What's the SKINny on that rash?
Derm Infections
Creams! Ointments! Emollients! Oh My!
A RanDERM Category
This potpourri category is so CUTEaneous
100
Name 3 features of classic eczema and the area(s) of the body most commonly affected in adults
1) Pruritis
2) Dry Skin
3) Erythematous papules (acute)
4) Dry and scaly erythematous papules (chronic)
location - in adults, skin flexures are commonly involved in addition to face, neck, or hands
100
Name this condition and how you decide on treatment

This is HSV! note grouped vesicles on an erythematous base.
-Oral lesions can be on the vermillion border or the buccal mucosa.
-Don't forget that genital HSV can involve the glute as well
primary infection may involve more prolonged treatment but we usually see recurrent infection! goal to start treatment ASAP (give refills!) - can be acyclovir or VALacyclovir but acyclovir is more frequent dosing!
100
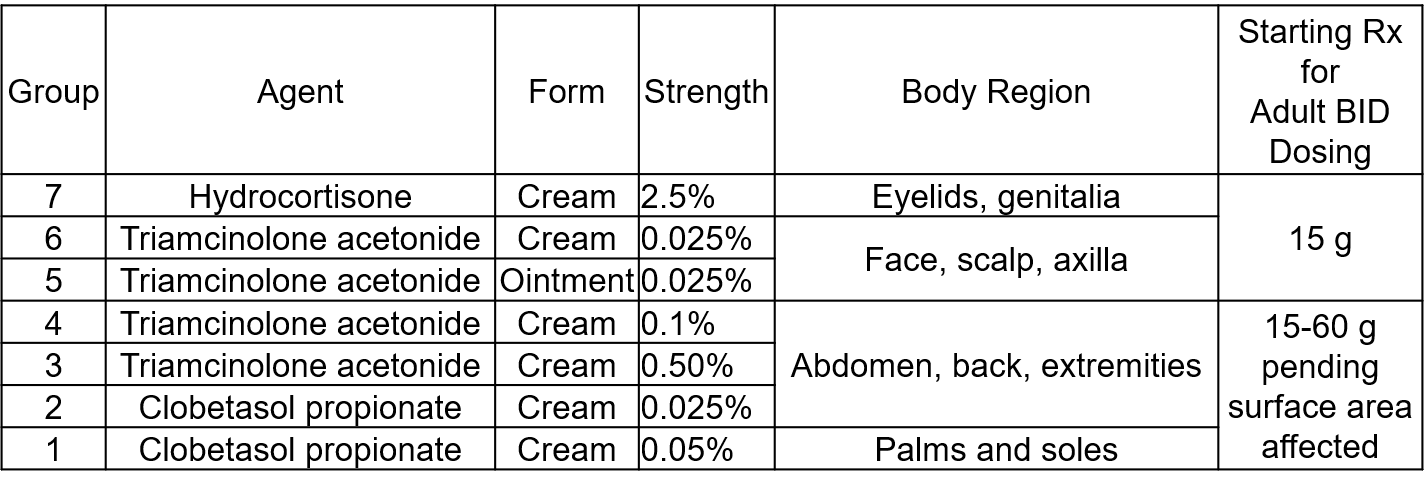
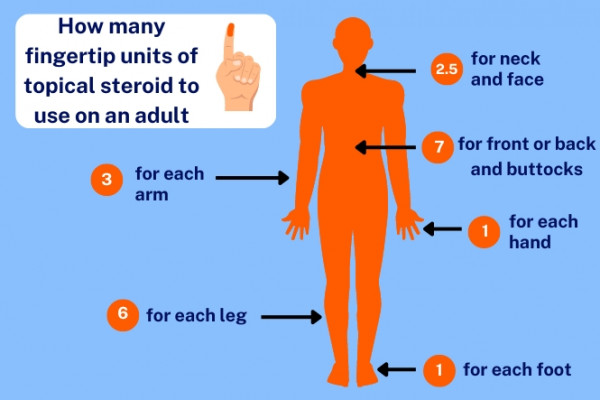
How do you approach choosing a topical steroid?
100
This is the typical description and locations (name 3) of chronic plaque psoriasis, the most common form of the chronic skin condition
symmetrically distributed cutaneous plaques with common sites including the extensor elbows, knees, scalp, and gluteal cleft. Plaques are well demarcated and erythematous usually with a thick silvery scale on the plaque.


