Perilous Presentation
Perplexing Pathophysiology
Diagnostic Dilemmas
Timely Treatment
Spicy Questions :)
100
Upon presentation at the ER, Josiah had faint wheezing on auscultation. Which feature of the immune response is most responsible for this change in airflow?
A. Mast cell degranulation
B. IgE activation
C. Eosinophils resulting in airway remodeling
D. Increased vascular permeability
Answer: A. Mast cell degranulation.
Explanation: Mast cells release immune mediators such as histamine and leukotrienes upon activation by IgE. Histamine and leukotrienes induce bronchoconstriction. Narrowing of the airways produces the wheezing sound heard on auscultation. Eosinophils do cause airway remodeling, which contributes to the pathogenesis of asthma, but is not the primary source of bronchoconstriction. Histamine and leukotrienes do contribute to increased vascular permeability, but this leads to mucus production and edema.
100
Which type of immune cell plays a key role in the inflammatory response in asthma by releasing histamine and leukotrienes?
A. Neutrophils
B. Basophils
C. Mast Cells
D. T lymphocytes
C, Mast cells.
Asthma is a type I hypersensitivity reaction, and in the acute phase of an asthma exacerbation, IgE activates mast cells which release histamine, prostaglandins and leukotrienes. This leads to bronchoconstriction, increased vascular permeability, and mucus production.
100
PaO2, PaCO2 and HCO3- are values found in an arterial blood gas (ABG). What do these values tell us about the status of gas exchange?
A. Diffusion, perfusion, acidity
B. Oxygenation, ventilation, metabolic homeostasis
C. Ventilation, perfusion, pH
D. Oxygenation, diffusion, buffering
Answer: B. Oxygenation, ventilation, metabolic homeostasis.
Explanation: PaO2 assesses the oxygenation status of the arterial blood, while PaCO2 informs us about the ventilation status. HCO3- is an indicator of metabolic balance. In Josiah’s case, we saw a decreased PaO2 due to poor oxygenation. His increased PaCO2 suggests respiratory acidosis, while his HCO3- was normal, which tells us that his body has not started to compensate by inducing metabolic alkalosis via bicarbonate excretion.
PaO2 normal value is between 80-100mmHg. PaCO2 normal value is 35-45mmHg. HCO3- normal value is 22-26 mmol/L.
100
A 7-year-old boy with a history of asthma presents to the emergency department with acute shortness of breath, wheezing, and tachypnea. He is given an inhaled medication that rapidly improves his symptoms. Which of the following best describes the mechanism of action of this medication?
A. Competitive inhibition of leukotriene receptors
B. Inhibition of phospholipase A2, reducing inflammatory cytokine production
C. Activation of β2-adrenergic receptors, leading to bronchodilation
D. Blockade of muscarinic receptors, preventing vagally mediated bronchoconstriction
E. Inhibition of mast cell degranulation, preventing histamine release
Answer: C. Activation of β2-adrenergic receptors, leading to bronchodilation
Albuterol is a short-acting β2-agonist (SABA) that relaxes bronchial smooth muscle by increasing cyclic AMP (cAMP), leading to bronchodilation.
100
Dr. Goff's favorite author
Jane Austin
200
A 54-year-old male with a history of COPD presents for a routine check-up. Wheezing and prolonged expiration is noted on auscultation. A spirometry test shows decreased FEV1 and a reduced FVC, consistent with his diagnosis of COPD. Which of the following best describes the inspiratory-to-expiratory (I/E) ratio in this patient?
A. The I/E ratio is shortened due to increased expiratory time
B. The I/E ratio is prolonged due to increased inspiratory time
C. The I/E ratio is normal
D. The I/E ratio is shortened due to decreased inspiratory time
Answer: A. The I/E ratio is decreased due to increased expiratory time. In a normal patient, I/E ratio may be 1:2. Due to airway obstruction in COPD, the I/E ratio is often decreased as a result of a longer expiratory phase.
200
What is atopy, and how is it related to asthma?
Answer: Atopy refers to a genetic predisposition to develop allergic diseases, including asthma, allergic rhinitis, and atopic dermatitis. It is driven by an exaggerated Th2 immune response, leading to increased IgE production in response to allergens. This IgE binds to mast cells, priming them for degranulation upon allergen exposure, contributing to airway inflammation and hyperresponsiveness in asthma. In our case this week, we saw this as Josiah had a food allergy to peanuts, plaques indicative of atopic dermatitis, and a family history of asthma and allergies.
200
Describe the findings of the following CXR. What does this indicate about respiration?


