Statin Alive on April Fool’s
Oops! All Frailty
Pheo or Faux?
Light Chains, Heavy Lies
Pop Culture ft Dr. Harpalani
100
What lab should be sent on all patients at least once in their life that is new in the 2026 dyslipidemia guidelines?
Lp(a)
Unique "tail" is structurally almost identical to plasminogen without function of plasminogen
Results in decreased fibrinolysis
Highly hereditary
Stable levels over lifetime
100
What criteria must be met for a patient to qualify for inpatient hospice?
Terminal illness prognosis < 6 months
Severe, uncontrolled symptoms that cannot be safely managed at home hospice, assisted living or nursing facility - uncontrolled pain, dyspnea, intractable N/V etc.
100
In a patient with granulomatous disease that is affecting their calcium, what would you expect their workup to show regarding
PTH
25(OH) Vit D
1,25-(OH) Vit D
Low PTH, low 25-(OH) Vit D and high 1,25-(OH)
Sarcoidosis classically, also fungal infections, TB, lymphoma
100
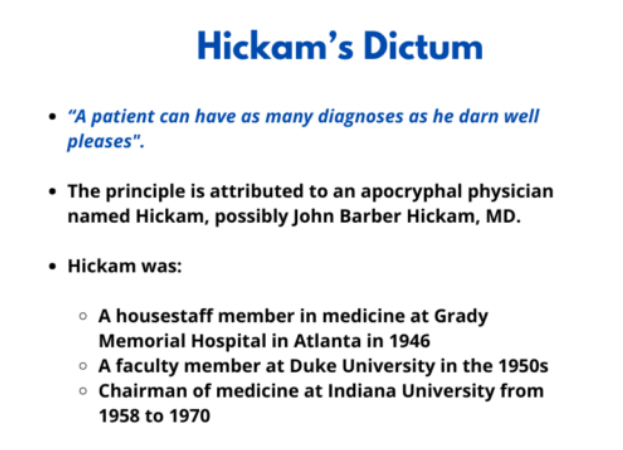
What is Hickam's Dictum
100
Which golf star was recently arrested for a DUI?
Tiger Woods
200
Patients with what 3 comorbid conditions (not ASCVD) should be started on statins regardless of PREVENT score.
HIV
CKD 3+, though limited evidence to support in ESRD unless established ASCVD.
TIIDM
200
