Take my breath away
You spin me right round
Vent out of shape
Lunguage arts
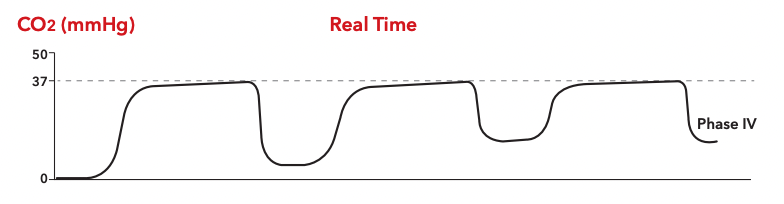
CO2 much to handle
100
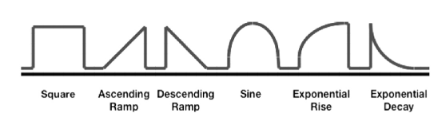
These are 3 of the 6 basic vent scalars.
100
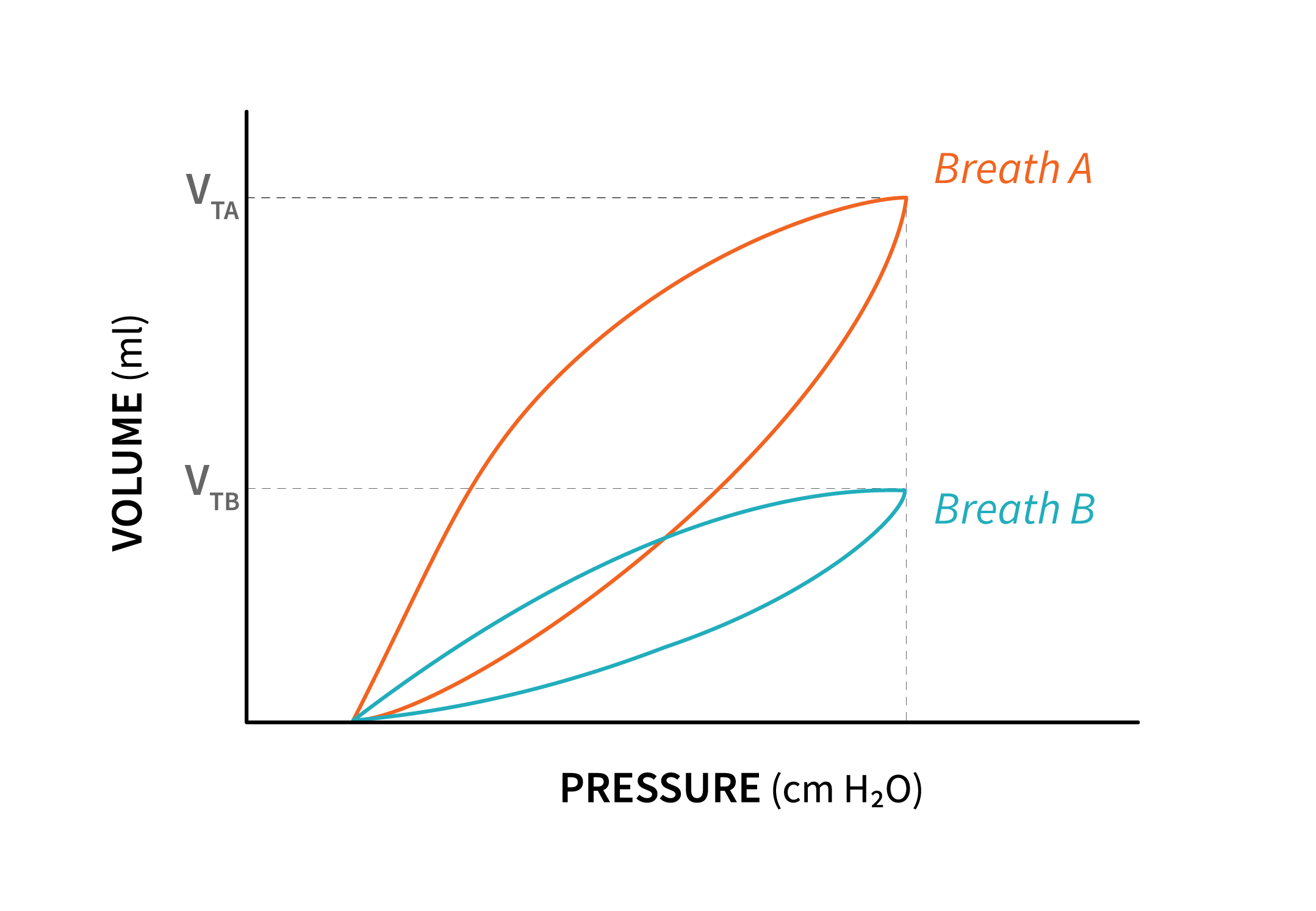
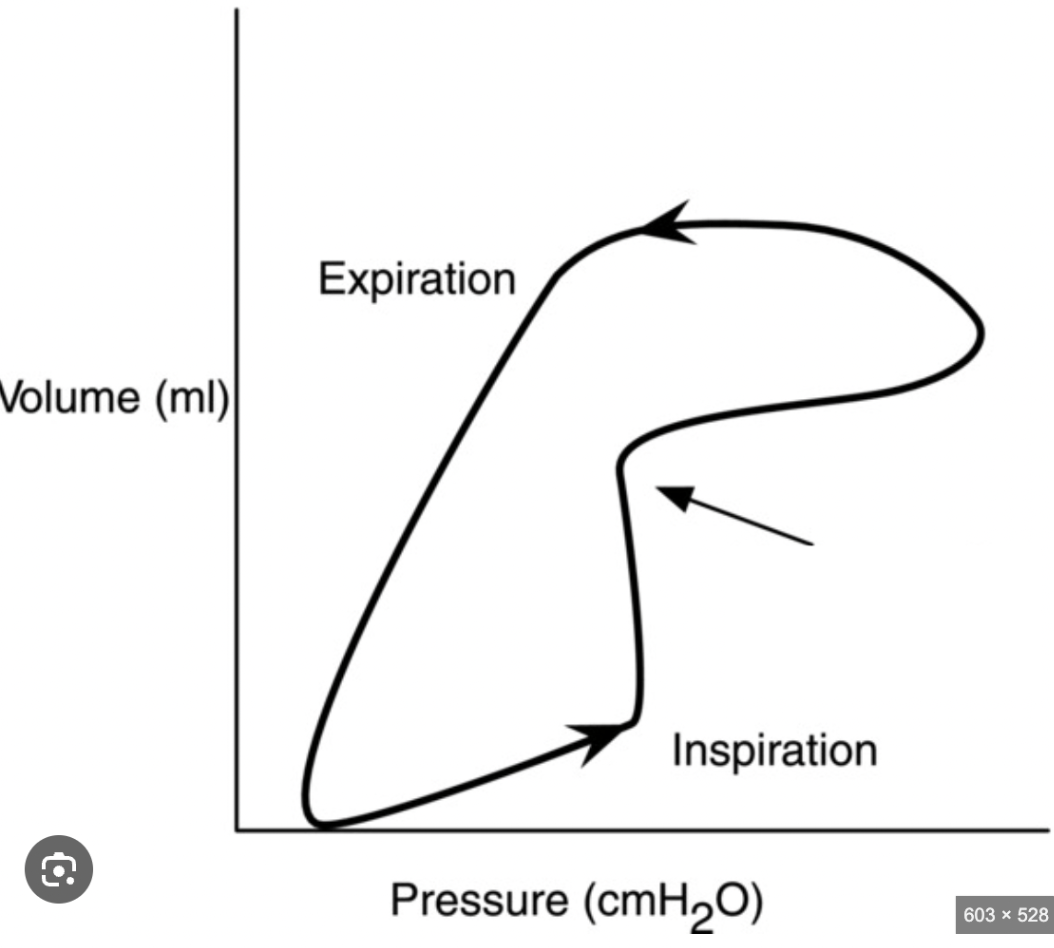
Name 3 things you would assess if you see breath B on your PV loops
pneumothorax