Answer: Hyperinflation, evidenced by the flattened diaphragm and increased retrosternal airspace. This is not pathognomonic for any specific condition, but is indicative of an obstructive process that volume of air that is expired. This is what was seen on Josiah’s CXR, and is not necessary for diagnosis of asthma, but helpful in excluding other differentials.
200
A 65-year-old man with asthma is prescribed an inhaled medication that blocks muscarinic receptors to prevent bronchoconstriction. Which of the following adverse effects is most likely to occur with this medication?
A. Excessive sweating
B. Oral candidiasis
C. Dry mouth
D. Hyperglycemia
E. QT prolongation
Answer: C. Dry mouth
Ipratropium bromide is a short-acting muscarinic antagonist (SAMA) that prevents bronchoconstriction by blocking vagally mediated pathways. Common adverse effects include dry mouth, urinary retention, and blurred vision due to its anticholinergic properties.
*inhaled IPRA bromide only causes dry mouth
200
Dr. Goff's favorite singer
Taylor Swift
300
An 8-year old child presents to the ER with intermittent episodes of dyspnea and cough. Wheezing is heard on auscultation. Along with allergic rhinitis and a family history of asthma, which skin finding can be seen commonly in asthmatic patients, and what kind of reaction causes this symptom?
A. Erythematous plaques on extensor surfaces, type 1 hypersensitivity
B. Erythematous plaques on flexor surfaces, type 4 hypersensitivity
C. Erythematous plaques on flexor surfaces, type 1 hypersensitivity
D. Erythematous plaques on extensor surfaces, type 4 hypersensitivity
Answer: C. Erythematous plaques on flexor surfaces, type 1 hypersensitivity.
Explanation: This describes the mechanism of atopic dermatitis, one of the features known as the “atopic march”, and is seen in many patients with asthma as a result of IgE hyperreactivity.
Erythematous plaques on extensor surfaces could be descriptive of psoriasis.
Allergic contact dermatitis may be present on any of these surfaces and is a type 4 hypersensitivity reaction.
300
A 19-year-old woman with a history of asthma presents to the emergency department with severe dyspnea, wheezing, and chest tightness after exposure to strong perfume. She is given nebulized albuterol and intravenous corticosteroids, which provide partial relief. She reports experiencing similar episodes several times a year, requiring multiple courses of oral steroids.
Which of the following best describes the primary pathophysiological difference between acute and chronic asthma?
A. Acute asthma is primarily mediated by eosinophils, while chronic asthma is mediated by neutrophils.
B. Acute asthma involves reversible airway obstruction, while chronic asthma can lead to permanent airway remodeling.
C. Acute asthma is caused by direct alveolar damage, whereas chronic asthma leads to restrictive lung disease.
D. Acute asthma is triggered only by allergens, while chronic asthma is triggered only by infections.
E. Acute asthma primarily affects alveoli, whereas chronic asthma affects pulmonary capillaries.
Answer: B
This patient has acute respiratory acidosis (low pH, high PaCO₂, normal HCO₃⁻), which occurs due to alveolar hypoventilation. In severe asthma exacerbations, bronchoconstriction and mucus plugging cause air trapping and increased airway resistance, making it difficult to exhale CO₂. Initially, patients hyperventilate (Josiah had a RR of 40), causing low PaCO₂, but as they tire, their ventilation decreases, leading to CO₂ retention and respiratory acidosis. This is a sign of impending respiratory failure, requiring aggressive intervention such as noninvasive ventilation or intubation.
300
What are 2 histologic findings do you expect in a lung biopsy specimen from a patient with asthma?
Acceptable Answers:
Curschmann spirals - whorled mucus plugs containing shed epithelial cells found in the sputum or bronchioles of patients with asthma or chronic bronchitis
Charcot-Leyden crystals: needle-shaped, eosinophilic crystals composed of eosinophil membrane proteins seen in asthma
Hypertrophy/Hyperplasia of smooth muscle
300
A 21-year-old woman with a history of asthma comes to her primary care physician because of a 3-week history of increased wheezing and associated shortness of breath. She has been using her albuterol inhaler more frequently, including nights, and says that it does not work as well to control her symptoms. A new daily-use inhaled medication is prescribed to control her symptoms, and the patient is advised to rinse her mouth with water after each use of this new agent in order to avoid an oral infection.
Which of the following is the mechanism of action of the most likely medication prescribed?