What medication can be used to reverse opiod-related constipation? Why does it not worsen pain?
Methylnaltrexone - avoid in suspected bowel obstruction
Also nalexogal, naldemedine
They are designed to not cross the blood-brain barrier, and therefore do not worsen pain - either large attached molecule or extreme charge
200
What are considered first-line therapies for TIIDM?
Metformin - classic example, but increasingly favoring starting medications based on comorbidities
GLP if ASCVD, overweight
SGLT2 if ASCVD, CKD, HF
Insulin if A1c > 10%
200
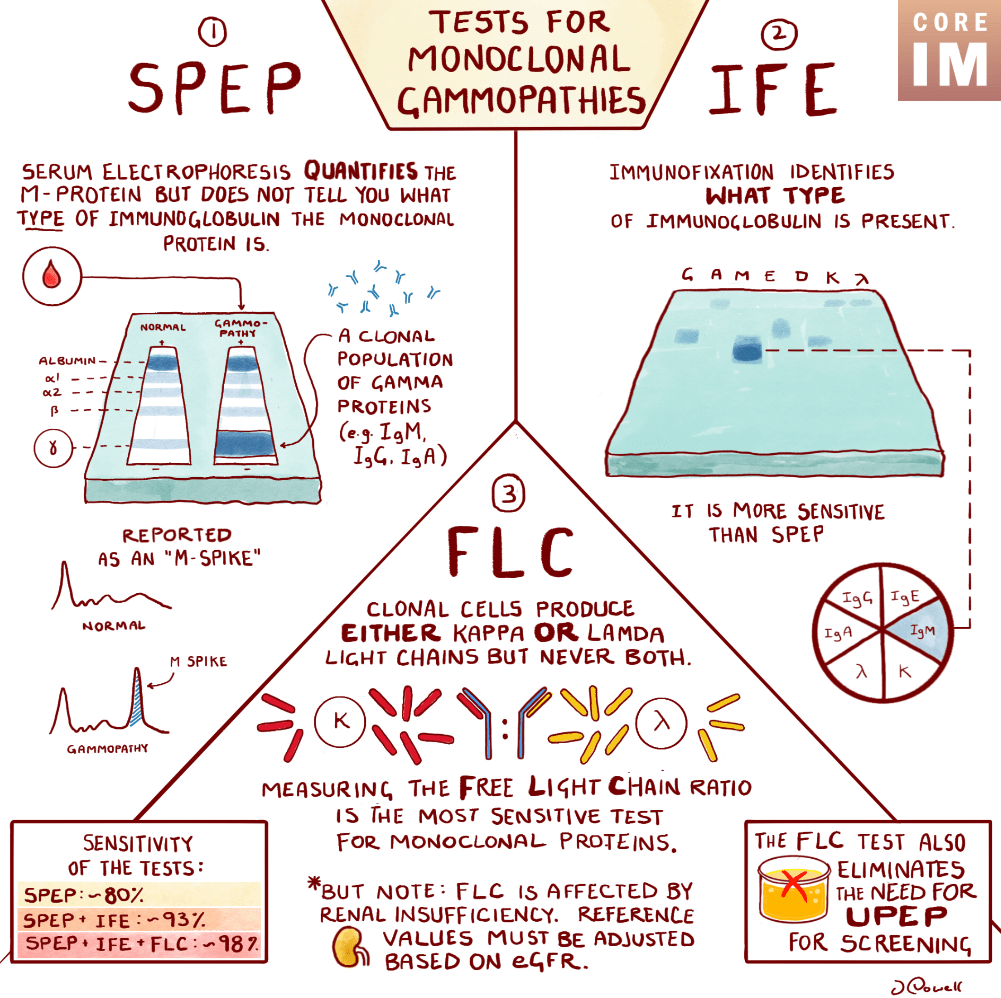
What are the three lab tests used to work up a protein gap, and what is each designed to detect?
200
Which iconic Disney show just had their 20th season reunion?
Hannah Montana

300
At what level of LDL should you consider starting a statin, even if a patient's PREVENT score is <3%?
>160 (2A), DEFINITELY for > 190 (1)
300
What is the most common cause of chronic cough?
>8 weeks duration, most often caused by upper airway cough syndrome (UACS), formerly known as post-nasal drip
Management include intranasal corticosteroids + antihistamines
300
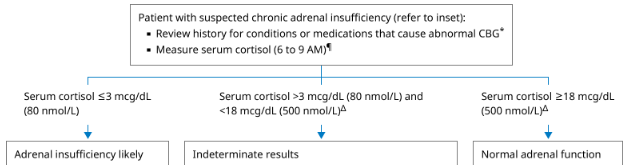
What are the thresholds for an absolute diagnosis, likely diagnosis and a rule out of Adrenal insufficiency for cortisol level? How must it be drawn?