patient positioning for wxcessive tidal volume or PEEP
100
This issue increases the work of breathing and increases intathoracic pressures. It is indicated by the arrow below:
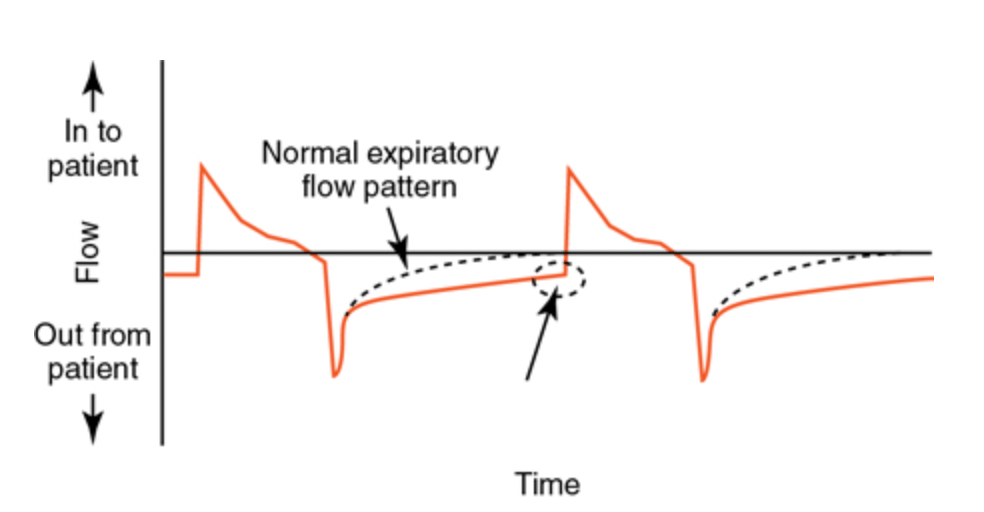
What is autoPEEP?
100
This is the equation for dynamic compliance
TV/(PIP-PEEP)
100
This is the equation for alveolar minute ventilation.
RR*(VT - VD)
200
