Pathophys
Clinical Presentation
Labs/Diagnostics
Treatment
Ethics/Spicy
100
A patient with long-standing untreated celiac disease is most likely to have which of the following laboratory findings?
A. Elevated serum triglycerides
B. Macrocytic anemia due to B12 deficiency
C. Prolonged PT due to vitamin K deficiency
D. Hypercalcemia due to vitamin D toxicity
E. Hyperalbuminemia due to dehydration
Answer: C
Fat-soluble vitamin malabsorption includes A, D, E, and K.
K → ↓ clotting factors → ↑ PT
100
A 29-year-old woman presents with fatigue, bloating, and chronic diarrhea. She reports unintentional weight loss and frequent pale, greasy stools. Physical exam reveals pallor and mild proximal muscle wasting. Labs show iron deficiency anemia and low vitamin D.
Which of the following combinations of symptoms is most consistent with untreated celiac disease?
A. Fever, right lower quadrant pain, bloody diarrhea
B. Chronic diarrhea, weight loss, iron deficiency anemia
C. Hematemesis, abdominal pain, macrocytic anemia
D. Postprandial abdominal pain, gallstones, jaundice
E. Diarrhea, tenesmus, urgency, and mucous in stool
Correct Answer: B. Chronic diarrhea, weight loss, iron deficiency anemia
This triad reflects classic celiac disease due to malabsorption from villous atrophy affecting iron, fat, and caloric absorption.
100
Fill in the blanks with expected CBC findings in celiac disease and explain your answers.
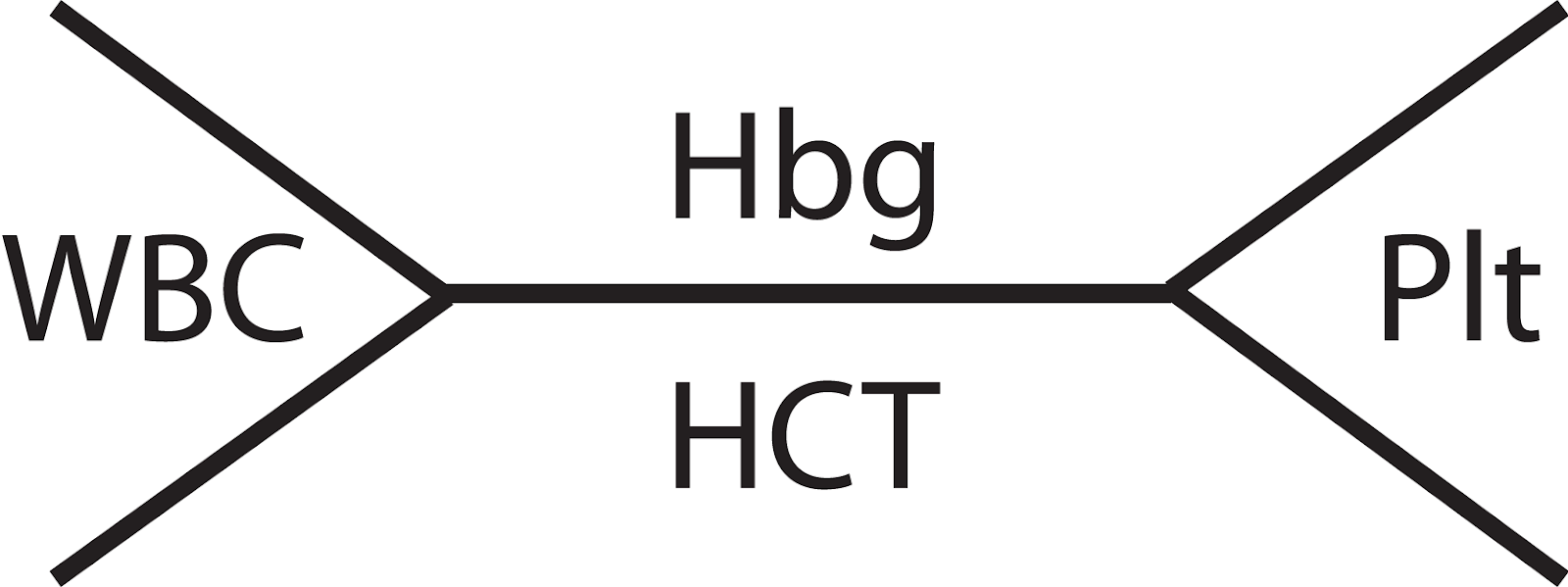
WBC: normal
Hbg: decreased
Hct: decreased
Plt: increased
In celiac disease, the most common CBC finding is anemia, often microcytic due to iron deficiency from impaired absorption in the proximal small intestine. Hemoglobin and hematocrit are typically low, and the MCV will decreased in anemia from iron deficiency or inflammation. Thrombocytosis can be seen as a reactive response to anemia or chronic inflammation. These hematologic abnormalities may be the first sign of silent or atypical celiac disease.
