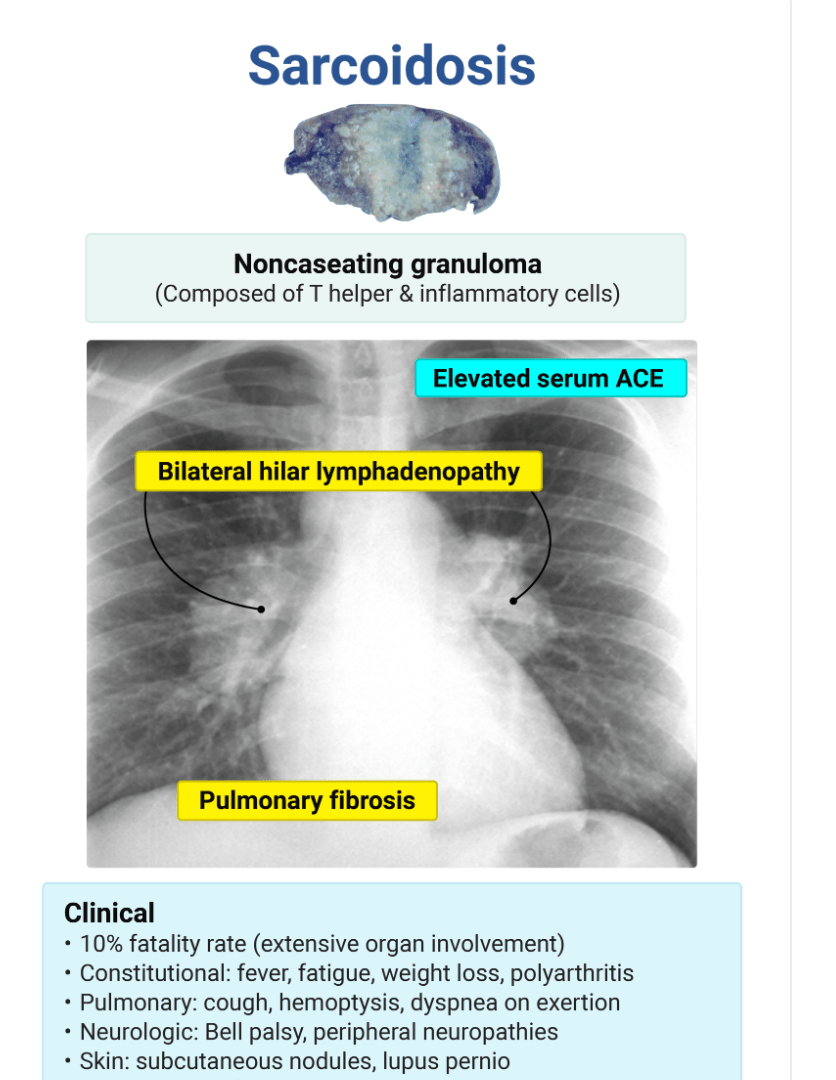 Explanation:may present with similar symptoms, such as fever, cough, malaise, and dyspnea on exertion. It is most often asymptomatic but can cause severe disease in immunocompromised patients. Histoplasmosis is endemic to the Ohio and Mississippi River valleys. Fungal cultures should be obtained prior to initiating treatment in a patient with sarcoidosis. This culture is necessary because the two conditions can present similarly, and treating a patient with histoplasmosis with systemic steroids can lead to dissemination of the disease. usually occurs in the setting of an occupational or environmental exposure. The symptoms of cough and dyspnea on exertion may be similar. presents with systemic and pulmonary symptoms, as well. Tuberculin skin test and mycobacterial cultures should be performed in patients with suspected sarcoidosis to rule out tuberculosis. This patient had negative culture results.
Explanation:may present with similar symptoms, such as fever, cough, malaise, and dyspnea on exertion. It is most often asymptomatic but can cause severe disease in immunocompromised patients. Histoplasmosis is endemic to the Ohio and Mississippi River valleys. Fungal cultures should be obtained prior to initiating treatment in a patient with sarcoidosis. This culture is necessary because the two conditions can present similarly, and treating a patient with histoplasmosis with systemic steroids can lead to dissemination of the disease. usually occurs in the setting of an occupational or environmental exposure. The symptoms of cough and dyspnea on exertion may be similar. presents with systemic and pulmonary symptoms, as well. Tuberculin skin test and mycobacterial cultures should be performed in patients with suspected sarcoidosis to rule out tuberculosis. This patient had negative culture results.