A.Activates β-adrenergic receptors
B.Inactivates NF-κB
C.Inhibits IgE binding FCeRI
D.Inhibits leukotrienes receptors
E.Inhibits muscarinic receptors
F.Inhibits phosphodiesterase
B. Inactivates NF-κB
This presentation is consistent with mild persistent asthma requiring the addition of a low-dose inhaled corticosteroid. Common adverse effects of inhaled corticosteroids include oral candidiasis, throat irritation, upper respiratory tract infections, and headache. Oral candidiasis can be prevented by rinsing the mouth after inhalation. Corticosteroids act in part by inactivating NF-kB, a transcription factor complex that controls genes involved in immune and inflammation processes. This helps to prevent the inflammatory response that is responsible for acute asthma exacerbations.
300
Dr. Goff's Favorite Breakfast
Lox and bagels
400
A 72-year-old woman with a history of CHF and COPD is admitted to the hospital with worsening dyspnea. On physical examination, RR is 30, and she appears to be using accessory muscles of respiration. Her O2 sat is 88% on room air, and she is noted to have bilateral lower extremity edema. A chest X-ray shows cardiomegaly with pulmonary edema.
Which of the following best describes the increased work of breathing in this patient?
A. Increased inspiratory muscle activity due to reduced lung compliance
B. Decreased work of breathing due to improved chest wall compliance
C. Decreased inspiratory muscle activity due to diaphragmatic fatigue
D. Increased expiratory muscle activity due to airway obstruction
Answer: D. Increased expiratory muscle activity due to airway obstruction
To compensate for the obstruction caused by COPD, she is hyperventilating and using accessory muscles to aid in expiration.
400
A 30-year-old woman with a history of poorly controlled asthma presents to the emergency department with severe dyspnea and accessory muscle use. Her husband, who is accompanying her, is extremely worried about her state. He explains that she has not been feeling the best for a couple of days now, but refused to go to the hospital and instead insisted of following a holistic respiratory meditation guide she found on TikTok to make herself feel better. He finally dragged her in as she was only getting worse. On physical exam, she is found to have pulsus paradoxus, diffuse wheezing, and a hazy mental state. Her arterial blood gas (ABG) is as follows:
pH: 7.18 (7.35-7.45)
PaCO₂: 66 mmHg (35-45 mmHg)
PaO₂: 58 mmHg (75-100 mmHg)
HCO₃⁻: 30 mEq/L (22-26 mEq/L)
Which of the following best explains the underlying pathophysiology of her acid-base disturbance?
A. Respiratory muscle fatigue leading to acute respiratory acidosis with metabolic compensation
B. Hyperventilation causing a mixed respiratory alkalosis and metabolic acidosis
C. Increased CO₂ diffusion due to alveolar hyperperfusion leading to a primary metabolic acidosis
D. Excessive β-agonist use leading to hypokalemia-induced metabolic alkalosis
E. Anion gap metabolic acidosis due to increased lactic acid production
Answer: A. Respiratory muscle fatigue leading to acute respiratory acidosis with metabolic compensation.
In early asthma exacerbations (seen with Josiah), patients hyperventilate, and as airway resistance worsens over time (in this case many days) air trapping and respiratory muscle fatigue develop causing hypoventilation and CO2 retention, worsening respiratory acidosis with clear metabolic compensation seen.
400
A 65-year-old man presents to the clinic with progressive dyspnea, chronic cough, and occasional wheezing for the past five years. He reports a 40-pack-year smoking history. Spirometry reveals a FEV₁/FVC ratio of 65%, which does not significantly improve after administration of an inhaled bronchodilator.
Which of the following findings would best differentiate chronic obstructive pulmonary disease (COPD) from asthma in this patient?
A. Increased total lung capacity (TLC)
B. Increased diffusing capacity for carbon monoxide (DLCO)
C. Irreversible airflow obstruction on spirometry
D. Eosinophilic infiltration of the airway
E. Intermittent symptoms triggered by allergens
Answer: C
COPD is characterized by persistent, irreversible airflow obstruction, primarily due to emphysema (alveolar destruction) and chronic bronchitis (mucus overproduction). Bronchodilator testing typically shows little or no improvement in FEV₁.
Asthma, in contrast, is reversible with bronchodilators. An increase in FEV₁ by ≥12% and ≥200 mL after bronchodilator administration confirms asthma. In Josiah’s case, his FEV1/FVC ratio became normal after bronchodilatory treatment!
400
A 50-year-old man with a history of hypertension, hyperlipidemia, and asthma presents to the clinic for follow-up. He is currently taking albuterol as needed, fluticasone daily, atorvastatin, and metoprolol for hypertension. He reports worsening shortness of breath despite frequent albuterol use. What is the most likely explanation for his worsening symptoms?
