<3 :(
Too much T4
Uh-Oh! A Rash!
Ouch sans Opioids
Hi Dad
100
Iron deficiency is present in __% of people with HFrEF regardless of presence of anemia
40-60%
22% to 25% reduction in heart failure hospitalization in patients receiving intravenous iron replacement compared with usual care, with no effect on all-cause mortality
100
Name common causes of hyperthyroidism
1. Graves
2. Toxic multinodular goiter
3. Toxic adenoma
4. Thyroiditis
100

Name that rash!
Seborrheic Dermatitis
100
This is first line treatment for chronic pain related to hand and knee OA
topical NSAIDs (50% reduction in pain, NNT 10 vs 7 based on med)
Followed by oral NSAIDs
Followed by duloxetine (50% improvement, NNT =6)
100
What is the incidence of venous stasis ulcer in adults?
1-3%
200
What are the indications for initiation of GDMT?
* bonus: what is the impact of GDMT on all cause mortality?
- EF <40%
- Symptomatic (class C or D AHA or class II - IV NYHA)
* reduction by 61%, this is added on ~7.9yrs to a 50 yo life span
200
These are common symptoms of hyperthyroidism
weakness, palpitations, weight loss, and heat intolerance, and the most common signs are a palpable goiter, tachycardia, muscle weakness, and tremor
- folks >60 yo less likely to have symptoms, more likely to have afib
- folks with subclinical hyperthyroidism can experience symptoms and are still at risk for complications like cardiovascular mortality, atrial fibrillation, and decreased bone mineral density
200
Describe the common findings of seborrheic dermatitis on physical exam
symmetric, poorly defined erythematous patches with yellow, oily scales and fine, superficial desquamation.
in folks with darker skin, erythema may be similar or less noticeable, and postinflammatory pigmentary changes can be a key presenting feature and must be distinguished from other skin disorder than can cause hypopigmentation (pityriasis alba). May also have a more localized/annular presentation on hairline/face known as petaloid seborrhea
predominantly areas rich in sebaceous glands, include the scalp (colloquially dandruff), face, chest, intertriginous areas (eg, skin folds such as the groin, axillae, and inframammary folds), nasolabial folds, upper eyebrows, and the nasal bridge
200
For treatment of chronic lower back pain this class of medication is the only one shown to have effect on pain and disability for >few weeks.
NSAIDs. topical or oral. in a 3-12 mo time frame.
*SNRIs, muscle relaxers, gabapentnoids/AEDs, TCAs, all with some evidence (low-mod quality) about having little to no impact on pain or disability.
:'(
200
There are ____ types of generally available compression over the counter/commercially
3! Light, medium, heavy
light (15–20 mm Hg), medium (ie, 20–30 mm Hg), and heavy (ie, 30–40 mm Hg)
300
True or false: ARBs have less of a mortality benefit than ACEi
True, 20% to 30% reduction in all-cause mortality
----------------------------------------
Recommended to start if ACEi intolerable due to side effects.
Best benefit/first line: entresto (NNT 32 or 36, ARR of 3.2 or 2.8%). Start when congested during hospitalization. 36hr washout if on other ACE.
If they don't tolerate this class start isosorbide dinitrate and hydralazine.
300
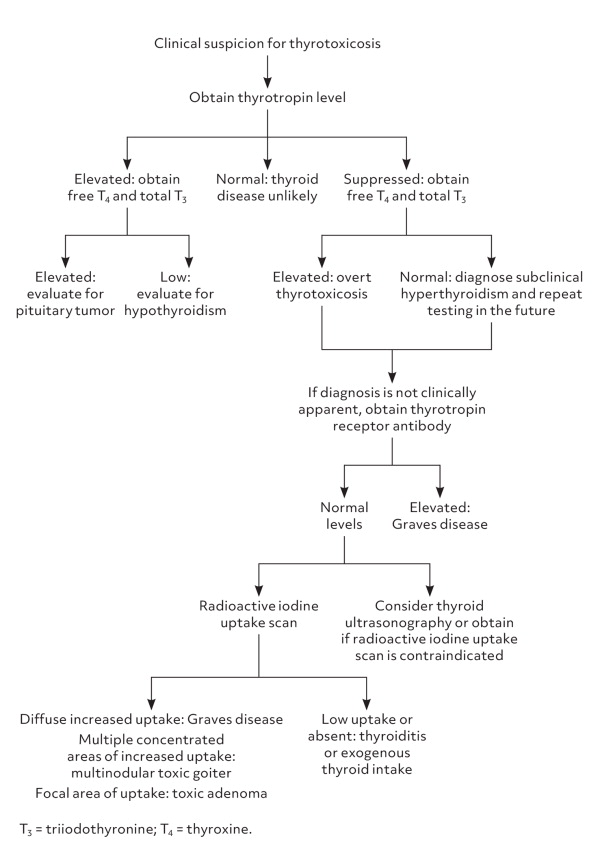
Describe the diagnostic process when you have a suppressed TSH
1. obtain free T4, total T3
2. if both elevated and clinically c/w Graves ---> treat
3. if unclear etiology still ---> obtain thyrotropin receptor antibodies
4. If normal ---> radioactive iodine uptake scan vs thyroid US if uptake scan contraindicated
300
Pathophysiology of seborrheic dermatitis is thought to be 3-fold:
1. overgrowth of _____
2. disruption of _____
3. dysregulated inflammatory response
1. Malassezia yeast species
2. epidermal skin barrier
300
Gabapentin at dosages of ____ mg/day or greater leads to at least moderate benefit in neuropathic pain.