100
A 68-year-old male with a history of severe COPD and benign prostatic hyperplasia (BPH) presents with increased urinary retention and dry mouth. Which of the following inhaled medications is the most likely cause of these adverse effects?
A. Albuterol (ProAir HFA)
B. Tiotropium (Spiriva)
C. Fluticasone (Flovent)
D. Salmeterol (Serevent)
E. Budesonide (Pulmicort)
Answer: B
Explanation: Tiotropium is a Long-Acting Muscarinic Antagonist (LAMA). Antimuscarinics/Anticholinergics can cause urinary retention and should be used with caution in patients with prostatic hyperplasia.
100
Which of the following antidepressants is an FDA-approved first-line agent for smoking cessation?
A. Nortriptyline (Pamelor)
B. Fluoxetine (Prozac)
C. Bupropion SR (Zyban)
D. Sertraline (Zoloft)
E. Paroxetine (Paxil)
C. Bupropion SR (Zyban).
Explanation: Bupropion is the only FDA-approved antidepressant for this indication. Nortriptyline is second-line and off-label,,.
100
A patient with chronic asthma is prescribed Advair HFA (Fluticasone/Salmeterol). Two weeks later, he complains of a sore throat and white patches on his tongue. This adverse effect is caused by the mechanism of which component, and how could it have been prevented?
A. Salmeterol; by taking the medication on an empty stomach.
B. Fluticasone; by rinsing the mouth with water and spitting after use.
C. Salmeterol; by using a spacer.
D. Fluticasone; by taking an antihistamine concurrently.
E. The propellant; by shaking the canister vigorously before use.
Answer: B
Explanation: Oral candidiasis (thrush) is a common side effect of ICS (Fluticasone). It can be prevented by rinsing the mouth with water and spitting it out after every use.
200
A 16-year-old male football player presents for a sports physical. He reports that during intense practice in the cold autumn air, he often develops a cough and chest tightness about 15 minutes into the session. He has no symptoms at rest or during the school day. He currently takes no medications. Which of the following is the most appropriate prophylactic intervention for this patient?
A. Oral corticosteroids 2 hours before practice
B. Inhaled Short-Acting Beta-Agonist (SABA) 5-15 minutes before practice
C. Inhaled Long-Acting Muscarinic Antagonist (LAMA) daily
D. Inhaled Long-Acting Beta-Agonist (LABA) immediately before practice
E. Daily Leukotriene Receptor Antagonist (LTRA) starting 30 minutes before practice
Answer: B (Inhaled Short-Acting Beta-Agonist (SABA) 5-15 minutes before practice)
Explanation: For Exercise-Induced Bronchospasm (EIB), SABAs are 80% efficacious and should be taken minutes (typically 5-15) before exercise. They last 2-3 hours. LABAs can be used but are taken 15-30 minutes prior.
200
A 15-year-old male (Marcos) presents with a persistent dry cough worsening at night. He denies fever or heartburn. His father has asthma. Physical exam reveals end-expiratory wheezing. If this patient’s spirometry was normal, which diagnostic test would be most appropriate to confirm the diagnosis of asthma?
A. Chest X-ray
B. CT of the chest
C. Bronchoprovocation test
D. Sweat chloride test
E. Sputum culture
Answer: C (Bronchoprovocation test)
Explanation: If spirometry is normal but clinical suspicion is high (chronic cough, intermittent wheeze), a Bronchoprovocation test (e.g., Methacholine challenge) is indicated. A positive result shows bronchoconstriction.
200
A 45 year-old male presents with sudden onset of pleuritic chest pain, productive cough and fever for 1 day. He relates having symptoms of a "cold" for the past week that suddenly became worse yesterday. Which of the following findings will most likely be seen on physical examination of this patient?
A. spoken "ee" heard as "ay"
B. hyperresonant percussion note
C. wheezes over the involved area
D. vesicular breath sounds over involved area
This patient most likely has a bacterial pneumonia with consolidation, which would produce egophony, where a spoken "ee" is heard as "ay."