< 3 absolute, <5 likely, ruled out if >15 (some say 18)
6-9 AM
300
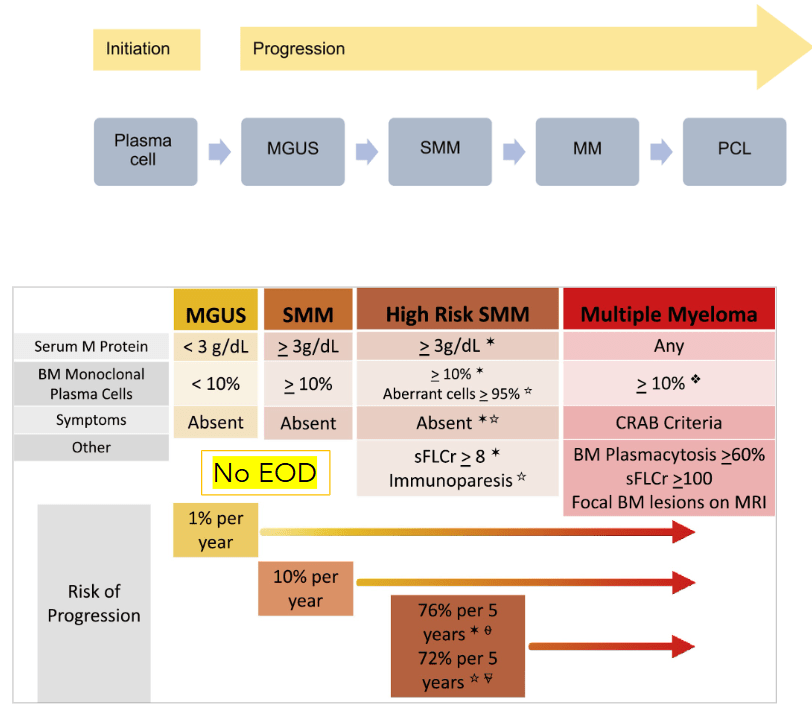
Define categories of MM spectrum regarding their levels of Serum M protein, % monoclonal plasma cells, and symptoms.
Monoclonal gammopathy of undetermined significance
Smoldering multiple myeloma
Multiple myeloma
300
What shade of blue did Anne Hathaway wear to kick of Devils Wear Prada 2 filming (also an iconic line in the movie)?
Cerulean blue
"But what you don't know is that that sweater is not just blue. It's not turquoise. It's not lapis. It's actually cerulean. "

400
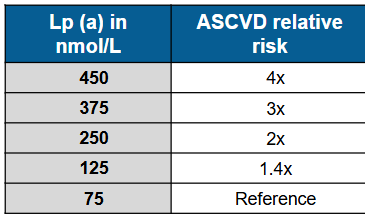
What is the lowest CAC score on coronary CT angiogram that is associated with an increased risk of ASCVD?
1-100 confers 4x risk ASCVD when compared with 0
If >0 but < 1 there is no clear guidance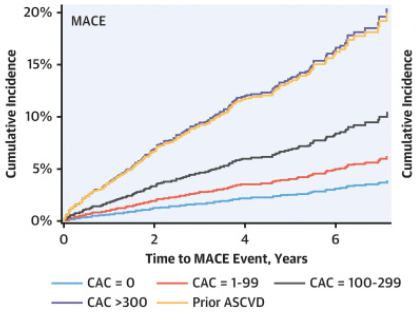
400
What is first line treatment for insomnia?
Name 2 medication classes FDA approved for insomnia.
CBTi
Nonbenzodiazepine sedative-hypnotics (zolpidem, zaleplon, and eszopiclone - less preferred, but often used), dual orexin receptor antagonists (suvorexant and daridoexant) and low-dose doxepin (TCA).
400
33M PMH Graves disease presents with tremors, palpitations, exertional dyspnea, and N/V 1 month after being unable to get refills of his methimazole. T 104F HR 124 BP 164/94 with Irr/Irr tachycardia, bibasilar rales, lid lag, tremor and delirium on physical exam. Labs show elevated LFTs and signs evidence of thyrotoxicosis on bloodwork. CXR shows pulmonary edema.
Identify 4 first-line classes of medications that should be utilized for the management of this patient’s underlying diagnosis
Beta-blocker → thionamide → iodine → steroids
1) Nonselective beta-blockers -Propranolol (or esmolol)
- Controls adrenergic symptoms (HR, tremor), ↓ T4 → T3 conversion
2) Thionamides (Propylthiouracil or Methimazole)
- PTU preferred in thyroid storm because it blocks secretion and also ↓ T4 → T3 conversion
3) Iodine (after thionamide!)
- Blocks release of preformed thyroid hormone (Wolff-Chaikoff effect) - given ≥1 hour after thionamide to avoid fueling synthesis
4) Glucocorticoids - Hydrocortisone
- ↓ T4 → T3 conversion, Treats possible relative adrenal insufficiency
400
Name 3 clinical complications/diagnoses that are seen in Waldenstrom's macroglobulinemia that are rarely seen in multiple myeloma.