100
Which of the following foods should a patient with celiac disease strictly avoid?
A. Corn
B. Rice
C. Wheat
D. Quinoa
C. Wheat
Explanation: Wheat, rye, and barley are all grains that contain gluten, which trigger the immune response in individuals with celiac disease. A gluten-free diet is the only definitive treatment, and avoiding it all together is the only way to prevent an autoimmune reaction to gliadin proteins found in gluten.
100
Gluten-free foods can be up to _________ more expensive than regular food options.
A. 23%
B. 87%
C. 115%
D. 183%
D. 183%
200
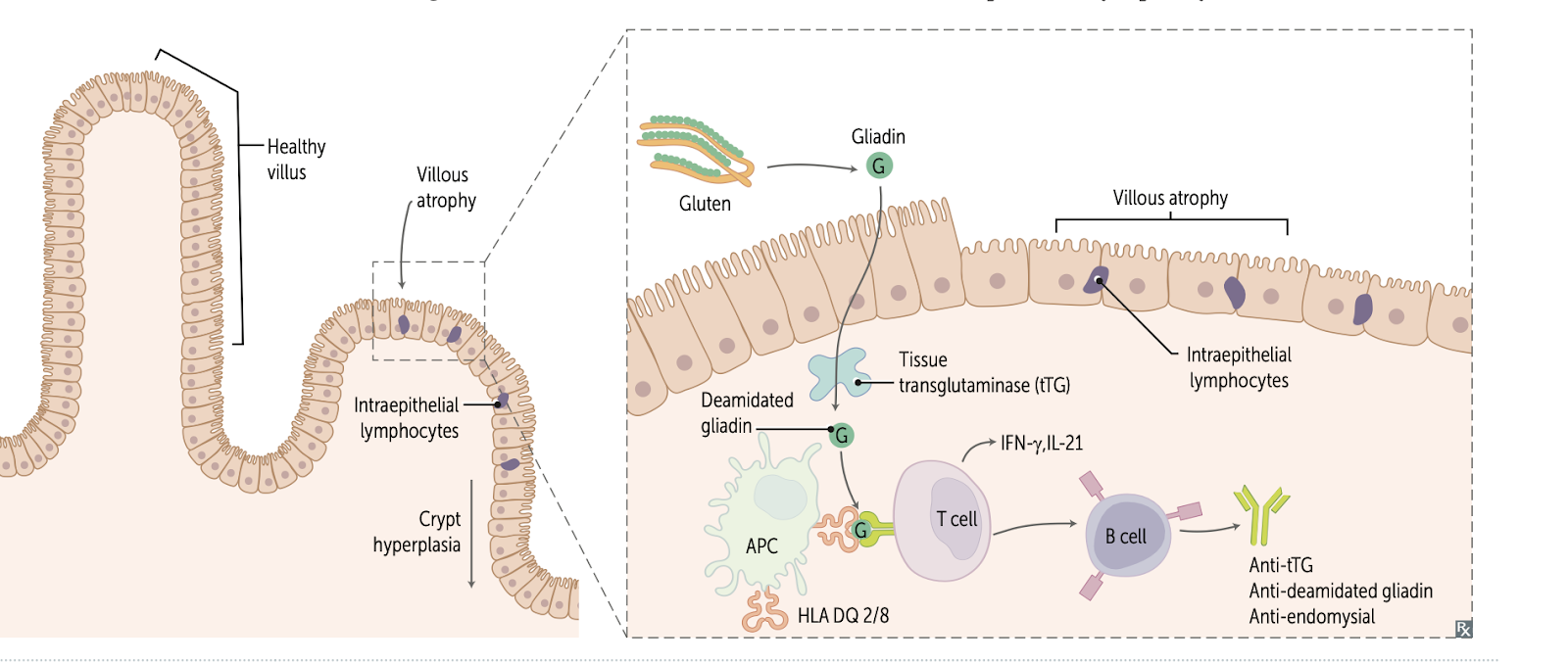
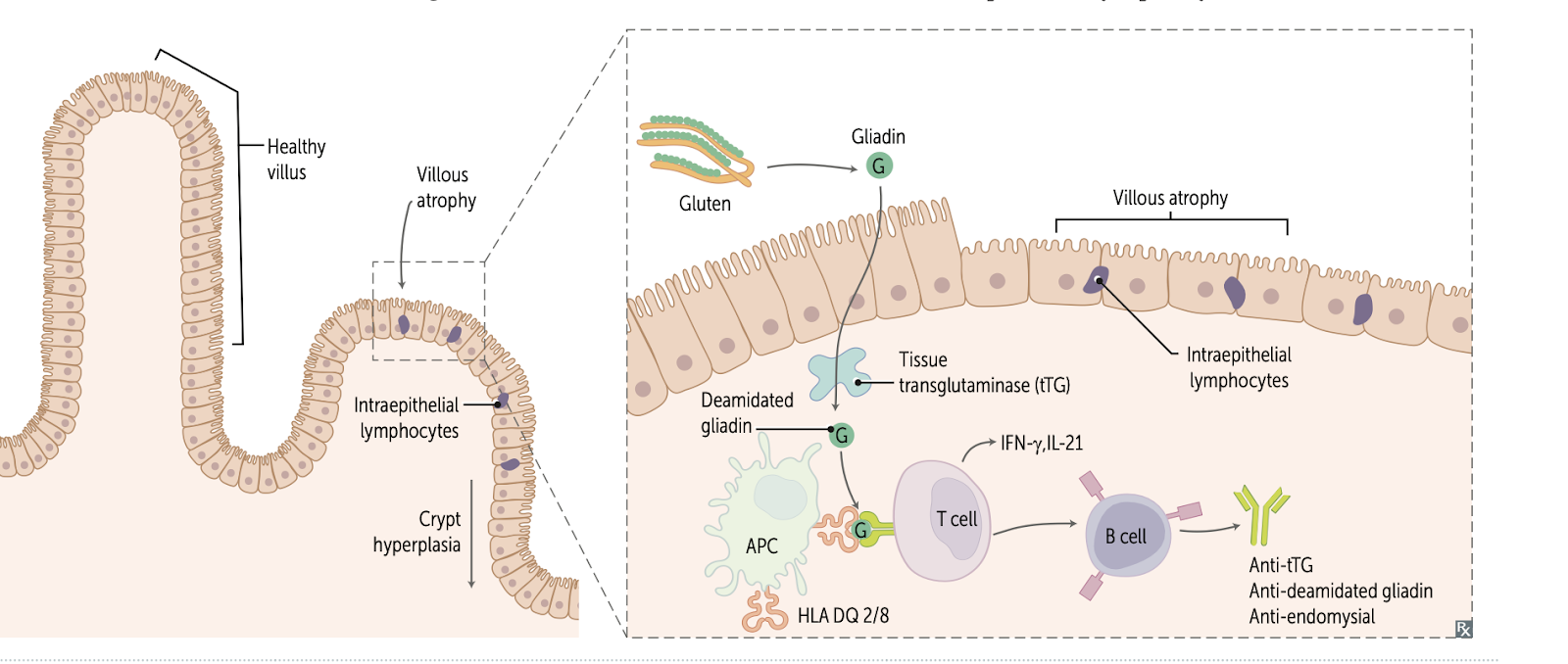
Match the sequence of pathophysiological events that occur after gluten ingestion in a patient with Celiac's
A. CD4+ T cells activate, releasing cytokines
B. Gluten crosses epithelium via transcytosis
C. Villous atrophy, crypt hyperplasia, lymphocytosis
D. Deamidated gliadin binds HLA-DQ2/8 on APCs
E. Tissue transglutaminase deamidates gliadin
F. IFN-γ and TNF-a release
1. B. Gluten crosses epithelium via transcytosis
2. E. Tissue transglutaminase deamidates gliadin
3. D. Deamidated gliadin binds HLA-DQ2/8 on APCs
4. A. CD4+ T cells activate
5. F. IFN-γ and TNF-α release
6. C. Villous atrophy, crypt hyperplasia, lymphocytosis
200
A 40-year-old woman presents with fatigue, bloating, and chronic diarrhea. She has lost 15 pounds over the past 4 months despite a normal appetite. Labs show microcytic anemia, low vitamin D, and low albumin. Stool studies are positive for fat. Duodenal biopsy shows villous blunting and increased intraepithelial lymphocytes.
Which of the following best describes the type of malabsorption seen in this patient?
A. Selective malabsorption due to specific enzyme deficiency
B. Global malabsorption due to widespread mucosal damage
C. Post-absorptive malabsorption due to lymphatic obstruction
D. Primary congenital malabsorption due to genetic transporter defects
E. Acquired malabsorption due to ileal inflammation
B. Global malabsorption due to widespread mucosal damage
Celiac disease = immune-mediated destruction of small intestinal villi → loss of absorptive surface → global malabsorption
Explains fat malabsorption (steatorrhea), micronutrient deficiencies (iron, vit D), and protein loss (low albumin)
200
A 25-year-old woman presents with fatigue and iron-deficiency anemia. You suspect celiac disease and order a tissue transglutaminase IgA (tTG-IgA) test. Which of the following best describes the sensitivity and specificity of the tTG-IgA test for diagnosing celiac disease?