200
Which of the following statements accurately describes the "Black Box Warning" associated with Long-Acting Beta Agonists (LABAs) like Salmeterol when used in the treatment of asthma?
A. They cause significant adrenal suppression in children.
B. Monotherapy increases the risk of asthma-related death.
C. They are associated with a high risk of tendon rupture.
D. They cause irreversible hepatic failure.
E. They significantly increase the risk of developing pneumonia.
Answer: B
Explanation: LABAs have a Black Box Warning stating that monotherapy (using LABA without an ICS) in asthma treatment increases the risk of asthma-related death.
200
A 29-year-old female is starting Varenicline (Chantix) for smoking cessation. She plans to quit smoking on October 14th. Based on the pharmacokinetic profile and dosing guidelines of the drug, when should she take her first dose?
A. October 14th (on her quit date)
B. October 7th (1 week prior to quit date)
C. September 14th (1 month prior to quit date)
D. October 1st (2 weeks prior to quit date)
E. October 15th (1 day after her quit date)
B. October 7th (1 week prior to quit date).
B. October 7th (1 week prior to quit date).
Explanation: Varenicline should be started 1 week before the quit date to titrate the dose and block receptors before the final cigarette.
200
A patient using Brimonidine (Alphagan P) eye drops complains of drowsiness. You explain that this is a known adverse reaction. To which pharmacological class does this medication belong?
A. Prostaglandin Analog
B. Beta-Blocker
C. Alpha-2 Adrenergic Agonist
D. Carbonic Anhydrase Inhibitor
E. Anticholinergic
C. Alpha-2 Adrenergic Agonist
Explanation: Brimonidine is listed under Alpha-2 Adrenergic Agonists. Common adverse drug reactions for this class include drowsiness and eye pruritus.
300
A 28-year-old female with diagnosed asthma presents for a follow-up. She reports waking up with coughing and wheezing approximately 2 times per week. She also uses her rescue inhaler 5 days a week for daytime symptoms. According to the "Preferred Controller Initiation" guidelines, which step of management is most appropriate for this patient?
A. Step 1
B. Step 2
C. Step 3
D. Step 4
E. Step 5
Answer: C (Step 3)
Explanation: The patient has symptoms most days (5 days/week) and wakes up with asthma > 1x/week (2x/week). The "Preferred Controller Initiation Approach" indicates that if a patient has symptoms most days OR wakes due to asthma ≥ 1x/week, they should start at Step 3.
300
A 62-year-old male with a 40-pack-year smoking history presents with a "barrel chest," pursed-lip breathing, and significant muscle wasting. He is leaning forward in a tripod position. Which of the following pathological changes primarily explains his airflow limitation?
A. Excessive mucus production plugging the large airways
B. Fibrosis of the pulmonary capillaries
C. Loss of elastin tethering causing airway collapse during exhalation
D. Hyper-responsiveness of the smooth muscle to allergens
E. Impaired ciliary motility in the trachea
Loss of elastin tethering causing airway collapse during exhalation.
Explanation: In emphysema, the destruction of elastin fibers removes the radial traction that holds small airways
300
A 29-year-old man presents to the emergency department with new-onset dyspnea and right-sided chest pain. He is tall and thin, his vital signs are within normal limits except for an oxygen saturation of 92%, and chest X-ray reveals a pneumothorax with a 3.5 cm rim of air in the right pleural space. Which of the following represents the best initial treatment for this patient?
Chest tube thoracostomy
Needle aspiration
Supplemental oxygen and observation
Video assisted thoracoscopic surgery
Needle aspiration
Chest tube thoracostomy (A) is reserved for patients who are hemodynamically unstable, patients in whom needle aspiration fails, patients with recurrent pneumothorax, and patients with concurrent hemothorax. Supplemental oxygen and observation (C) alone, without removal of pleural air by any means, is reserved for stable patients with a pneumothorax measuring under 3 cm. Supplemental oxygen should be administered to any patient with a pneumothorax as it aids in the reabsorption of pleural air. Patients with a small pneumothorax should be observed for at least six hours, and serial chest radiographs should be obtained during that time to ensure that the pneumothorax is not growing and that the lung is reinflating. Video-assisted thoracoscopic surgery (D) can be performed on patients who fail needle aspiration and on patients who have hemopneumothorax or a large pneumothorax. During the surgery, pleurodesis can be performed.