Pregabalin at dosages of ___ mg/day or greater leads to at least moderate benefit compared with placebo
duloxetine ___ mg/day
1,200 (NNT 5-7)
300 (NNT 4-22) (NNH 7-35)
60 (NNT 5)
Studies based primarily on post-herpetic neuralgia and diabetic neuropathy pain
300
Compression is both a mainstay of ____ and _____ for venous stasis ulcers.
Treatment and prevention of recurrence
400
1. beta blockers provide _______ improvements in mortality and left ventricular ejection fraction.
2. If admitted for first time HF exacerbation beta blockers should be started when?
3. Beta blockers ______ be continued during acute heart failure exacerbation.
4. Initiation and titration, some patients may develop ________ heart failure symptoms
1. dose-dependent
2. after adequate diuresis
3. can! If held they should be re-started on discharge
4. transient worsening
Odds ratio for mortality reduction with treatment compared with placebo was 0.69 (95% CI, 0.56–0.80) - meta analysis
400
Methimazole is preferred over propylthiouracil to reduce the risk of hepatotoxicity associated with propylthiouracil, except in these patients:
- during the first trimester of pregnancy
- in thyroid storm
- in patients with adverse reactions to methimazole
Dosing guided by initial T4 concentration.
Guidance provided on signs of agranulocytosis, hepatotoxicity.
18mo therapy can achieve euthyroid state in 40-50% of patients. TFTs should be monitored q4-6wks after initiation of meds. Consider switching to RAI or surgery if not in remission 12-24mo after initiation of therapy.
400
This is standard treatment for cradle cap!
oops.. no real agreed upon "standard"
Typically for mild-mod cases it is use of barrier/emollient to soften scales before brushing them away.
For severe/inflammatory cases can use low potency topical steroid w/ topical antifungal (e.g 0.025% triamcinolone w/ ketoconazole). Could also consider shampoos.
400
These three medications have the best evidence for treatment of fibromyalgia
- pregabalin - pain reduction by 30-50%; NNT 7-14
- duloxetine
- milnacipran
30% pain reduction (NNT of 10); low-quality evidence
400
This level is the most effective level of compression.
Heavy!
Studies show ARR 24.7%; 95% CI, 11.0%–33.4%; number needed to treat [NNT] = 5; when compared to no compression.
However NNH of 14 due to risk of withdrawal from treatment.
500
Goal is to start all therapies within ____ timeframe to decrease 180d all cause mortality.
If unable to start all simultaneously, start ___ and ___ first to decrease risk of sudden death and readmission risk. Then add on ____ in 1-2 weeks, then ____ in another 1-2 weeks.
Someone is persistently symptomatic. Now what?
6 week.
BB and SGLT2.
ACEi vs ARB/neprolysin
MRA inhibitor
Titrate to max tolerated doses. Then likely will need referral to cards, however:
- digoxin
- ivabridine
- Isosorbide dinitrate and hydralazine
- Vericiguat (Verquvo), an oral soluble guanylyl cyclase stimulator promoting vasodilation and myocardial remodeling
500
Radioactive iodine is first line treatment for patients with ____ and ___.
____ develops post-RAI in 86% of patients who had Graves and 34% of patients who had multinodular goiter.
Toxic multinodular goiter, toxic adenoma.
Hypothyroidism
*RAI can exacerbate thyroid eye disease, can be mitigated with steroid pre-treatment
500
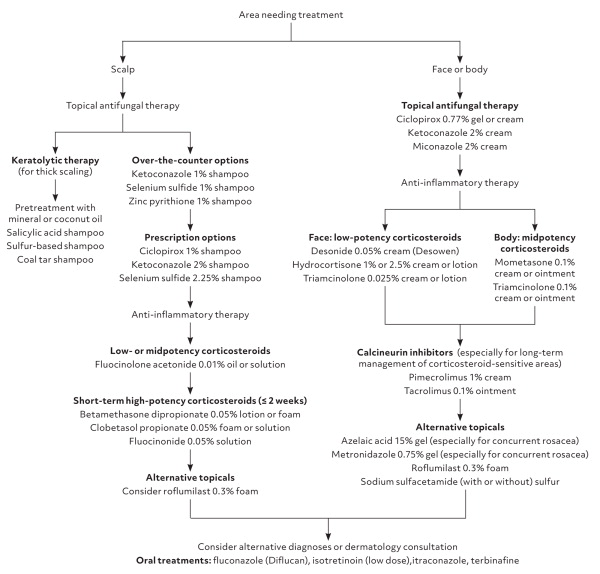
Discuss treatment options for different locations of seborrheic dermatitis
500
So what the heck, this feels hopeless? Are you supposed to use opioids?
Woah there... Try anyway :)
500
Clinicians should ensure adequate _______ as needed when using compression therapy to evaluate and treat leg ulcers
arterial circulation with pulse examination or vascular studies