Hepatomegally, splenomegally + LAD - behaves more like lymphoma then myeloma - lymphoplasmacytic lymphoma
Hyperviscosity - IgM particle size much higher risk
Peripheral neuropathy - anti-MAG antibody can cause demyelination
Cryoglobulinemia - Type 1 IgM fixes complement
Cold agglutinin disease - IgM can bind RBC's at low temps -> lacelike rash
Aqcuired von Willibrand syndrome
MYD88 mutation in 90+%
Absence of lytic bone lesions/hypercalcemia
400
Which mom from Secret Lives of Mormon Wives just had her season of the bachelorette cancelled, and why?
Taylor Frankie Paul
And a video of a domestic violence dispute from 2023 resurfaced.

500
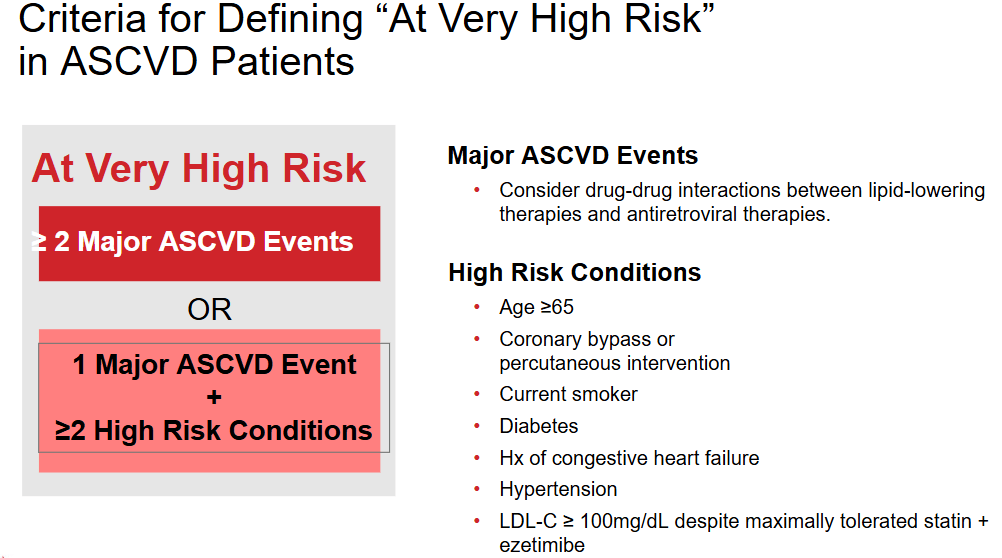
How do the 2026 guidelines define patients that are at "very high risk" of ASCVD?
Target LDL < 55 and Non-HDL-C < 85. Can consider ApoB goals if those are reached.
500
Convert 2 mg IV and 2 mg PO dilaudid to PO morphine.
2 mg IV x20 = 40 mg PO morphine
2 mg PO x4 = 8 mg PO morphine

500
AASLD recommends all patients diagnosed with cirrhosis should be screened for this endocrine disease at diagnosis and every 2-3 years following.
Osteoporosis (hepatic osteodystrophy)
30-50% of patients with cirrhosis have osteopenia/porosis, and they have increased fracture risk. Driven primarily by decreased hepatic IGF-1, but also vit D def, hypogonad, inflammation, alcohol use.
500
Define monoclonal gammopathy of clinical significance
Clone of plasma cells secrete immunoglobulins that have paraneoplastic properties - they are functioning proteins, but NOT meeting criteria for MM - (<10% in marrow, no plasmacytoma)
Can cause nephropathy or many skin disorders. Also POEMS (polyneuropathy, organomegaly, endocrinopathy, m spike, skin changes), DADSM (Distal acquired demyelinating syndrome with M Protein)
500
Which two bravo-lebrities just announced their relationship this week?
Amanda Batula and West Wilson