300
You are treating a 9-year-old patient with Step 4 severe persistent asthma. You are considering adding a biologic agent. The patient’s lab work reveals an elevated serum IgE level and positive skin tests to perennial allergens. Which of the following agents utilizes a mechanism of action that inhibits the binding of IgE to the high-affinity IgE receptor on mast cells?
A. Mepolizumab (Nucala)
B. Benralizumab (Fasenra)
C. Dupilumab (Dupixent)
D. Omalizumab (Xolair)
E. Reslizumab (Cinqair)
Answer: D
Explanation: Omalizumab (Xolair) is an anti-IgE monoclonal antibody. It inhibits the binding of IgE antibodies to the receptor on mast cells and basophils. Mepolizumab, Reslizumab, and Benralizumab target IL-5.
300
A 45-year-old male presents to the clinic motivated to quit smoking. He states he smokes his first cigarette within 5 minutes of waking up every morning. He prefers to use a lozenge rather than a patch. Which of the following is the most appropriate starting pharmacotherapy regimen for this patient?
A. Nicotine lozenge 2 mg; one piece every 1–2 hours
B. Nicotine lozenge 4 mg; one piece every 1–2 hours
C. Nicotine lozenge 2 mg; one piece every 4–8 hours
D. Nicotine lozenge 4 mg; one piece every 4–8 hours
E. Nicotine lozenge 4 mg; one piece daily as needed for cravings
B. Nicotine lozenge 4 mg; one piece every 1–2 hours.
Explanation: Dosing for gum/lozenges is based on "Time to First Cigarette" (TTFC). If TTFC is < 30 minutes, use the 4 mg dose. The starting schedule is 1 piece q 1-2h.
300
According to the "Lock and Key Hypothesis," why is the molecular weight of a drug important?
Larger drugs are always more potent.
Drugs must be between 100–1000 g/mole to have a unique structure that facilitates selective receptor binding.
Smaller drugs (under 100 MW) bind more tightly to receptors.
Molecular weight determines the toxicity of the drug.
2 – Sufficient size (100-1000 MW) gives a unique structure for selective binding
400
A 32-year-old female non-smoker presents with dyspnea on exertion. A CT scan of the chest reveals panacinar emphysema predominantly in the lower lobes. Which of the following pathophysiological mechanisms is most likely responsible for this patient’s condition?
A. Uninhibited neutrophil elastase activity due to protein deficiency
B. Chronic mucus hypersecretion from goblet cell hypertrophy
C. Hypoxic vasoconstriction leading to pulmonary hypertension
D. Oxidative stress caused by inhalation of biomass fuels
E. IgE-mediated hypersensitivity reaction to environmental allergens
A. Uninhibited neutrophil elastase activity due to protein deficiency.
Explanation: This vignette describes Alpha-1 Antitrypsin (A1AT) deficiency (young age, non-smoker, lower lobe panacinar emphysema). A1AT normally inhibits neutrophil elastase; without it, elastin is destroyed.
400
A 66-year-old "blue bloater" presents with worsening dyspnea, peripheral edema, and jugular venous distention (JVD). What is the underlying physiological cause of his edema and JVD?
A. Left ventricular hypertrophy
B. Cor Pulmonale (Right heart failure) due to pulmonary hypertension
C. Severe hypoalbuminemia due to malnutrition
D. Acute renal failure
E. Hepatic cirrhosis secondary to alpha-1 antitrypsin deficiency
Cor Pulmonale (Right heart failure) due to pulmonary hypertension.
Explanation: Chronic alveolar hypoxia leads to pulmonary vasoconstriction and hypertension. This increases the afterload on the right ventricle, leading to right heart failure (Cor Pulmonale), which presents with edema and JVD.
400
Which of the following best describes the pathophysiology of bronchiectasis?