A. High sensitivity but low specificity; positive in many GI disorders
B. High specificity but low sensitivity; useful for confirming the diagnosis
C. Both sensitivity and specificity are high, making it a reliable first-line screening test
D. Low sensitivity and specificity unless combined with anti-gliadin antibody testing
E. Sensitivity is only high in patients with dermatitis herpetiformis
Answer: The tTG-IgA test has a sensitivity and specificity >90% (often quoted around 95–98%) for untreated celiac disease when total IgA levels are normal. It’s considered the first-line serologic test. If IgA deficiency is present, tTG-IgG or DGP-IgG may be used instead
200
Use the whiteboard to explain the mechanism of action of dapsone, and why it was used to treat Mrs. Townsend’s rash.
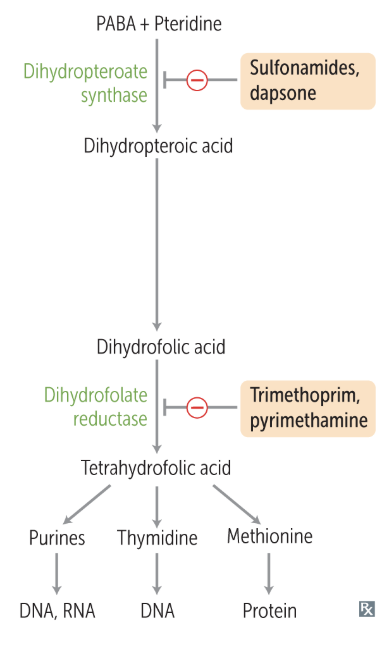
Explanation: Dapsone is an antimicrobial agent that inhibits the enzyme dihydropteroate synthase, which converts PABA + pteridine into dihydropteroic acid. This is an important precursor step for the synthesis of dihydrofolic acid in bacteria, which TMP/SMX and other sulfonamides act on. In our case specifically, dapsone is used as an anti-inflammatory agent, inhibiting neutrophil function and recruitment. Dapsone is used for rapid relief of symptoms (days) while a patient begins transitioning to a gluten-free diet.
200
Name a few examples of indirect costs associated with the management of chronic conditions like celiac disease.
Explanation: Lost wages, travel costs, emotional stress, and lower quality of life are all examples of indirect costs that affect patients dealing with chronic conditions. These factors are exacerbated when the patient is uninsured, like Mrs. Townsend. These patients have to also then consider what treatment/testing they can afford, and whether they can pay for constant appointments out of pocket.
300
An individual with chronic diarrhea and positive anti-endomysial antibodies is found to have a high expression of HLA-DQ2. What is the role of HLA-DQ2 in this disease process?
A. Presents deamidated gliadin peptides to CD8+ T cells
B. Enhances B cell class switching to IgA
C. Presents deamidated gliadin peptides to CD4+ T cells
D. Activates innate immune responses to gluten
E. Causes T cell–independent epithelial apoptosis
Answer: C.
APCs present deamidated gliadin peptides on HLA-DQ2/8 to CD4+ T cells in the lamina propria → cytokine release → mucosal damage.
300
You're a third-year medical student on your family medicine rotation in Pilot Point, Texas. You’re seeing a 34-year-old woman with known celiac disease who’s complaining of muscle cramps, tingling in her hands and face, and new-onset fatigue. She’s been non-adherent to her gluten-free diet and has had chronic diarrhea for the past few months.
Unfortunately, your phlebotomist didn’t show up today, and the lab system is down (classic rural med life). You still suspect hypocalcemia due to vitamin D deficiency from ongoing malabsorption.
You’re working with a fabulous clinical team from the Burnett School of Medicine at TCU 🐸💜 — and you need to think fast.
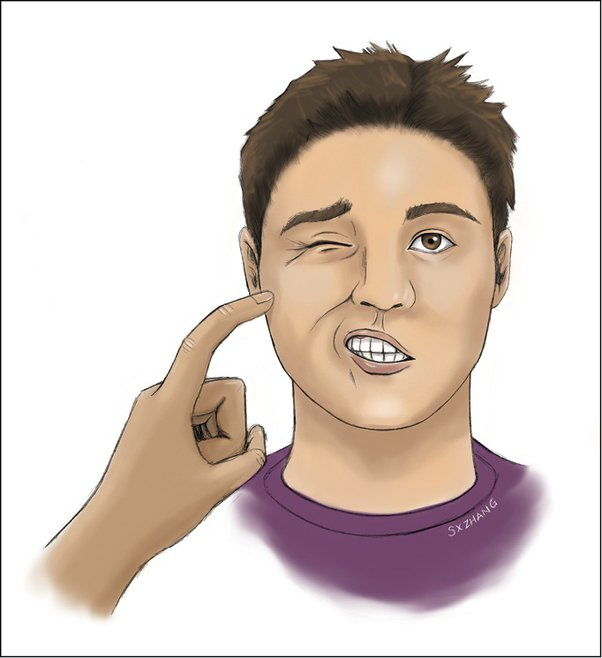
Without access to labs, what two bedside physical exam tests can you perform in the clinic to assess for hypocalcemia in this patient? Please perform the test on a teammate and for full credit your teammate must act out the expected finding.