A. Atorvastatin-induced myopathy leading to decreased respiratory effort
B. Fluticasone-induced adrenal suppression
C. Metoprolol antagonism of β2-receptors, reducing albuterol efficacy
D. Albuterol-induced hypokalemia worsening respiratory muscle function
E. Development of steroid resistance due to chronic fluticasone use
Answer: C. Metoprolol antagonism of β2-receptors, reducing albuterol efficacy
Beta-blockers (especially non-selective ones like propranolol) can reduce the bronchodilatory effects of β2-agonists. Although metoprolol is β1-selective, at higher doses it can still have some β2-blocking effects, potentially worsening asthma symptoms.
400
Dr. Goff's Favorite dog
OP
500
A 45-year-old woman with a history of asthma presents to the emergency department with worsening shortness of breath, wheezing, and cough over the past 2 days. On physical examination, her blood pressure is 130/80 mmHg while at rest. However, during inspiration, her systolic blood pressure drops to 90 mmHg. Her respiratory rate is elevated, and she is using accessory muscles of respiration. A peak flow measurement shows significant airflow obstruction. This blood pressure finding can be seen as a result of obstructive pulmonary disease, due to significant negative intrathoracic pressure during inspiration leading to impaired left ventricular filling. What other conditions can cause a similar change in blood pressure?
A. Cardiac tamponade
B. Restrictive pericarditis
C. Sarcoidosis
D. Pulmonary hypertension
Answer: A. Cardiac tamponade
The finding of a significant decrease in systolic blood pressure during inspiration, known as pulsus paradoxus, is often observed in conditions that increase intrathoracic pressure, such as severe asthma exacerbations, compression of the heart by cardiac tamponade or constrictive pericarditis. Obstruction of the airways requires more negative pressure in order to draw air into the lungs. During inspiration, the increased negative pressure in the thoracic cavity causes an increase in venous return. The increased filling of the RV causes it to expand into the LV, thereby reducing LV filling. This leads to a greater drop in systolic blood pressure during inspiration. In severe asthma, the combination of bronchoconstriction and increased respiratory effort causes an exaggerated intrathoracic pressure change, resulting in pulsus paradoxus.
500
A 64-year-old man is brought to the ER after being found unresponsive by his wife. She says he was in his usual state of health when she left home a few hours ago. The patient has a history of bipolar disorder and type 2 diabetes mellitus. Blood pressure is 100/60 mm Hg and pulse is 64/min. Arterial blood gas analysis reveals the following:
pH: 7.22
PaCO2: 60 mm Hg (35-45 mmHg)
HCO3-: 24 (22-26 mEq/L)
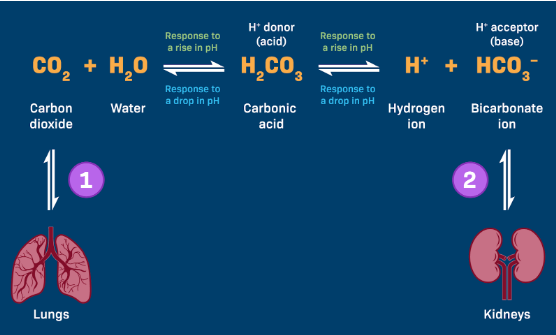
The diagram on the board the bicarbonate buffer reaction and explain how the reaction is shifting with this patient's state. Include discussions of both his respiratory and metabolic state in your answer.
This patient is in a state of respiratory acidosis without metabolic compensation. The increased CO2 will push the reaction to the right and increase the hydrogen ion concentration which is directly reflected by the pH. Because of the acute nature of this patient's condition, the body has not had an opportunity to metabolically compensate by increasing renal excretion of hydrogen and reabsorption of bicarbonate.