100
Name 3 risk factors for and 3 common sites of skin tags
Risk Factors:
-Age
-Obesity
-Diabetes/Insulin Resistance
Common sites - usually sites of friction:
-neck
-axillae
-inguinal region
200
Name 4 exacerbating factors for rosacea
temperature changes, sun exposure, hot liquids, spicy foods, alcohol, exercise, extreme emotion, irritation from topical products, certain vasodilator meds
Main features of Rosacea:
-classic phenotype - centrofacial erythema (nose, medial cheeks). can include papules and pustules, flushing, telangiectasias
-less common - phymatous changes w/ tissue hypertrophy

200
What are the treatment indications for this condition?

Bonus: Who should be vaccinated?
This is shingles. Treatment is Valacyclovir administered as follows:
-immunocompetent- within 72 hours of onset, perhaps longer window in those >65, with lesions in dangerous locations (ex: face), new lesions still coming after 72 hours
-immunocompromised- option to start treatment anytime after onset. consider IV therapy for those at highest risk for dissemination (transplant, neutropenic, etc)
vaccination: immunocompetent > 50, anyone >18 actively or will be immunocompromised
200
Your 20 year old patient calls in with earlobe pain and redness 2 days after getting her ear pierced. She notes that if she puts pressure on the lobe, a small amount of milky material comes out of the new hole. What do you recommend and what topical agent might you prescribe?
1) Remove piercing (could in theory put a loose suture through the hole to keep it patent)
2) Wash thoroughly
3) Infected lobe piercings are likely due to skin flora- staph (including MRSA), strep, etc. You might be able to get away with an OTC antibiotic ointment but the most effective option here is Mupirocin (Bactroban) for a few days. Covers all of the skin flora including MRSA.
200
This Type IV hypersensitivity reaction can be described as an acute, intensely pruritic rash of papules, plaques, vesicles, and/or bullae often in a linear streak
Name the condition and how you treat it

Poison Ivy/Oak/Sumac! All due to the Urushiol oil released from the plant (alive or dead!). It is easily transmitted from plan to skin. The oil is an intense sensitizer so only 1 prior exposure is needed to generate an intense type IV reaction with the next exposure.
Treatment - steroids! Topical high or super high potency for limited mild-moderate disease, oral steroids for more severe or extensive disease. The earlier the better! Topical soothing measures (cold compresses, oatmeal baths, etc) can help with symptom management
NB: antihistamines don't help here despite the itching since this reaction isn't allergic/histamine mediated!
200
Name this lesion and how it should be managed:

Epidermoid Cyst - can be anywhere on the body and is skin colored.
Treatment:-if not inflamed or infected, no treatment is required! they can be remove for cosmetic reasons if the patient desires
-if inflamed but not infected, can inject steroid in it
-if infected, manage as you would any other abscess
300
Describe the common sites, appearance, and the 2 major treatment options for seborrheic dermatitis


Common sites - scalp, center of face, external ear, upper trunk, intertriginous areas
Appearance- well-demarcated, erythematous plaques with yellowish scale (dandruff) on areas rich in sebaceous glands
Treatment- main mechanism is local inflam reaction to normal skin fungi- treatments are EITHER topical antifungals or topical steroids!
300
name 2 other conditions on your differential for this condition. How you would treat this and what med should you NOT use

This is Tinea Corporis/Ringworm! note the raised border, some scaling, and central clearing.
DDx:
Granuloma Annulare - 
(no scale, wouldnt respond to antifungal)
Cutaneous Lupus-
can be one or multiple, usually on sun-exposed skin
Treatment of Ringworm - any topical AZOLE. This is TINEA, not CANDIDA so no Nystatin!
300
You are seeing a young patient for management of mild acne. The acne isn't new or different but they would like to try a topical agent for management. Their acne looks like this:


What would you recommend as first line treatment and how would you advise her to apply it?
This is COMMEDONAL ACNE - just whiteheads/blackheads without any inflammatory component or scarring.
Classes of acne treatment include:
-Retinoids
-Antibiotics
-Anti-inflammatories
-Hormonal treatments
Escalating doses and multi-agent regimens might be used for papulopostular/inflammatory acne but this patient just has mild commedonal acne for which the first line treatment is a RETINOID
Retinoids- well tolerated, work well at reducing follicular hyperkeratosis and prevent the formation of comedones.
Options include- Tretinoin (Retin-A), Adapalene (the only OTC one! Brand Differin), Tazarotene
-apply pea-sized amount nightly to whole face on dry skin. Main AE is skin irritation/flaking/redness which can occur in the first month, if that happens can start with lower potency or QOD.
300
This chronic and recurrent condition of hyperproliferative melanocytes is most commonly seen in women of reproductive age. It usually appears as irregular brown patches and macules on sun exposued skin. Many studies have demonstrated a psychologically devastating effect on QOL.

This is MELASMA - often there is a familial association, especially in 1st degree relatives. UV light clearly as a role with the incidence highest in the tropics. Hormones are implicated as well with occurrences after discontinuing OCPs, during pregnancy, menopause, or with HRT.
Treatment often includes topicals that inhibit melanin production or skin lighteners.
300
These are the two first line treatments for warts
1) Salicylic Acid - exfoliates the epidermis and may stimulate local immunity. lots of strengths and formulations (liquid, ointment, pads, etc), many of which are OTC. Takes weeks!
2) Cryotherapy- liquid nitrogen freezes the wart tissue causing thermal injury and triggering local immune response. Can cause irritation and discomfort that may take a few days to resolve
400
We see a lot of contact dermatitis but there are different types! Here is a 3 part question about irritant and allergic contact derm:
1) Acute Allergic and Irritant Contact Derm can look the same - describe 2 physical exam findings that you might see in both
2) The symptoms may be different, though! What main symptom might you see in each condition?
3) How would you treat the conditions?
A quick note:
-allergic contact derm requires prior sensitization so typical exposures are things like nickel (jewelry), plants (poison ivy), and topical skin products.
-irritant contact derm doesn't require sensitization so it's often physical/chemical exposures - wet work, solvents, acids, wood, fiberglass, industrial detergents, etc.
1) edema, erythema, vesicles

2) irritant - pain/burning, allergic- itching
3) usually emollients/moisturizers and super high/high potency topical steroids. note: there is less evidence that topical steroids do anything for irritant contact derm since it's not as inflammatory but it's still often/usually used.
400
Name this condition, the typical symptom(s), first line treatment(s), and what guidance you might give to the patient about transmission and expected course
Tinea Versicolor - note, this is a bit of a misnomer since the culprit organism is Malassezia, a yeast, not a dermatophyte
typically asymptomatic!
first line treatment - topical AZOLE or TERBINAFINE
counseling- not contagious (90-100% of people have Malassezia normally on our skin!), often recurs, can take weeks to resolve AFTER completing appropriate treatment
400
You notice that a patient with eczema on their neck is refilling their medium-potency steroid cream pretty regularly. When you inquire about this they say it's the only thing that works and the only thing they've ever tried! In addition to counseling about behavioral changes that might help (emollients, humidifiers in the winter, etc) what alternative topical agent should you prescribe to reduce the frequency of steroid use?