Chvostek’s Sign
→ Tap the facial nerve just anterior to the ear (near the angle of the jaw).
→ A positive sign is twitching of the ipsilateral facial muscles, indicating neuromuscular irritability from low calcium.Trousseau’s Sign
→ Inflate a blood pressure cuff on the arm above systolic pressure for 3 minutes.
→ A positive sign is carpopedal spasm (wrist flexion, MCP flexion, IP extension), also due to neuromuscular excitability from hypocalcemia.

300
A 32-year-old man presents for evaluation after a recent routine blood test showed elevated ALT and AST. He has no symptoms, drinks alcohol occasionally, and has no significant past medical history. Hepatitis B serology is ordered and reveals the following:
HBsAg: positive
Anti-HBs: negative
Anti-HBc (total): positive
Anti-HBc (IgM): negative
HBeAg: negative
Anti-HBe: positive
Which of the following best describes his current hepatitis B status?
A. Acute hepatitis B infection
B. Chronic inactive hepatitis B carrier state
C. Resolved past hepatitis B infection
D. Vaccinated against hepatitis B
B. Chronic inactive hepatitis B carrier state
This serologic profile shows positive HBsAg and positive anti-HBc total, indicating chronic infection. The negative IgM anti-HBc rules out acute infection, and the positive anti-HBe with negative HBeAg suggests a low replicative phase — often called the inactive carrier state. ALT elevation could be mild and non-specific here, but ongoing monitoring is essential to detect reactivation.
300
List three long-term consequences/complications of not following a gluten-free diet in celiac disease, and explain why they occur.
Explanation:
Enteropathy-associated T-cell lymphoma (EATL) - chronic inflammation and exposure to antigens promotes clonal expansion of increased intraepithelial lymphocytes (IELs), which increase the risk of developing lymphoma.
Osteomalacia - long-term malabsorption of vitamin D can lead to weakening of bones, bone pain, and increased risk of fractures. Mrs. Townswend already displayed mild levels of vitamin D deficiency.
Iron-deficiency anemia - similar to osteomalacia in that the underlying cause is malabsorption due to celiac disease. Long-term iron deficiency can lead to fatigue, pallor, tachycardia, and increased risk of infection.
300
Which of the following foods would you need to double-check before recommending it to a celiac patient?
A. Rice
B. Plain potatoes
C. Soy sauce
D. Grilled chicken breast
C. Soy sauce
Many soy sauces contain wheat unless labeled gluten-free.
400
Fill in the blank:
Celiac disease causes damage to the __________ and __________ of the small intestine, leading to __________ of the intestinal villi. This results in decreased __________ area for absorption.
Iron is primarily absorbed in the __________ portion of the small intestine, which is one of the earliest and most severely affected regions in celiac disease.
As a result, patients may present with __________ anemia, characterized by a __________ mean corpuscular volume (MCV) and often accompanied by __________ on CBC.
Celiac disease causes damage to the duodenum and proximal jejunum of the small intestine, leading to blunting of the intestinal villi. This results in decreased surface area for absorption.
Iron is primarily absorbed in the duodenum, which is one of the earliest and most severely affected regions in celiac disease.
As a result, patients may present with microcytic anemia, characterized by a low mean corpuscular volume (MCV) and often accompanied by low hemoglobin on CBC.
400
On the board, write the pathophysiologic mechanism and a histological finding for why we see a rash in Celiac patients.
*Bonus: include the proper name of this rash*
Pathophysiology: B-cells activated by T cells produce IgA antibodies against epidermal transglutaminase. These antibodies deposit in dermal papillae causing a gross rash on extensor surfaces.
Histology: Deposits of IgA at tips of dermal papillae
400
A 28-year-old woman presents with chronic diarrhea, bloating, and weight loss. Her labs reveal iron deficiency anemia and low folate levels. Serologic testing shows positive anti-tTG IgA antibodies. An upper endoscopy is performed to confirm the diagnosis. Which of the following endoscopic findings is most commonly associated with celiac disease?