This patient is being ventilated in this mode.
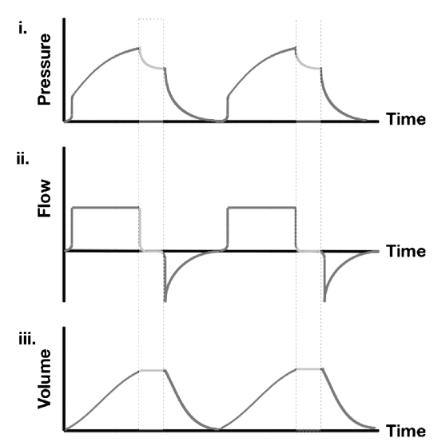
What is volume control?
200
This term describes what change in "B" during an inspiratory pause would indicate:
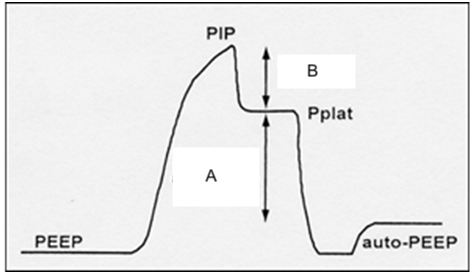
What is resistance?
200
The dotted line in the flow-volume loop indicates this problem.
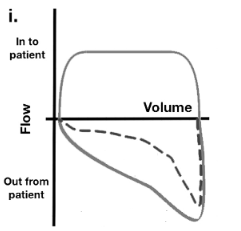
What is scooping, airway obstruction?