500
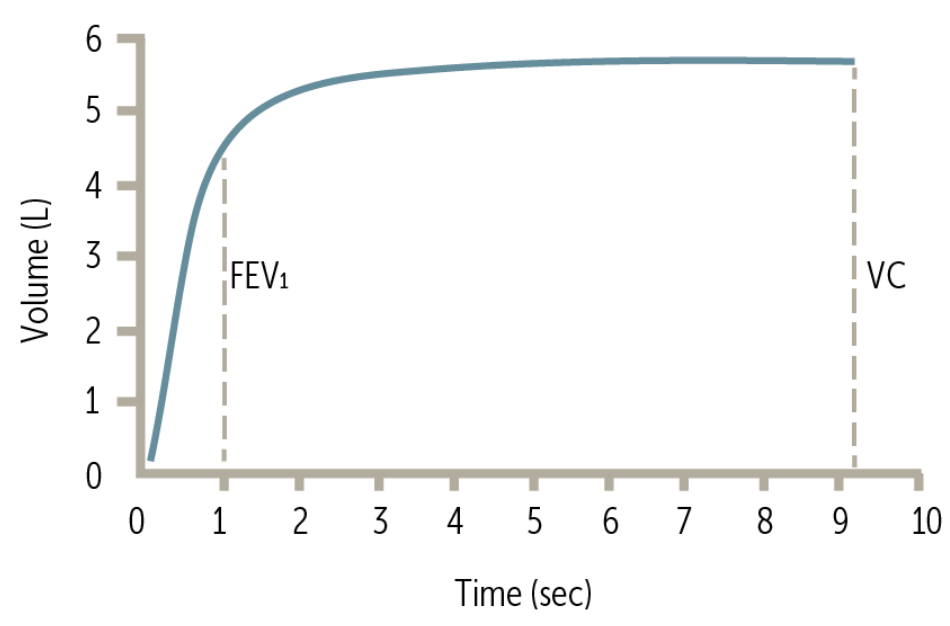
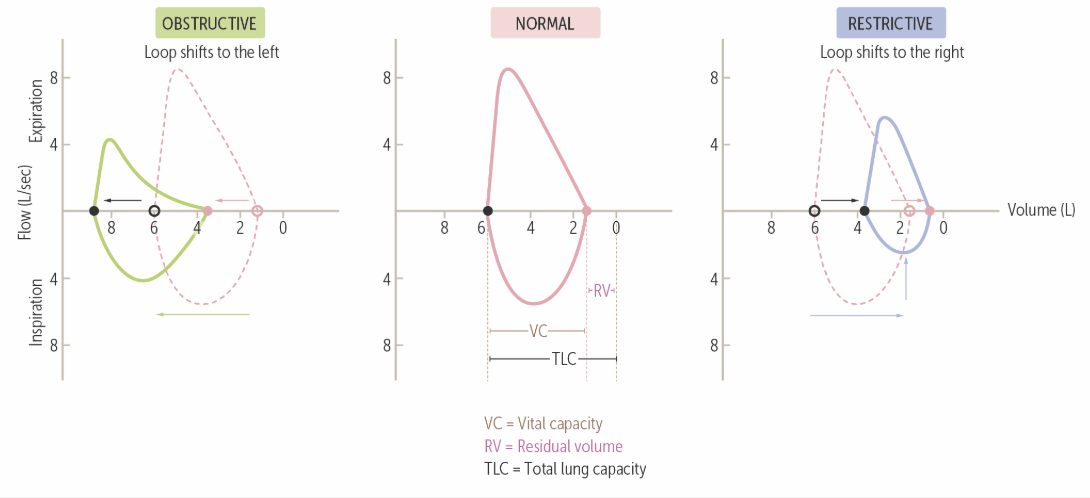
Compare and contrast a normal time-volume graph and a flow volume loop with those that would reflect Josiah’s condition when he initially presented and explain what is happening through the use of the whiteboard. Additionally, explain how they change with medication.
Josiah presented with an acute exacerbation of obstructive lung disease, which would shift time-volume curves down and flow-volume curves to the left. Additionally, an initial peak in expiratory volume would be accompanied by a rapid decline as obstructive lung diseases decrease expiration. Medications would shift these curves back to normal as the FEV1/FVC is corrected
500
A 10-year-old boy with a history of asthma presents with worsening shortness of breath and wheezing over the past hour. His mother states he has been compliant with his daily medications, which include fluticasone and montelukast. In the emergency department, he is unable to speak in full sentences, has intercostal retractions, and has an oxygen saturation of 89% on room air. Which of the following is the most appropriate next step in management?
A. Increase the dose of fluticasone
B. Administer inhaled albuterol and ipratropium, plus systemic corticosteroids
C. Initiate leukotriene receptor antagonist therapy
D. Administer inhaled albuterol and ipratropium
E. Administer inhaled albuterol and systemic corticosteroids
Answer: B. Administer inhaled albuterol and ipratropium, plus systemic corticosteroids
This is an acute asthma exacerbation requiring immediate bronchodilation with inhaled short-acting β2-agonists (albuterol) and muscarinic antagonists (ipratropium), plus systemic corticosteroids (prednisolone) to reduce airway inflammation. Chronic medications (e.g., fluticasone, montelukast) do not provide rapid relief and should not be adjusted during an acute attack.
500
Dr. Goff's Favorite place
Possum Kingdom