A. Cobblestoning and skip lesions in the terminal ileum
B. Villous atrophy with scalloping of the duodenal folds
C. Thickened gastric folds with nodularity
D. Patchy mucosal erythema and exudates in the jejunum
E. Normal-appearing mucosa with normal biopsies
B. Villous atrophy with scalloping of the duodenal folds
In celiac disease, upper endoscopy may reveal changes in the duodenum such as scalloping of the folds, loss of mucosal folds, mosaic pattern, and villous atrophy (confirmed on biopsy). These changes result from chronic immune-mediated injury. While sometimes subtle or even normal to the naked eye, biopsy of the duodenum remains the gold standard for diagnosis. Other options listed reflect findings seen in Crohn’s disease (A), gastritis or lymphoma (C), infectious or inflammatory jejunitis (D), or could be misleading (E) in early or patchy disease.
400
Mrs. Townsend is here for a follow-up on her new gluten-free diet. She brought along a receipt from her recent grocery trip and asks you for help identifying which items she can safely eat. Which of the following items do not contain gluten?
A. Clif Bar
B. Great Value frozen broccoli
C. Twizzlers
D. Kikkoman soy sauce
E. Mentos chewy mints
Explanation: All of these items contain gluten! Many common grocery store items contain gluten without it being explicitly labeled on the product.
Clif Bar - contains barley malt extract and may contain wheat.
Great Value Frozen Broccoli - has warning label that it may contain traces of wheat (cross-contamination).
Twizzlers - contains enriched wheat flour.
Soy Sauce - third main ingredient is wheat.
Mentos - second ingredient is wheat syrup, maltodextrin also a source of gluten.
