CHD Things
Unit Policies/ Procedures
X RAYS
Vent/ ABGs
Arrythmias And Treatments
100
What is a big concern (hemodynamically) for patient's s/p repair of coarctation of the aorta?
Why is this a big concern to the physicians?
Paradoxical HTN
LV is used to having to use lots of force to adequately provide for the body through the coractation- when repaired, the LV has to "re-learn" that it doesn't need as much force. Thus can cause HTN. Will self correct over time.
Can pop sutures/ tamponade!
100
How do you TPA a occluded port?
Pre-measure TPA volume for your line!
Stopcock with TPA> pull back on empty syringe and rotate stopcock while aspirating, line should pull in TPA
100
What do you see in this xray?

Pleural effusion
100
How can you tell if your ETT is in the correct spot without touching the patient?
ETCO2
TV
SPO2
100

SVT
Vagal Manuvers
Adenosine
Synchronized Cardioversion
200
Your patient is a post op day 4 VSD repair. 4 month old. Intubated.
Your patient alarms. These are the vitals- what is your course of action.
HR 60, BP 60/30, SPO2 70, ETCO2 60
Yell for help/ push staff assist.
Support ventilation first! Bag or manual breaths. Provide supp fio2.
What do you think happened to this patient?
200
Your patient is 3 months old, has a PIV, a single lumen power PICC and a g tube.
Does your patient get a CHG bath? What about this patient indicates that they get a chg?
Yes!
Central Line
Older than 2 month!
200
What is wrong with this Xray?

ETT is right mainstem
ETT should be between 2nd and 4th intercostal space
200
VBG on 2 Ventricle Patient - SpO2 95
Oxyhbg- 45
AVO2 difference is 50 (Norm 20-40)
High is indication of high consumption of O2. Can be indication of low cardiac output.
Causes of low SVO2- low hgb (less carrying capacity), SaO2 is low.
Treatment- supportive and treat cause if treatable.
200