Topical Calcineurin Inhibitor! These include:
-Pimecrolimus
-Tacrolimus
Tacrolimus is probably a bit stronger than Pimecrolimus, equivalent to a ~medium potency steroid.
They are immunomodulators that do not cause any of the nasty side effects of steroids, notably skin thinning. Can cause some skin burning for very active lesions so might want to cool off with steroid for a few days then start Calcineurin Inhibitor
400
A patient sends you a mypennmedicine message about intense itching, especially at night around their wrists and fingers. The only skin findings are those made from their nails from scratching so much. They live with 1 child who had similar symptoms the week prior.
Name this condition, how to treat it (be specific), and counseling you should give them about their child.
This is classic scabies!
First line treatment is PERMETHRIN cream. This shouldn't just be applied to the affected area. The mites can be in many locations so the cream should be applied from the neck down covering as much surface area as possible. This is usually done twice, one week apart, to ensure the mites are eliminated.
Counseling - all close/household contacts should be treated regardless of whether they have active symptoms. Symptoms take weeks to develop so you want to break the cycle of reinfection.
400
What lab workup might you consider for non-specific hair loss/thinning?
Perhaps none, but for generalized hair loss/thinning (AKA not a clear diagnosis such as MPHL or Alopecia Areata) the derm societies recommend checking CBC, Ferritin/iron studies, Vit D, and TSH.
The caveat, though, is that there is insufficient data to say that supplementing D or Fe in those who are deficient actually does anything.
500
Name this condition, a variant presentation of a more common dermatologic entity, and how you would treat it. Hint: this is the opposite of the normal presentation despite being the same condition


This is INVERSE PSORIASIS - involves intertriginous areas and is often mistaken for fungal dermatitis. it is the opposite of the typical presentation of psoriasis
key differentiating features from candidal intertrigo - intertrigo may have nearby satellite lesions, inverse psoriasis patients may have a personal or family history of psoriasis, location may help in some scenarios
treat with topical steroid! that wouldn't be the TOC for candidal intertrigo so it's worth knowing the difference!
500
1) Name this condition
2) What are your treatment options?
3) How do you decide amongst those options?

1) Onychomycosis - dermatophyte infection of nail
2) treatment options include oral terbinafine or various topical options including topical azoles (Eficonazole) or Ciclopirox that are in vehicles that penetrate the nail (lacquers for example)
3) options depend on PERCENT OF NAIL INVOLVED and DISTRIBUTION OF THE NAIL INVOLVED
-distal and <50%? topical OR oral could be an option
-proximal (involving nail bed) or >50%? oral only
500
A patient sends you a MyPennMedicine message saying that they cut their finger on their car's tailpipe while washing the car. You can see in the chart that they are up to date on their TdaP booster. After cleansing the wound with soap and water they are wondering about any OTC treatments that would help prevent and/or treat infection. What 2 OTC options could you recommend? BE SPECIFIC
1) Petroleum Jelly (Vaseline)!
2) Triple Antibiotic - Bacitracin (gram +), neomycin (gram -), and Polymyxin B (gram -). Brand name is NEOSPORIN
-NOTE: there are single and double OTC antibiotic ointments too (bacitracin, Polysporin aka bacitracin/polymyxin B)
-They are basically equally effective! Head-to-head studies of Vaseline vs. Triple Antibiotic have not shown one to be markedly superior to the other and more Triple Antibiotic users can get local allergic reactions
500
Name 3 of the most common causes of hair loss (that Lauren wanted you to choose :) ) and the general treatment approach for each
1) Telogen Effluvium - acute, usually in response to a stressor. abnormal shift in follicular cycling that leads to hair loss. Tx - fix underlying cause (if possible, like nutritional issue), psychological support, supportive care
2) Alopecia Areata- depends on area involved, for areas like below, usually intralesional corticosteroid injection or topical high potency steroid because this is immune-mediated

3) Male/Female Pattern Hair Loss (Androgenetic alopecia)- frontal scalp and vertex hair loss, chronic and progressive. likely related to effect of androgens.
-men - oral finasteride, topical minoxidil
-women - oral or topical minoxidil +/- spiro
minoxidil - poorly understood but likely increases growth phase and shortens the telogen/resting phase of hair follicles
500
Name this skin lesion in an asymptomatic patient.


These are Dermatofibromas- one of the most common cutaneous lesions. They appear usually in the 20-40 age range and are asymptomatic. They grow minimally or extremely slowly. They are thought to be reactive secondary to local trauma, bites, etc.
Note these might be confused for a neoplastic process - take a good history about growth, location, etc to avoid unnecessary eval as these are completely benign.