400
Pick one of the ethical pillars of healthcare (autonomy, beneficence, non-maleficence, and justice) and explain how it relates to Mrs. Townsend’s experience as an uninsured patient.
Autonomy - Mrs. Townsend autonomy was limited by her lack of insurance at the beginning of our case; while willing to do whatever she needed to get better, she was limited to certain tests/procedures that she could feasibly pay out-of-pocket. Picking treatment and management based on what she can afford inherently limits her autonomy to make choices for herself.
Beneficence / Non-maleficence - Physicians always have a duty to not cause harm and reduce risk to patients. This is especially true in caring for uninsured patients; we as physicians have to be especially cognizant that the options provided to uninsured patients are reasonable without adding unneeded financial burden. We may get used to ordering additional tests to cover our bases, but when patients can’t afford them it can affect our decision making and increase the risk of something being missed.
Justice - Mrs. Townsend is unable to be treated as an equal to other insured patients, as other patients’s care is not limited by what they can afford 100% out-of pocket. By nature Mrs. Townsend care is different; I don’t think it was lesser than in our PIBL case, but we can’t deny her experience was different and/or unequal to that of an insured patient in a similar situation.
500
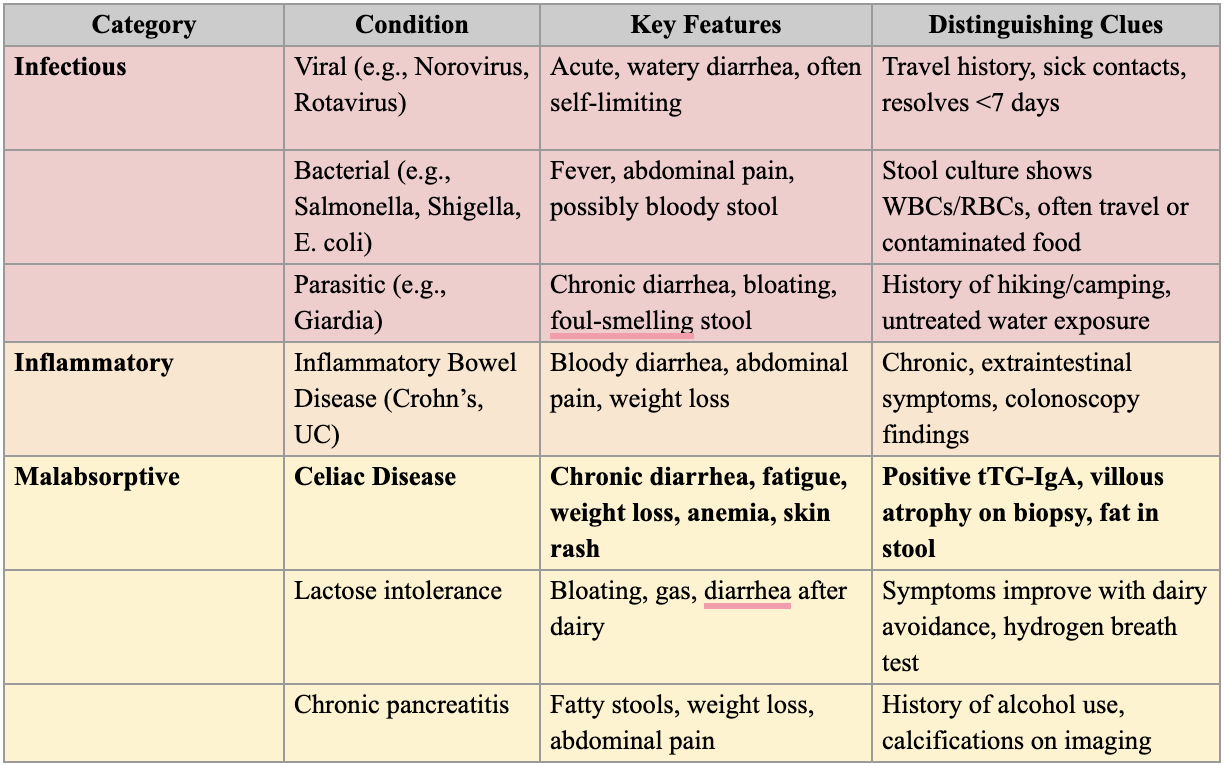
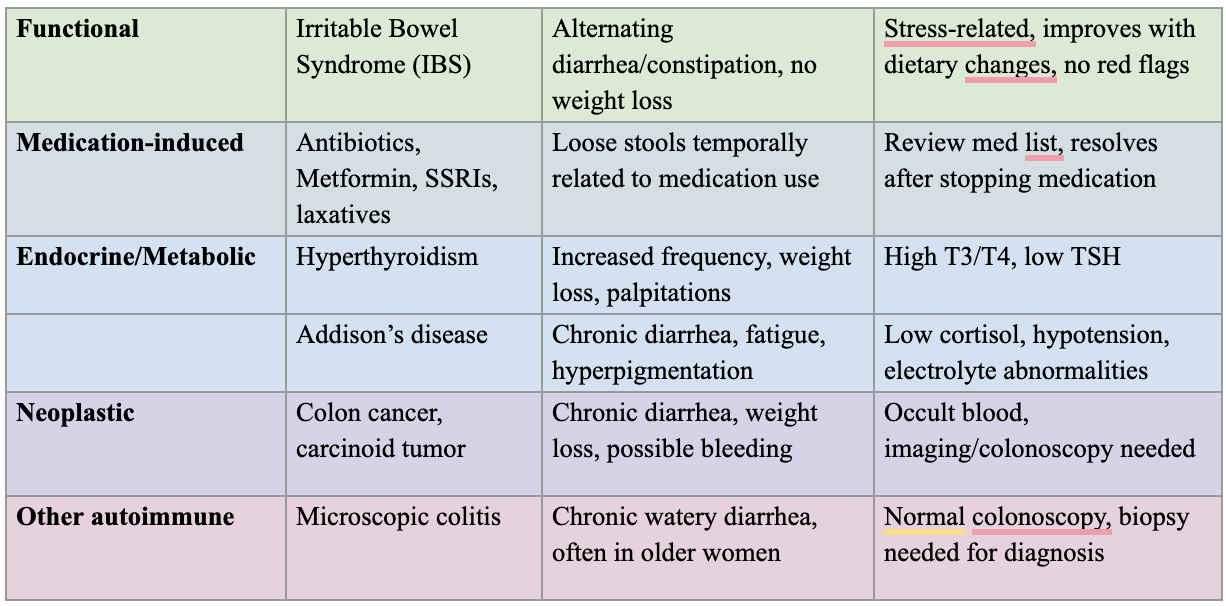
List four possible causes of chronic diarrhea that were considered in the differential, and explain briefly why each was ruled out.