Bronchial wall thickening and permanent airway dilation due to recurrent inflammation
Focal infection involving the pulmonary parenchyma
Hyperresponsiveness of the airway to the environmental allergens
Lower respiratory tract infection involving the bronchi
Bronchial wall thickening and permanent airway dilation due to recurrent inflammation
Explation
Focal infection involving the pulmonary parenchyma (B) describes pneumonia. Pneumonia presents as an acute illness with cough and usually changes in vital signs (e.g., fever, tachycardia, tachypnea). Hyperresponsive of the airways to environmental allergens (C) describes the pathology behind reactive airway disease, such as asthma. Asthma is associated with triggers, causes reversible airway obstruction, usually presents during childhood, and causes intermittent cough, wheezing, and shortness of breath. Asthma symptoms may be worse at night. Lower respiratory tract infection involving the bronchi (D) describes acute bronchitis. Acute bronchitis presents clinically as a cough for more than five days and typically lasts one to three weeks.
400
Which of the following is an example of an Enzymatic Receptor?
Insulin Receptor
Nicotinic Cholinergic Receptor
Estrogen Receptor
Adrenergic Receptor
1 – The Insulin Receptor is an enzymatic receptor
400
A 40-year-old man with a history of intermittent asthma treated with as-needed albuterol presents with worsening asthma symptoms over the past 3 weeks. Cough, shortness of breath, and wheezing have limited his ability to perform his normal activities, such as gardening. He reports using his albuterol inhaler daily to control his symptoms. He is also waking up at night once or twice a week with cough and wheezing. Which of the following would be the preferred medication to control his asthma at this time?
Cromolyn nebulizer 1 ampule four times per day
mometasone dry powder inhaler 110 mcg/actuation
Montelukast 10 mg at bedtime
theophylline 300 mg daily
mometasone dry powder inhaler 110 mcg/actuation 1 puff at night
Cromolyn nebulizer 1 ampule four times per day (A) and theophylline 300 mg daily (D) are rarely used nowadays and should be avoided due to their low efficacy.
Montelukast 10 mg at bedtime (C), like other leukotriene receptor antagonists, is less effective than an inhaled corticsteroid but may be used as an alternative treatment in patients who need but cannot tolerate inhaled corticosteroid therapy. Montelukast is associated with an increased risk of serious mental disturbances, including suicidality.
This patient has increasingly severe symptoms suggesting that his asthma severity is no longer intermittent and is poorly-controlled. Therefore, he should proceed to step 2 therapy by adding a daily low-dose inhaled corticosteroid such as mometasone dry powder inhaler 110 mcg/actuation 1 puff at night, according to the National Asthma Education and Prevention Program guidelines and the Global Initiative for Asthma guidelines. The patient's previously diagnosed intermittent asthma is characterized by the following: daytime asthma symptoms occurring two or fewer days per week, two or fewer nighttime awakenings per month, use of rescue therapy to relieve symptoms no more than 2 days a week, no interference with normal activities between exacerbations, and one or no exacerbation requiring oral glucocorticoids in the preceding year.
400
Match the Receptor Type (A-E) to its correct Example/Description (1-5):A. G-Protein Coupled Receptor (GPCR) B. Ligand-Gated Ion Channel C. Enzymatic Receptor D. Cytokine Receptor E. Nuclear Receptor
_____ Includes the Nicotinic Cholinergic and GABAergic receptors.
_____ Includes Thyroid Hormone and Vitamin D receptors.
_____ Includes Growth Hormone and Erythropoietin receptors.
_____ Includes Adrenergic, Serotonergic, and Histamine receptors.
_____ Includes Insulin and Growth Factor receptors.
Part 2: Matching Answers
1. B (Ligand-Gated Ion Channel)
2. E (Nuclear Receptor)
3. D (Cytokine Receptor)
4. A (GPCR)
5. C (Enzymatic Receptor)
500
A 60-year-old female presents with a daily productive cough that has persisted for 4 months a year for the last 3 consecutive years. Spirometry confirms airflow obstruction. This clinical presentation is the definition of:
A. Emphysema
B. Chronic Bronchitis
C. Asthma-COPD Overlap
D. Bronchiectasis
E. Pneumonia
B. Chronic Bronchitis.
Explanation: Chronic Bronchitis is defined clinically as a chronic productive cough for 3 months for 2 or more consecutive years.
500
Which of the following is a common, nonpulmonary sequela of cystic fibrosis?