Junctional
Symptomatic or Asymptomatic
Sedation
Electrolytes (Magnesium!)
Keep Cool 36-37
Override pace if wires are present
Meds: Precedex, Amiodarone (Give CaCl prior), procanamide, esmolol
300
What is the flow of blood through the heart of a hlhs patient s/p hybrid?
IVC/ SVC > RA> RV & LA (Through asd)> PA's > lungs & through PDA to body
300
It is a Tuesday. Your patient has a right IJ TL.
Upon initial assessment, the TL dressing is peeling up and the port is exposed partially.
Does this dressing need to be changed?
Change the dressing
Dressing are Q 7 days, on Sundays ideally
BUT CHANGE if not occlusive.
If still occlusive but starting to peel you may secure with additional dressing.
300
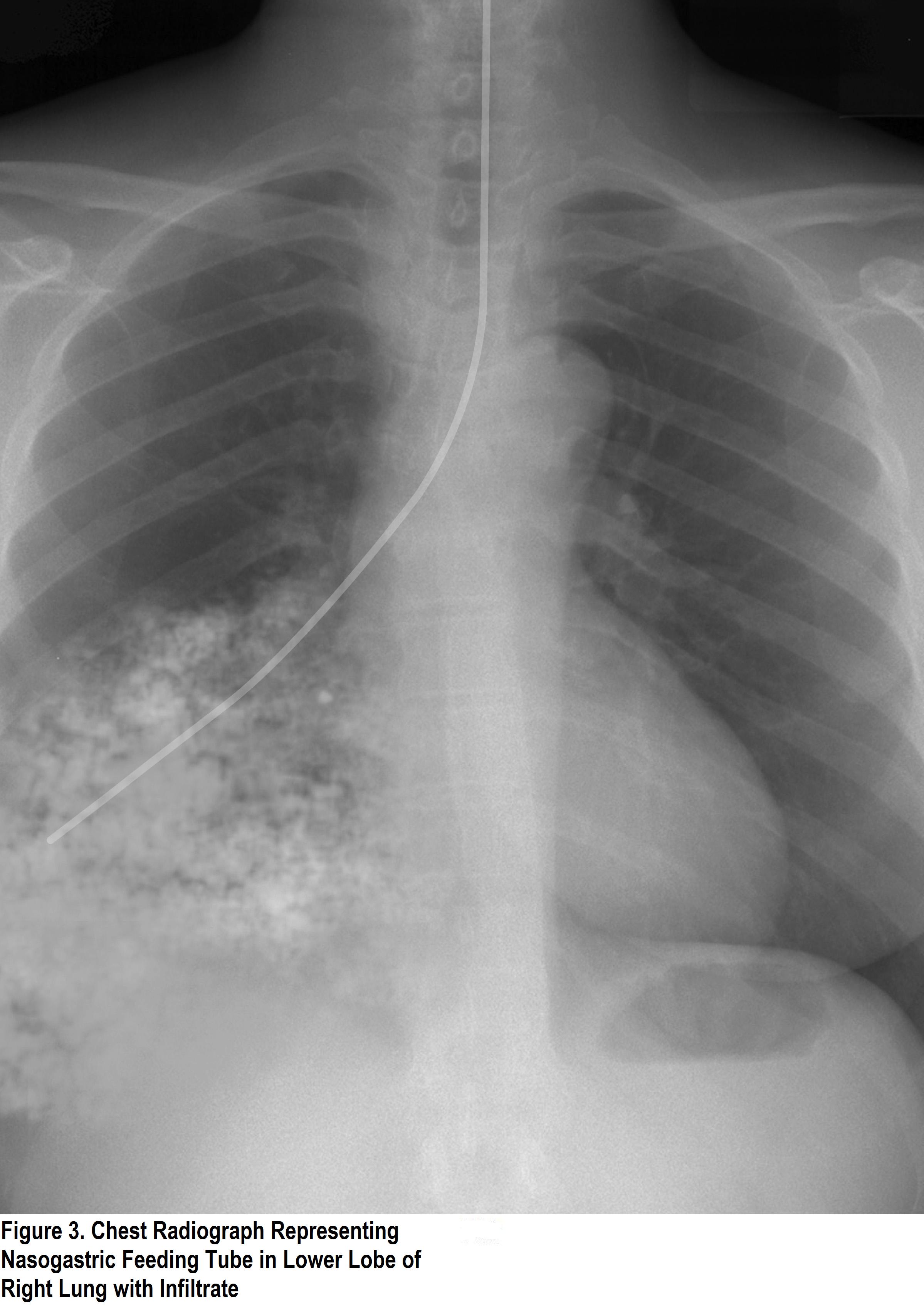
NG tube is in lungs
300
How can you adjust a patient's CO2 on a ventilated patient?
Goal
Lower CO2- increase the rate OR increase the TV (on volume control you can choose a tv) on pressure control you can provide additional support/ pressure
Raise CO2- wean rate/ sedate patient breathing over rate, decrease pressure/ TV
300
V Tach
Runs vs Sustained?
CPR/ Defibrillate
Amio or Lidocaine
Electrolyte replacement if stable?
400
What are the 3 (or 4) stages of repair of a hypoplastic LH patient?
Hybrid
Norwood
Glenn
Fontan
400
How often should caps/ microclaves at the end of a central line be changed?
every 4 days! same as the tubing!
400

Pneumothorax L Side
Pneumos have no lung markings, only air which appears dark on xray.
400
Interpret this ABG
7.56/26/70/30/-1
Ventilated patient. What is your intervention?
Respiratory alkalosis
Patient is being over-ventilated
Wean rate/ give sedation.
400
 HR = 190
HR = 190
Sinus Tachycardia
Treat cause!
Causes: Irritability, hypovolemia, hyperthermia, sepsis, heart failure, hypoxia
Tamponade?
500
Why can't a single Ventricle (mixer) patient cry for a long time?
"Cry or die" physiology
500
How often do we change our arterial line dressings?
As needed!
500

What congenital heart defect has this boot shaped xray? Why?
Tetralogy of fallot - RV hypertrophy!
500
How would you interpret this gas? What treatment would you expect for a gas like this? What probably caused it?
7.53/40/80/38/+9
Metabolic Alkalosis
What treatment? Diamox or wean diuretics
Cause: Lasix/ hypovolemia
500
HR 80
Patient 5m 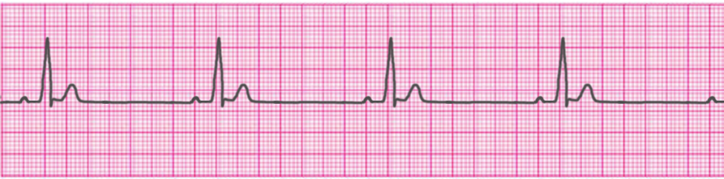
Sinus Bradycardia
Pacing if wires present!
Epinephrine or Atropine if symptomatic
Treat underlying cause- did patient vagal? Hypothermia?