500
Your patient returns to the clinic with a history of Celiac disease. She has a history of not following a gluten-free diet. You prepare to perform a physical exam. Which physical exam findings should you look out for? Try to give at least 4
Pallor → Suggests iron deficiency anemia due to impaired absorption in the duodenum
Glossitis or angular cheilitis → Indicates iron or folate deficiency
Koilonychia (spoon nails) → Another sign of iron deficiency
Dermatitis herpetiformis (itchy, vesicular rash on elbows/knees) → Indicates IgA deposition in skin, classic for celiac
Easy bruising → Suggests vitamin K deficiency from fat malabsorption
Bone tenderness (e.g., shins, ribs) → Due to vitamin D deficiency, leading to osteomalacia
Positive Chvostek’s or Trousseau’s sign → Reflects hypocalcemia secondary to vitamin D malabsorption
Proximal muscle wasting or weight loss → From generalized malnutrition
500
One rep from each team races to draw the villus structure before and after celiac disease, labeling:
Enterocytes
Goblet cells
IELs
Crypts
Blunted villi
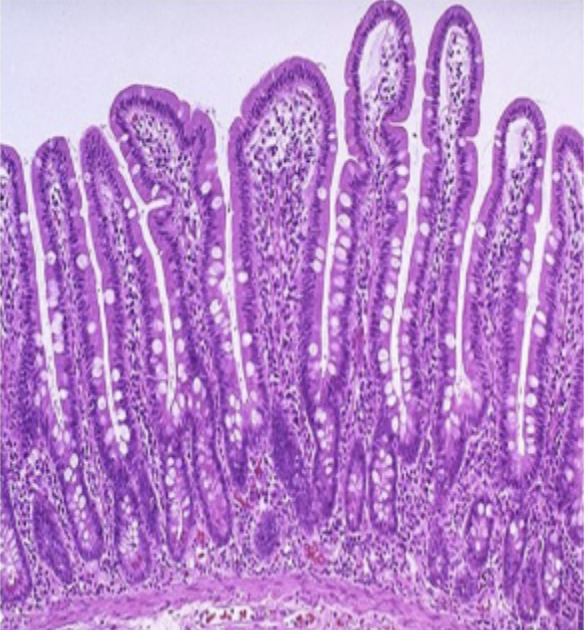
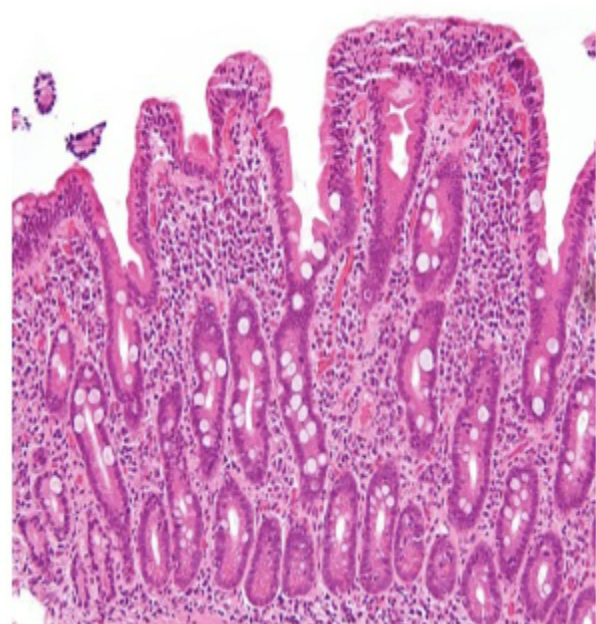
The chronic inflammation from CD4 T cells damages the small intestinal mucosa, leading to blunted villi. This is the flattening of the villi, which reduces absorptive surface area. Villous atrophy causes an increase in the depth of crypts with more goblet cells at the base of the villi, along with increased epithelial lymphocytes as a result of the inflammatory response to gliadin.
500
A 26-year-old woman presents to her primary care physician with chronic fatigue, intermittent diarrhea, and a 10-pound unintentional weight loss over the past 6 months. She also reports increased bruising and tingling in her feet. Her past medical history is unremarkable. Physical exam shows pallor of the conjunctiva and oral mucosa. Testing reveals a positive anti-tissue transglutaminase IgA test and blunting of villi on biopsy.
Which of the following is the most appropriate next step in the management of this patient?
A. Start short-term course of prednisone
B. Recommend over-the-counter antacids
C. Refer to registered dietician for lifestyle changes
D. Recommend lactose-restricted diet
C. Refer to registered dietician for lifestyle changes
Explanation: The best option would be to refer to an RD to help the patient navigate lifestyle changes required for celiac disease, mainly a gluten-free diet. An RD can help the patient navigate what foods to eat and avoid, how to implement gluten-free alternatives into her diet, and provide additional education and support of how to live with celiac disease.
500
During a discussion about barriers to care, a student asks how much it typically costs to diagnose celiac disease in the U.S. without insurance. Which of the following best represents the estimated total out-of-pocket cost for the full diagnostic process, including consultations, serology, genetic testing, and endoscopy with biopsy?
A. $200–$500
B. $500–$1,200
C. $1,600–$4,600
D. Over $10,000
E. The cost of giving up bread for life (priceless)
C. $1,600–$4,600
The average total cost of diagnosing celiac disease without insurance can range from $1,626 to $4,614. This includes:
Primary care visits
Blood tests (e.g., tTG-IgA)
Genetic testing (HLA-DQ2/DQ8 if needed)
Upper endoscopy with small bowel biopsy, which is the gold standard for diagnosis.
This highlights the financial burden that can delay diagnosis, especially in uninsured or underinsured patients — a great point for sparking discussion on access to care and health equity.