Infertility
Polycythemia
Poor visual acuity
Splenic autoinfarction
Infertility
Polycythemia (B) is not a common manifestation of cystic fibrosis. Generally, anemia is more common. Iron deficiency or chronic inflammation can cause the anemia of cystic fibrosis. Anemia may also be secondary to bone marrow suppression if the patient has undergone transplantation or can be the result of chronic blood loss through hemoptysis. Poor visual acuity (C) is not a sequela of cystic fibrosis. Splenic autoinfarction (D) is not common in cystic fibrosis. Patients with sickle cell disease are prone to splenic autoinfarction due to the abundance of sickled red blood cells that pass through it and cause ischemia.
500
A 23 year-old female with history of asthma for the past 5 years presents with complaints of increasing shortness of breath for 2 days. Her asthma has been well controlled until 2 days ago and since yesterday she has been using her albuterol inhaler every 4-6 hours. She is normally very active, however yesterday she did not complete her 30 minutes exercise routine due to increasing dyspnea. She denies any cough, fever, recent surgeries or use of oral contraceptives. On examination, you note the presence of prolonged expiration and diffuse wheezing. The remainder of the exam is unremarkable. Which of the following is the most appropriate initial diagnostic evaluation prior to initiation of treatment?
A Chest Xray
B Sputum gram stain
C peak flow
D V/Q scan
A peak flow reading will help you to gauge her current extent of airflow obstruction and is helpful in monitoring the effectiveness of any treatment interventions.
500
A 55-year-old male with COPD returns for a follow-up. He has had two moderate exacerbations in the past year despite strict adherence to his LAMA monotherapy. His blood eosinophil count is 150 cells/µL. What is the most appropriate pharmacological adjustment?
A. Add an Inhaled Corticosteroid (ICS)
B. Switch to a SABA monotherapy
C. Escalate to LABA + LAMA combination therapy
D. Add Roflumilast
E. Add Azithromycin
Answer: C
Explanation: For a patient in Group E (Exacerbate), the initial pharmacological treatment recommended is LABA + LAMA. ICS is generally considered if blood eosinophils are 300 cells/µL.
500
A heavy smoker (30 cigarettes/day) is interested in using the Nicotine Transdermal Patch (NicoDerm CQ). He complains that in previous attempts using the patch, he experienced vivid, disturbing dreams that disrupted his sleep. What is the most appropriate modification to his regimen?
A. Switch to the 14 mg patch immediately.
B. Remove the patch before bedtime and apply a new one in the morning.
C. Cut the patch in half to reduce the nightly dose.
D. Add an oral antihistamine at bedtime.
E. Apply the patch to the lower leg instead of the upper arm.
B. Remove the patch before bedtime and apply a new one in the morning.
Explanation: Vivid dreams are a side effect of nocturnal nicotine absorption. Removing the patch at bedtime eliminates this issue.
500
A 70-year-old male is preparing for a cruise and requests a transdermal scopolamine patch for motion sickness prevention. Reviewing his history, which of the following conditions would be a contraindication for this medication?
A. Hypertension
B. Open-angle glaucoma
C. Narrow-angle glaucoma
D. Peptic ulcer disease
E. Type 2 Diabetes
Narrow-angle glaucoma
Explanation: Scopolamine is an anticholinergic agent. A specific contraindication listed in the source is narrow-angle glaucoma.