200
This is the equation for static compliance
TV/(Pplat-PEEP)
200
The waveform below would prompt you to assess these things:
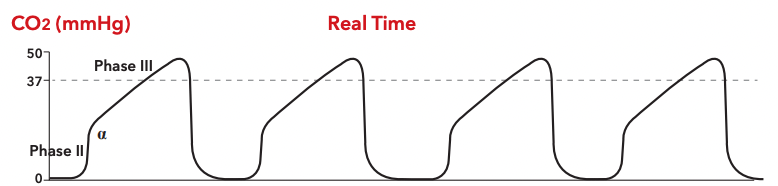
Tube kink or obstruction
Increased airway resistance
300
These are the characteristics of this type of breath.
What is supported?
300
This term describes what a change in "A" during an inspiratory pause would represent.
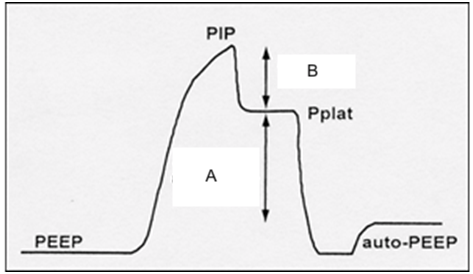
What is compliance?
300
The presence of this abnormality is indicative of overdistension of alveoli due to excessive TV.
What is "beaking"?
300
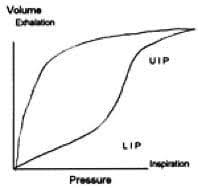
This term describes the phenomenon where the volume of lungs during inhalation is less than during exhalation at the same pressure.
What is hysteresis?
300
These are 2 ways you would troubleshoot a wide ETCO2-PaCO2 gradient on a MV patient
bolus
recruitment maneuver
400
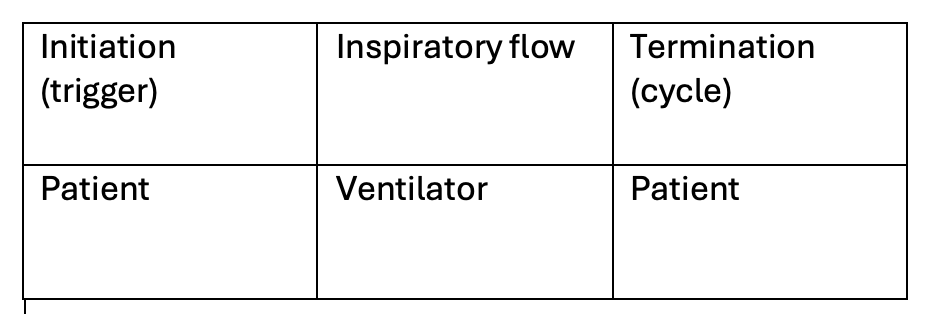
These are the 5 phases of the machine delivered breath.
1. initiation/trigger phase
2. inspiratory flow phase
3. inspiratory pause
4. expiratory flow phase
5. expiratory pause
400
Based on the loop below you would make this change on the MV settings
Increase flow rate
400
The maneuver below is evaluating for this problem

expiratory hold
autoPEEP
400
This equation determines the total pressure needed to generate a ventilator breath and is depicted below:
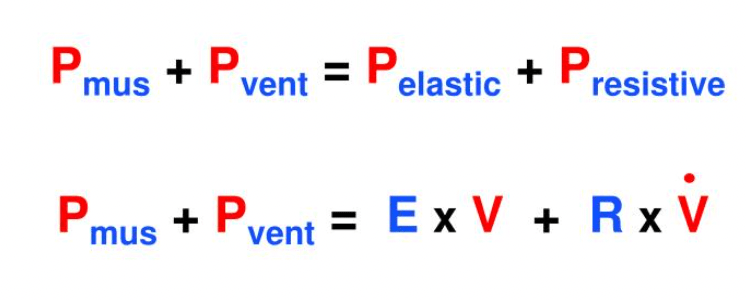
What is the equation of motion?