600
A 68-year-old man presents to the office for a wellness exam. You order a chest X-ray because of a persistent cough. He formerly smoked, with a history of 40 pack-years, and has chronic obstructive pulmonary disease. He has worked in construction, manufacturing facilities, and as a coal miner. There is a 1 cm nodule in the right upper lobe. Which of the following is the most likely risk factor in the development of this nodule
Asbestos exposure
Beryllium exposure
Carbon and silica exposure
Hard metal exposure
Carbon and silica exposure
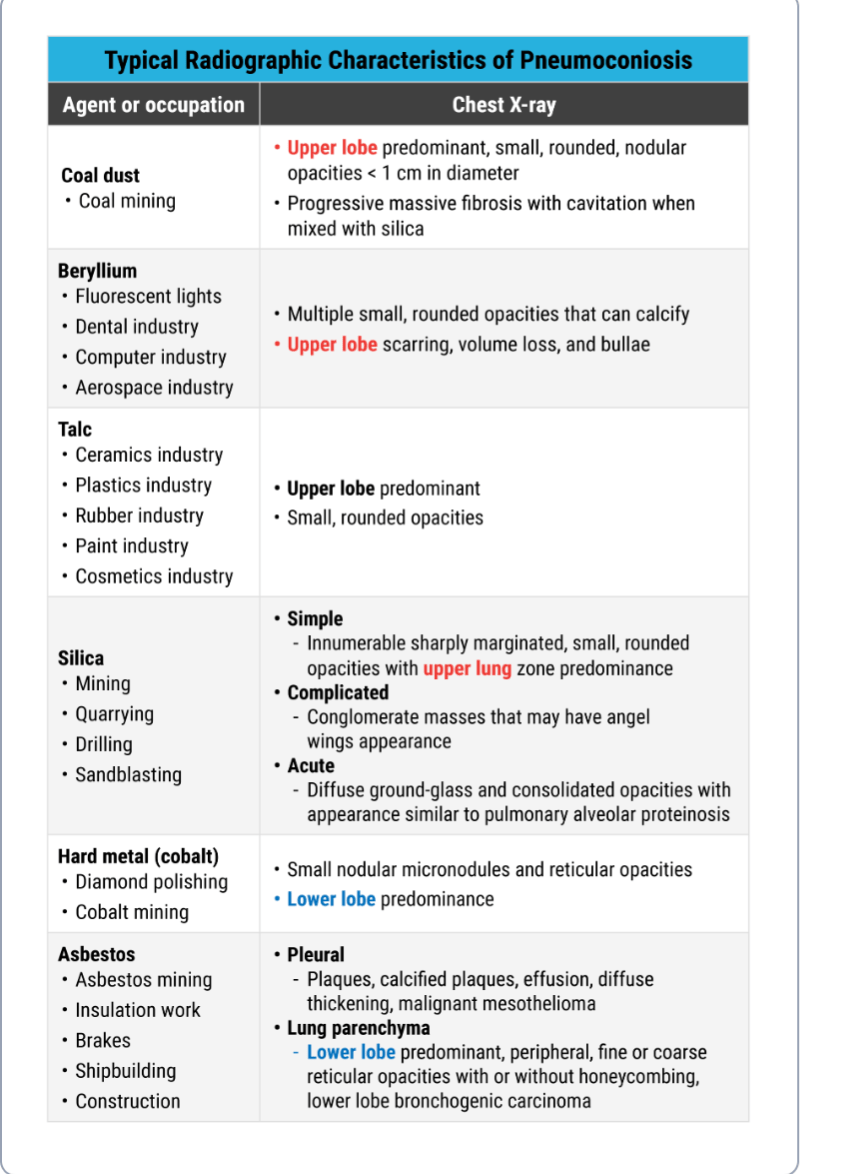 Asbestos exposure (A) is a risk factor for development of a myriad of pulmonary diseases, the most concerning being malignant mesothelioma. Asbestos is a fibrous magnesium silicate that is found in insulating material. Most exposures occur in mining and milling settings. Pleural plaques, pleural thickening, benign asbestos pleural effusions, and malignant mesothelioma are the spectrum of diseases produced by this occupational exposure. Pleural plaques on radiographs demonstrate a sunburst, punctate, or candle-dripping pattern. Pleural thickening often demonstrates blunting of the costophrenic angle and diffuse fibrosis. Malignant mesothelioma often demonstrates multiple radiographic changes, such as pleural effusions, nodular pleural masses, thickening of fissures, and diffuse pulmonary involvement. Beryllium exposure (B) due to inhalation of lightweight metals produces berylliosis. Beryllium was commonly used in fluorescent lights and is now found in the dental, computer, and nuclear industries. Berylliosis is a granulomatous disease. Radiographs reveal multiple, small, round opacities that may be calcified. Hard metal exposure (D) is different than heavy metal exposure. Hard metal pneumoconiosis develops after exposure to compacted cobalt, such as in diamond polishers. It creates asthma and diffuse interstitial fibrosis, so radiographic findings are often small nodular and reticular opacities primarily in the bases.
Asbestos exposure (A) is a risk factor for development of a myriad of pulmonary diseases, the most concerning being malignant mesothelioma. Asbestos is a fibrous magnesium silicate that is found in insulating material. Most exposures occur in mining and milling settings. Pleural plaques, pleural thickening, benign asbestos pleural effusions, and malignant mesothelioma are the spectrum of diseases produced by this occupational exposure. Pleural plaques on radiographs demonstrate a sunburst, punctate, or candle-dripping pattern. Pleural thickening often demonstrates blunting of the costophrenic angle and diffuse fibrosis. Malignant mesothelioma often demonstrates multiple radiographic changes, such as pleural effusions, nodular pleural masses, thickening of fissures, and diffuse pulmonary involvement. Beryllium exposure (B) due to inhalation of lightweight metals produces berylliosis. Beryllium was commonly used in fluorescent lights and is now found in the dental, computer, and nuclear industries. Berylliosis is a granulomatous disease. Radiographs reveal multiple, small, round opacities that may be calcified. Hard metal exposure (D) is different than heavy metal exposure. Hard metal pneumoconiosis develops after exposure to compacted cobalt, such as in diamond polishers. It creates asthma and diffuse interstitial fibrosis, so radiographic findings are often small nodular and reticular opacities primarily in the bases.
600
A 55-year-old male presents for a follow-up. His post-bronchodilator FEV1 is 45% of predicted. How would you classify the severity of his airflow limitation according to GOLD guidelines?
A. GOLD 1 (Mild)
B. GOLD 2 (Moderate)
C. GOLD 3 (Severe)
D. GOLD 4 (Very Severe)
E. GOLD 5 (End Stage)
C. GOLD 3 (Severe).
Explanation: GOLD 3 is defined as FEV1 between 30% and 49% of predicted.
600
A patient is reviewing their Asthma Action Plan with you. They ask what the "Green Zone" signifies regarding their Peak Expiratory Flow (PEF). You correctly reply that the Green Zone corresponds to a PEF of:
A. > 50% of personal best
B. > 60% of personal best
C. > 70% of personal best
D. > 80% of personal best
E. 100% of predicted value only
Answer: D (> 80% of personal best)
Explanation: The Asthma Action Plan defines the "Green Zone" (symptoms well controlled) as a PEF > 80-100% of the patient's personal best.
600
A 7-year-old boy is brought to the clinic by his mother. He has a history of allergic rhinitis and mild asthma. You consider prescribing Montelukast (Singulair). Before initiating therapy, you must counsel the mother regarding which serious Black Box Warning associated with this medication?
A. Increased risk of asthma-related death
B. Serious neuropsychiatric events, including aggression and suicidal ideation
C. Significant growth suppression
D. Increased risk of severe anaphylaxis
E. Potential for QTc prolongation
Answer: B
Explanation: In March 2020, a Boxed Warning was added to Montelukast regarding the risk of serious neuropsychiatric events, including agitation, aggression, depression, and suicidal thoughts/behavior.
600
A 55-year-old male is starting NRT Gum. He smokes about 15 cigarettes a day. Which of the following is a critical counseling point regarding the administration of the gum?
A. Chew the gum continuously like regular chewing gum to release the nicotine.
B. Drink coffee or soda while chewing the gum to enhance absorption.
C. "Chew and Park" the gum between the cheek and gums until the tingle is gone.
D. Spit out the gum after 10 minutes of chewing.
E. Use one piece of gum every 4 to 6 hours regardless of cravings.
C. "Chew and Park" the gum between the cheek and gums until the tingle is gone.
Explanation: Continuous chewing releases nicotine too fast (swallowed/wasted). "Chew and Park" allows buccal absorption.
600
2. A 24-year-old female presents with a "red, angry eye" for two days. She complains of copious purulent discharge that glues her eye shut in the morning. She is a daily contact lens wearer and admits to sleeping in them recently. Which of the following is the most appropriate first-line treatment for this patient?
A. Erythromycin ophthalmic ointment
B. Polymyxin B-trimethoprim drops
C. Ciprofloxacin ophthalmic drops
D. Oral Amoxicillin-clavulanate
E. Olopatadine drops
Ciprofloxacin ophthalmic drops
Explanation: While Erythromycin and Polymyxin B are preferred for general bacterial conjunctivitis, contact lens wearers require coverage for Pseudomonas. The source specifies that for contact lens wearers, a Fluoroquinolone (like Ciprofloxacin or Ofloxacin) should be used.