400
You would assess for this concern if you see the following waveform:
Rebreathing/breath stacking
500
These are 2 ways you can improve recruitment (recruitment maneuvers) in a MV patient
1. reverse I:E
2. high PEEP
3. intermittent high pressure breaths (sigh)
4. stepwise PEEP (ARDSnet)
500
The change in the PV loop below would prompt you to make what changes
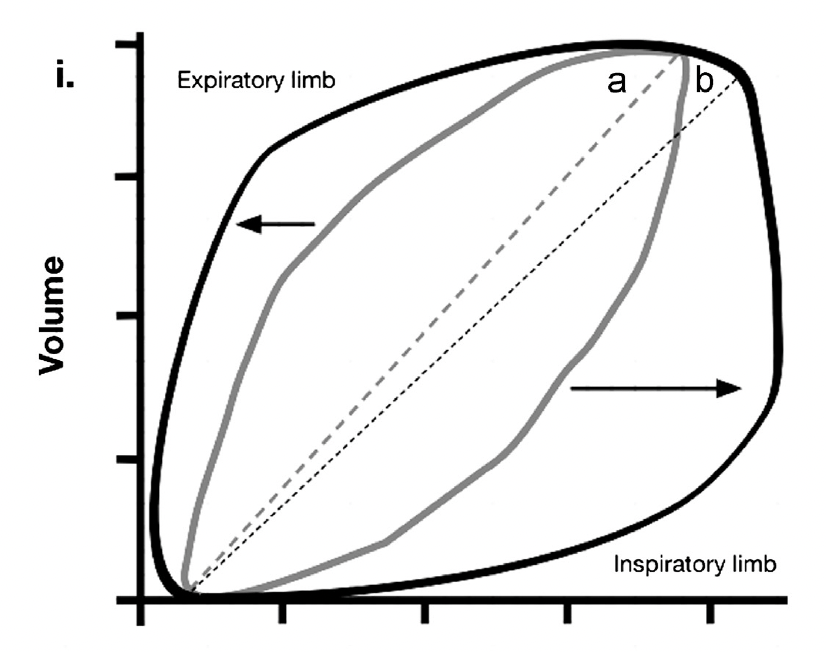
Bronchodilator
Check for ET tube obstruction or moisture in circuit
Suction
500
This waveform would prompt you to assess for:
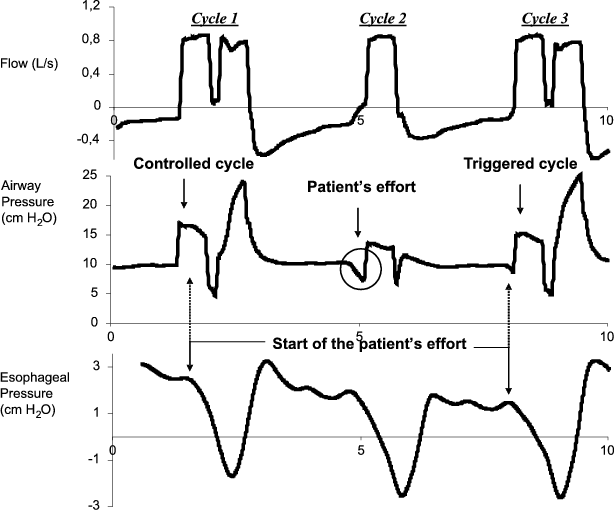
Double triggering
- too low flow or pressure
- increase inspiratory time
- sedate
- decrease trigger sensitivity
500
This is the term for movement or redistribution of gas within the lung without change in tidal volume.
What is pendelluft?
500
This is the value of the V/Q ratio that defines dead space ventilation
What is infinity?